

Neonatal grid training experiences: a UK-wide survey
Level 3 neonatal subspecialty training is assessed by an outcomes-based curriculum and can be undertaken at one of 15 deaneries across the UK. We undertook a survey to collate the experience of neonatal grid trainees across the UK with regards to the training they are receiving, to assess if and how neonatal units offer support to grid trainees towards achieving their competencies. The results demonstrated a concerning disparity between trainees’ experience across the UK compared to the competency-based curriculum outlined by the Royal College of Paediatrics and Child Health, creating significant potential gaps in trainees’ experience in preparing them for the consultant role.
Anna Darbyshire
Neonatal Grid Registrar
anna.darbyshire@nhs.net
Oluwaseyi Alake
Consultant Neonatologist
Asha Shenvi
Consultant Neonatologist
Neonatal Intensive Care Unit, Royal Stoke University Hospital, University Hospitals of North Midlands
The National Grid is a training scheme that represents a unique partnership between deaneries and the Royal College of Paediatrics and Child Health (RCPCH) in offering, through national competition, equitable access to high quality subspecialty training.1 In the UK, at level 3 of training (specialist trainee 6 to 8, ST6-8), paediatric trainees can begin subspecialty training in neonatology and ultimately enter on to the General Medical Council Specialist Register as a paediatrician with subspecialty training in neonatology.
Training is ideally three years in total – either three years neonatal medicine or two years neonatal medicine and one year of an allied specialty, such as paediatric cardiology or neonatal transport, research or overseas posts. Training is assessed by an outcomes-based curriculum and can be undertaken at one of 15 deaneries across the UK. The College Specialty Advisory Committees (CSAC) supervise the development and delivery of neonatal subspecialty training and the assessment standards. As of 1st August 2018, grid trainees use the RCPCH Progress level 3 generic syllabus alongside the RCPCH Progress neonatal medicine syllabus.2
Aim
Our aim was to collate the experiences of neonatal grid trainees across the UK in order to evaluate how various neonatal units and deaneries support grid trainees towards achieving their competencies outlined within the grid curriculum.
Methods
A 26-question survey was designed, based on the curriculum, to assess trainees’ experiences and a qualitative analysis of the responses was performed. The survey included sections on the working rota, training opportunities, management, leadership and service-related skills, and clinical skills. An electronic survey link was sent to all neonatal grid trainees, via the neonatal grid trainee representative, between March 2020 and May 2020. There were 125 grid trainees at the time; however, the survey was sent to 85 as the remainder had just been appointed and were, therefore, excluded.
The survey was left open until September 2020 to encourage sufficient responses from trainees and reminder emails were sent out twice after the initial invitation.
Results
There were 31 responses from ST6-ST8 trainees during the period of the survey. The responses spanned across 11 of the 15 deaneries (FIGURE 1):
- nine respondents (29%) were ST8
- 13 (42%) were ST7
- nine (29%) were ST6.
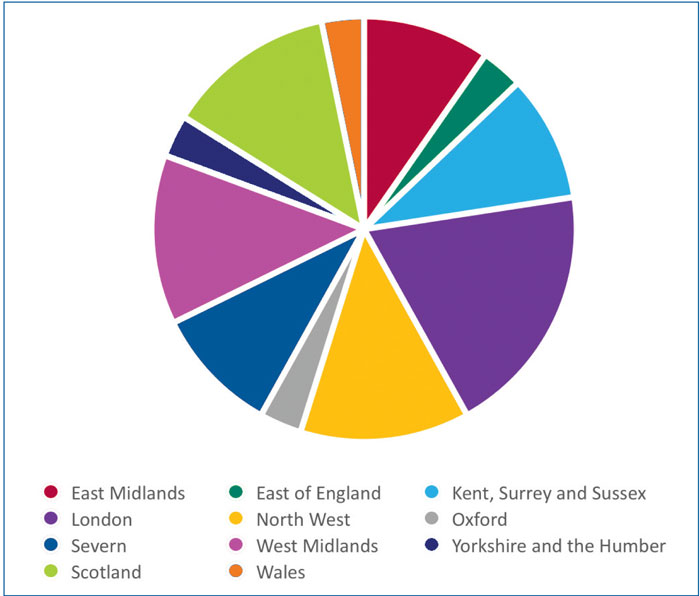
FIGURE 1 Distribution of respondents based on UK deanery.
Training opportunities
From a training opportunity perspective, 77% of respondents have access to neonatal grid training study days, but only around 20% of these had grid study days built in to their rota to allow attendance at these days.
Trainees were asked whether their rota facilitated attending antenatal counselling sessions and fetal medicine clinics; half of the respondents were not facilitated to attend key antenatal counselling sessions and two-thirds were not able to attend fetal medicine clinics. Just over a third were also not facilitated to attend specialist clinics, eg cardiology or chronic lung disease clinics.
There were also notable discrepancies in trainee clinical skills with over 50% not having the opportunity to undertake neonatal transport and 35% not having the opportunity to attend Bayley clinics. It is our opinion that the transport of sick infants to an appropriate neonatal unit and neurodevelopmental assessments are fundamentals of neonatal care and not gaining experience in these areas reflects poorly on the preparation of trainees for the consultant role.
Management, leadership and service-related skills
Less than 20% of trainees had been involved in developing a business case and 58% had no experience of supporting a trainee in difficulty. The majority of trainees had been able to get involved in an educational programme. Less than 10% of trainees had consented for a post-mortem examination and less than 20% had made a referral to the coroner. 13% and 29% had been involved in responding to a complaint and performing a root cause analysis, respectively.
Only 9% had had the opportunity to act as consultant of the week. We noted specifically that 29% of trainees were nearing the end of their ST8 year. Therefore, these trainees are likely to become neonatal consultants in 12-18 months’ time and are yet to have had the opportunity to act in the consultant role while being supported by a consultant.
Reassuringly, the majority of trainees had experience of discussions regarding reorientation of care (77%); a vital skill for neonatal consultants.
Discussion
Neonatal clinical service provision requirements often mean that neonatal grid trainees are participating on the same rota as other paediatric registrars who may be at the ST4 level. The training requirements of a neonatal grid trainee at ST8 level are vastly different to new registrars at ST4 level. It is crucial that neonatal units recognise the training requirements of grid trainees and maximise training opportunities for them by providing a slightly separate or adapted rota. Grid trainees are likely to have more knowledge and experience and would be able to provide support and training to other more junior registrars; their skills in this regard should be utilised. This process can be achieved by good communication between each department’s RCPCH college tutor and the neonatal consultants, prior to commencement of a new rotation. Discussion around the grid trainees and their specific needs are key; this will allow for better planning of provision of training opportunities. For more senior grid trainees, educational supervisors should be allocated based on their area of interest.
Our results are borne out by other similar surveys. A survey in 2012 on trainees’ views on being prepared for the consultant role showed that for neonatal paediatrics in the UK, new consultants feel confident about managing ill babies but are unprepared for other aspects of the consultant's role.3,4 The authors suggest that neonatal higher specialist training needs to allow opportunities for non-clinical training.
A 2018 survey of neonatal subspecialty trainees (ST5-ST8) collected information on exposure to fetal medicine and antenatal counselling, concluding that the level of experience was inconsistent and confidence was generally lacking.5 This seemed to be as a result of variable opportunity to learn about fetal medicine and develop counselling skills.
The article, The future of paediatric training in the United Kingdom - the trainees’ perspective,6 identifies that: “In addition to core training, it is essential to develop the generic skills needed to become a competent senior doctor. Areas of importance include communication skills, ethics, medical law, teaching techniques and management.” The author goes on to state: “Most deaneries co-ordinate sessions on these topics but not all regions provide funding and special leave over and above the normal entitlement for the trainee to attend.” The RCPCH charter for trainees in 2019 recommends stipulated non-clinical time in addition to departmental teaching and clinical admin time, which most training centres are finding difficult to deliver.7
Our results highlight a disparity in neonatal grid training in the UK. Training deaneries need to have a streamlined approach to providing a training programme that is mapped with the RCPCH grid curriculum, and they need to mobilise the tertiary neonatal units to support grid trainees towards achieving this in preparation for life as a neonatologist. There should be a balance between service provision and training opportunities. There should be dedicated rota time for management and leadership activities, such as gaining an in-depth understanding of the clinical governance processes by undertaking a root cause analysis and responding to complaints (with consultant supervision). A grid trainee lacking in these experiences is likely to suffer a steep learning curve when transitioning from registrar to consultant. There needs to be a degree of flexibility within the rota for ad hoc training opportunities such as post-mortem consent or antenatal counselling.
At Royal Stoke University Hospital, we have attempted to address this training need. Consultants support the trainee to achieve competencies within their own areas of special interest, for example: the clinical lead facilitates attendance at management meetings; the mortality lead facilitates attendance at mortality reviews; the BadgerNet and National Neonatal Audit Project leads facilitate data collection and report writing; the trainee is encouraged and supported to develop cranial ultrasound scans and echocardiography skills, if interested. In addition, the trainee is allocated a thoughtout quality improvement project based on consultant consensus and departmental needs, which they are expected to lead on and complete within 12 months.
Grid trainees are empowered to take ownership of the tier 2 rota and allocate trainees each week to the different clinical areas. The traineeis directed early to the rota manager and works collaboratively with them. In doing so, the grid trainee can adapt the rota to facilitate their own learning needs, while also gaining management and leadership experience. For example, on days where there are surplus registrars, grid trainees are able to attend specialist clinics or join the governance lead.
The role of the educational supervisor alternates between two consultants on a yearly basis. At the start of the academic year, trainees are provided with clear targets for the year ahead and the contact details for those who can help in achieving these targets. This includes specialists from other departments (eg fetal medicine, paediatric subspecialties – respiratory, gastroenterology, cardiology, etc) to enable attendance at specialist clinics (eg chronic lung disease clinic, cardiology clinic, etc). The whole consultant team is aware of, and supports, the differing training needs of a grid subspecialty trainee, as opposed to those needs of a level 2 paediatric registrar. From a grid trainee perspective, this system gives the trainee the right balance between having autonomy over their learning needs and the support to achieve their goals. It is recognised that the clinical needs and the skill mix will vary among different units, and these methods may not fit elsewhere.
Conclusion
In summary, there is a wide variation in neonatal grid training experience across deaneries in the UK. This creates significant potential gaps in trainees’ experience in preparation for the consultant role. These gaps are more prominent in the domain of management skills, but it is concerning there are deficiencies noted in clinical training as well. It is crucial that the rota is specifically modified to accommodate grid training days, ad hoc opportunities for clinical skills and opportunities to acquire governance and management skills. Training units need to provide individualised grid trainee-specific training opportunities to support the development of neonatal competencies.
Author contributions
Dr Shenvi and Dr Alake conceived the concept and designed the survey. Dr Alake conducted the survey and Dr Darbyshire wrote the article. All authors undertook subsequent reviews of the manuscript.
Or read this article in our
Tablet/iPad edition
- Neonatal grid training is outcomes-based and can be undertaken at one of 15 deaneries across the UK.
- Our survey of neonatal grid trainees highlights potential gaps in training opportunities, particularly in clinical governance and management skills.
- Training centres should recognise the unique training requirements of grid trainees and facilitate learning opportunities in clinical, management and leadership skills.
- A model example from our centre is explained from a grid trainee's perspective.
Also published in Infant:
