

Translation of in situ neonatal high-fidelity simulation training: identification and mitigation of latent safety threats
This study aimed to use in situ high-fidelity neonatal simulation training to identify latent safety threats in various neonatal scenarios. Having identified the threats, we then developed and implemented system improvement actions to mitigate them. We translated what we learnt from the mitigation process to real-life events. In this way we hope to improve upon our efficiency, quality of care, and patient safety.
Charu Bhatia
Consultant Neonatal Medicine
charubhatia@nhs.net
Geraldine Mangan
Practice Development Facilitator,
Senior Neonatal Nurse
Jessie Mertalla
Senior Neonatal Sister
Ather Ahmed
Consultant Neonatal Medicine
Neonatal Unit, Lister Hospital, East and North Hertfordshire NHS Trust
Background
Simulation, as defined by Gaba, is: “A technique, not a technology, to replace or amplify real experiences with guided experiences that evoke or replicate substantial aspects of the real world in a fully interactive manner.”1 Simulation has been adopted in health systems and education with the aim to deliver high quality patient care and develop individual knowledge and technical and crisis resource management skills, along with team work.2,3
Besides education and training, simulation-based training is also used to identify latent threats, implement new equipment or processes, and target health outcomes. A systematic review of simulation-based learning shows that it is effective in preventing iatrogenic medical error and improving patient safety.4
Latent safety threats (LSTs) are defined as system-based threats to patient safety that can materialise at any time and often go unrecognised by healthcare professionals.5 The threats generally fall under the categories of:
- medicines
- equipment
- environment
- knowledge and skills
- crisis resource management skills/human factors.
Latent threats can be identified during in situ simulation training. Mitigation strategies for an individual LST identified in a simulated environment can strengthen patient safety by preventing such threats from being translated to a real-life scenario.6
Objectives
In this study, we aimed to probe our existing systems7 to identify any LSTs and implement a mitigation process. Our objectives were:
- To identify LSTs during multidisciplinary in situ neonatal simulation training sessions on the neonatal unit.
- To develop and implement an action plan to mitigate the LSTs, thus ensuring patient safety and improved quality of care.
- To demonstrate the mitigation of LSTs by repeating the scenarios during the post-implementation period.
- To demonstrate the translation of simulation-based learning into real events.
TABLE 1 and FIGURE 1 show the steps and processes we took to identify and mitigate the LSTs.
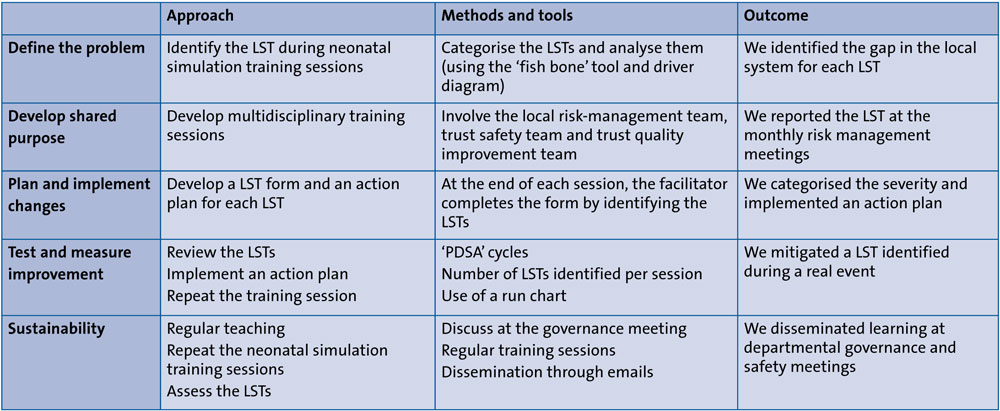
TABLE 1 Steps for the identification and mitigation of LSTs.
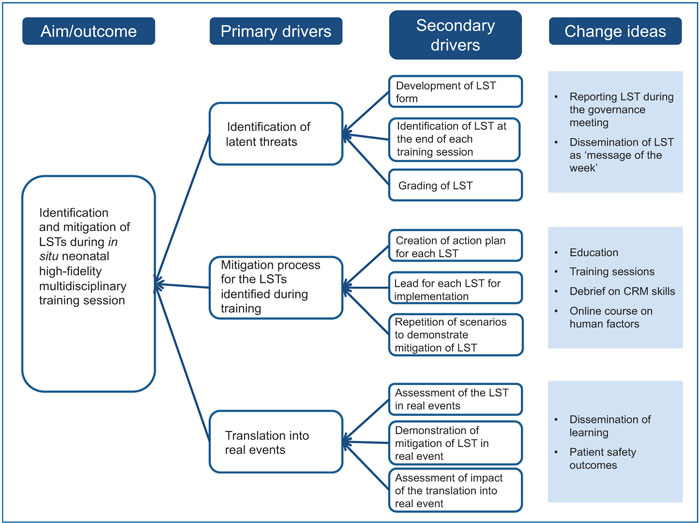
FIGURE 1 The driver diagram for the process of identifying and mitigating LSTs. Key: CRM=crisis resource management.
Methods
We have been conducting in situ neonatal high-fidelity simulation training at the Level 2 neonatal unit of Lister Hospital since 2014. The training is conducted at the unit in a dedicated area designed as the neonatal simulation room and undertaken with pre-prepared scenarios based on clinical events. The training involves a multidisciplinary team of two members of the medical staff, two nursing staff and two trained facilitators.
Since early 2019, we began to identify LSTs at the end of each training session, using a locally-developed LST form. For each LST, we implemented an action plan to identify system improvement actions to be taken by the neonatal multidisciplinary team to address and mitigate the LST.
TABLE 2 shows some of the scenarios used during the high-fidelity simulation training. Each scenario was based on recent events at the unit. Using an adapted Yorkshire Contributory Factors Framework,8,9 latent threats were differentiated into five main categories, namely: equipment, medication, technical, resources and crisis management skills/human factors.
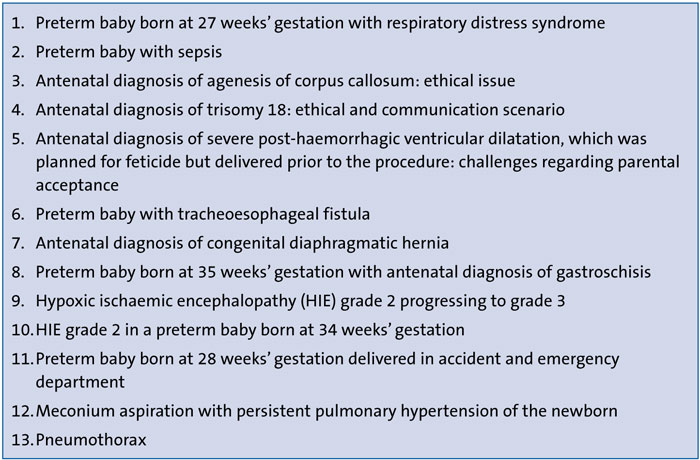
TABLE 2 Examples of scenarios used for in situ neonatal high-fidelity simulation training based on real events, 2019-2020.
Equipment: for example, equipment used not fit for purpose, incorrect use of equipment, lack of skill and knowledge of equipment and consumables.
Medication: for example, correct drugs, correct dose, timely administration, correctly prescribed, correct use of monograph.
Technical: for example, difficulty with clinical procedure, unfamiliar with procedure, knowledge deficit, skills deficit.
Resources: for example, correct use of guidelines/policies, protocol/monograph unclear or too complicated.
Crisis resource management skills/human factors: for example, team factors (conflicting goals, lack of respect, poor delegation, distraction, inexperience, insufficient staff, stress and fatigue, lack of situational awareness), communication (poor communication between staff, handover problems, escalation process not completed), leadership (inappropriate delegation, unclear responsibilities, lack of team supervision, failure to escalate, unreceptive to team views, prioritisation).
The latent threats were differentiated with respect to their severity using the RAG rating tool.10 An action plan was developed for individual LSTs and the person responsible for implementation was identified. The LSTs and the updates on implementation of the action plan were reported at the monthly departmental risk management meetings. The progress on implementation was reviewed fortnightly and information was disseminated at other meetings, including unit meetings and senior nursing meetings.
Since October 2019, we have been repeating the same scenarios in the simulation sessions and during debriefs. We continue to identify new LSTs and collect data to assess whether the previously identified LSTs have been mitigated.
We used two plan-do-study-act (PDSA) cycles. PDSA cycle 1 was used to identify the latent threats during the in situ high-fidelity simulation training and PDSA cycle 2 was applied to demonstrate the mitigation of the LSTs after the implementation of the action plan.
To demonstrate the translation of the simulation-based training and the mitigation of LSTs to real-life events, we collected data on the time taken to prescribe and administer medications, use of a Replogle tube, insertion of cerebral function monitor (CFM) leads and interpretation of amplitude-integrated electroencephalography (aEEG) during real-life scenarios.
Results
We conducted 22 multidisciplinary high-fidelity in situ neonatal simulation training sessions on the unit from January 2019 to December 2020, which included the post-intervention period. We trained a total of 88 neonatal staff, both medical and nursing staff in equal numbers. The breakdown of trainees was:
- specialty trainee grade 4-7 = 22%
- clinical fellows grade 1-2 = 26%
- General Practice Vocational Training Scheme = 7%
- nursing staff band 5-7 = 45%
A total of 67 LSTs were identified during this period, with an average of 3.0 threats per session. Other studies have found an average of 1.1 LST per session.11,12
The latent threats identified were categorised as:
- equipment = 22.3%
- medications = 17.3%
- technical = 19.4%
- resources = 12%
- crisis resource management skills = 29%.
TABLE 3 shows a sample of some of the LSTs and the mitigation processes.
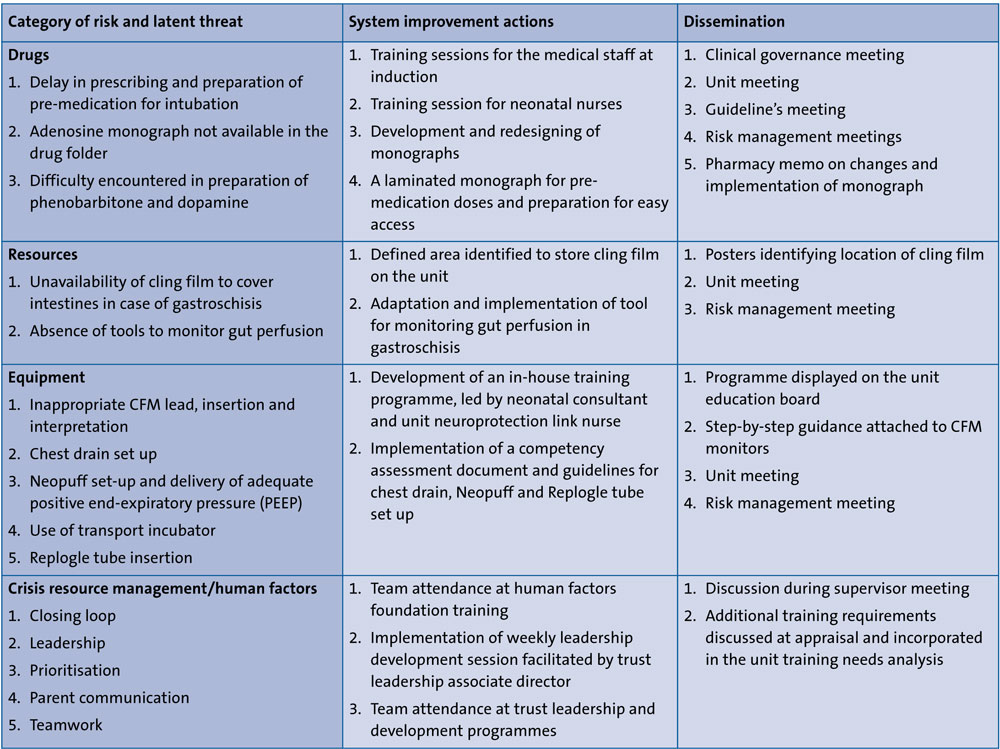
TABLE 3 Some examples of LSTs identified during the high-fidelity in situ simulation training and mitigation process.
Case study
An example of one of the LSTs identified is discussed. During a scenario, we identified a threat of delay in the prescribing and administration of pre-medication for intubation. The intervention process included:
- training sessions on prescription writing by a pharmacist for the medical staff at induction
- training session for neonatal nurses
- development of a laminated monograph for pre-medication doses and attachment of this to the intubation trolley.
We were able to demonstrate a post-intervention reduction in time for the prescription and administration of pre-intubation medication (FIGURE 2).
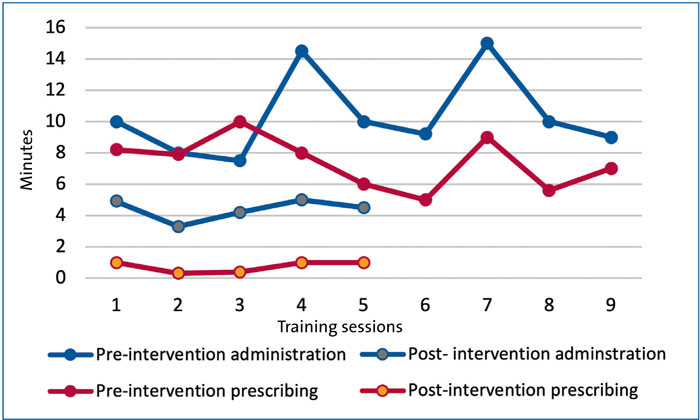
FIGURE 2 Mitigation of the threat of delay in administration of pre-medication for intubation.
Following the intervention process, we were able to demonstrate that we could mitigate most of the LSTs identified in our simulation training. We also attempted to demonstrate translation of the mitigated latent threats to real-life events. During a real event, the preparation and admin-istration of pre-medications prior to intubation, was timed and noted to improve in terms of reduced preparation and administration time (average time = 6.5 minutes). Translation of the training was also observed in:
- a reduction in the preparation time for phenobarbitone (from 14 to 5.6min), dopamine (from 15 to 8min), and adenosine (from 15 to 5min)
- appropriate insertion of a Replogle tube by neonatal nurses qualified in specialty (three events; 100% success)
- use of cling film and monitoring of bowel perfusion in gastroschisis (one event; 100% success)
- CFM lead insertion by neonatal nurses qualified in specialty (three events; 80% success)
- interpretation of CFM traces (three events; 70% success).
Discussion
In our study, we identified 67 LSTs during simulation training. We not only reported them during the risk management meeting, but also tested the efficacy of our system improvement by repeating the simulation training. We have also demonstrated the mitigation of some of the threats in real-life events.
Wetzel et al13 suggested that the improvement achieved after identifying LSTs during a multidisciplinary simulation training is the best objective evidence of the effectiveness of the training. Our study has not only provided this evidence, but is also one of the few studies to demonstrate the mitigation of latent threats identified during in situ simulation training, following the implementation of an action plan.
The scenarios in our high-fidelity simulations were based on real-life events. The advantage of using real-life events over standardised scenarios is that we can identify the existing LSTs in the system that could affect patient safety.14 We developed a robust process of mitigating the LSTs identified by implementing system-wide changes with the help of regular training for the medical and the nursing staff and a multidisciplinary approach.
We were able to identify an average of 3.0 LSTs per training session. LSTs per session reported in the literature vary between 0.8 and 1.8,11-13 and those most commonly reported relate to equipment and resources.11
The target of interventional translation simulation is to increase patient safety and improve the performance of the health service.15,16 We were able to translate some of our simulation-based learning to real-life events by assessing whether the LSTs identified were mitigated in clinical settings.3 However, some events are rare and it is important to note that the behaviour of participants in a simulation-based environment may not be reproducible in real life. The translation of the mitigated LSTs to real-life events was assessed at short intervals after the implementation of the changes in the system. Hence, we were unable to demon-strate the sustainability of our approach.
Conclusion
High-fidelity in situ neonatal simulation training should be used to identify and mitigate latent threats in a system; this will enable staff to deliver high quality care leading to improved patient safety.17,18
Author contribution
CB conceptualise this study and was responsible for writing the first draft of the manuscript. GM and CB designed the latent threat proforma. All authors facilitated the training sessions and contributed to the writing of the final version of the manuscript.
Or read this article in our
Tablet/iPad edition
- High-fidelity in situ neonatal simulation training on the neonatal unit helps develop technical and crisis resource management skills and can also identify latent threats in a system.
- Once latent safety threats are identified, it is possible to implement a process to mitigate them.
- Successful translation of mitigation processes to real-life scenarios indicates effective training and a patient-safe environment.
Also published in Infant:
