

Neonatologist-performed echocardiography: a pilot programme for delivering training and maintaining accreditation
Neonatologist-performed echocardiography is increasingly recognised as a useful clinical tool in the management of sick and often very preterm infants. However, robust training and governance processes, critical for neonatologists and their patients, are not routine in the UK. A variety of training ‘expert statements’ require collaboration between paediatric cardiology and neonatology services. We describe our successful experience of delivering this training within the UK higher specialist training programme and describe how this could be replicated in other training centres. UK certification and training programmes should be developed.
Anne Marie Heuchan1
Consultant in Neonatal Medicine
annemarie.heuchan@ggc.scot.nhs.uk
Mahmoud Montasser2
Consultant in Neonatal Medicine
Neil Patel1
Consultant in Neonatal Medicine
Lindsey E Hunter1
Consultant in Paediatric Cardiology
2University Hospital Wishaw, Lanarkshire
Background
Neonatologist-performed echocardio-graphy (NoPE) is increasingly recognised as a useful clinical tool in the management of sick and often very preterm infants.1-3 For a variety of clinical questions, such as significance of the patent ductus arteriosus (PDA), presence of acute or chronic pulmonary hypertension (PPHN), assessment of neonatal hypotension and/or cardiac dysfunction, line placement and exclusion of pericardial effusion, NoPE can provide valuable information to support clinical decisions and monitoring of treatment.2-7 However, the neonatal transitional circulation is unique and can coexist with unrecognised major congenital heart disease. It is essential that those undertaking NoPE have received robust technical echocardiography training, can exclude major congenital heart defects and also interpret transitional and functional changes in context of the clinical situation and neonatal care.
Concerns remain that without a structured training programme and gover-nance procedures, NoPE may result in misdiagnosis, potentially harmful inter-ventions or delays in appropriate referral to paediatric cardiology. These concerns have led to a number of proposed guidelines for NoPE training internationally. In Australia, governance has evolved independently of paediatric cardiology with the well-established Australian Neonatal Certificate in Clinician Performed Ultrasound (asum.com.au). Training is delivered by experienced neonatologists with their own training programme, resources and governance supported by the Australasian College of Radiologists. More recently there has been a plethora of training recommendations internationally and three different expert consensus statements specifically relevant to the UK and Europe.8-11 Notably all approaches, except the Australian, recommend involvement of paediatric cardiology in training with a primary emphasis on systematically confirming structural normality. However, the combined American and European Association practice guidelines for targeted neonatal echocardiography (TNE) training requirements8 are so dependent on cardiology training that they would both compete directly with cardiology training places in the UK and compromise neonatal training. Therefore these have not been adopted in the UK or most of Europe. The most recent proposal for training and accreditation (framework) specifically for the UK,9 which is compatible with wider European recommendations10,11 takes a more pragmatic approach but mandates a governance and training system with paediatric cardiology. Importantly, this approach was broadly endorsed by the British Congenital Cardiac Association (BCCA) and specialist neonatal interest groups in the UK. Key elements for training and practice are outlined in TABLE 1. Training takes a minimum of 12 months, suggests six months each in a paediatric cardiac centre and tertiary neonatal unit, joint neonatologist and cardiologist supervision, and 20% of time dedicated to echocardiography during the year. Although less onerous than the TNE standards, the training requirements have been considered challenging and neither the training programme nor system of accreditation have yet been established in the UK.
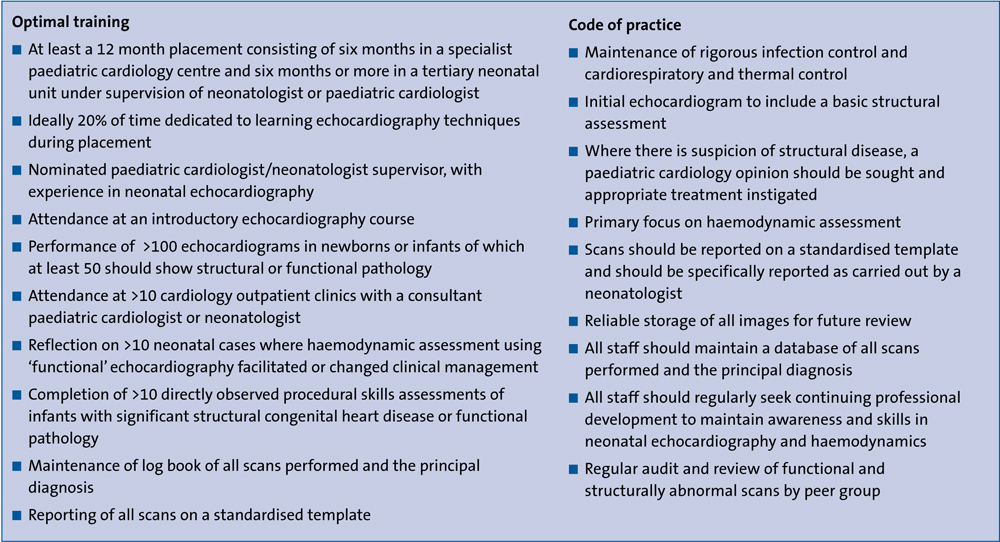
TABLE 1 Key elements of optimal training and code of practice for neonatologist-performed echocardiography. Adapted from Singh et al.9
Pilot training programme
Recognising the need for this structured training and the benefits of adopting the UK NoPE framework, we utilised the Royal College of Paediatrics and Child Health (RCPCH) Higher Specialist Training (HST) programme in neonatal medicine, advice from the paediatric Training Programme Director and the excellent working relationship between neonatology and cardiology at our institution, to pilot and test the feasibility of the delivery of the UK NoPE training framework.
Methods
Our pilot was designed to follow the key elements of the codes of practice from the UK Expert Consensus statement (TABLE 1). Utilising these we developed a flowchart for delivering NoPE training (FIGURE 1). The processes involved, the achievements and challenges are described and reviewed.
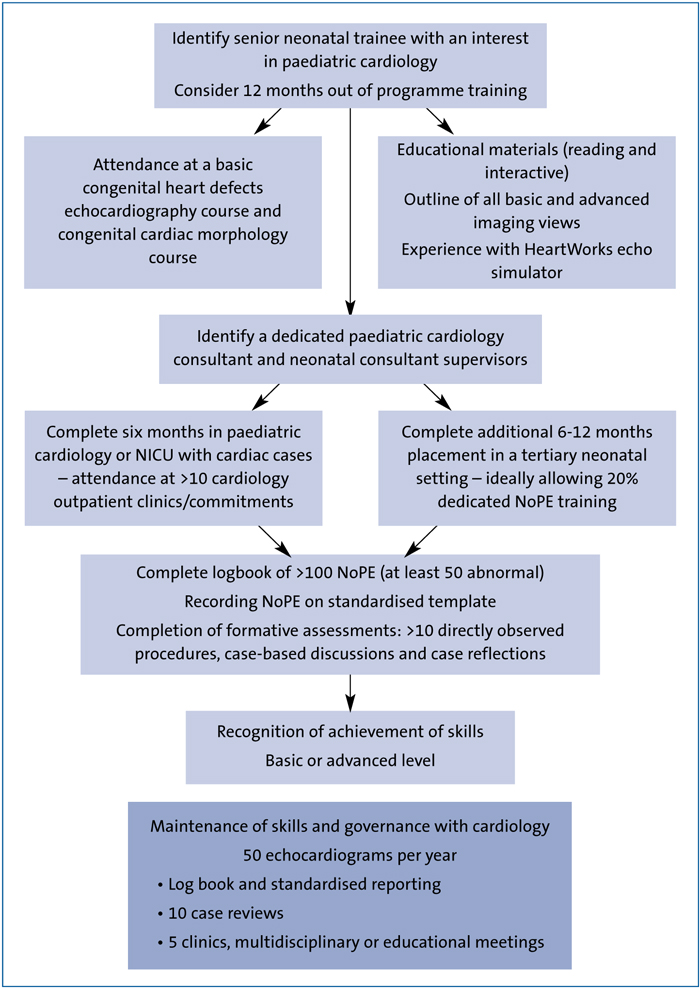 FIGURE 1 Training flowchart.
FIGURE 1 Training flowchart.
Candidate, training centre and training approval
Our neonatal service is co-located with the Royal Hospital for Children, Glasgow, and the Queen Elizabeth University Hospital maternity services. The neonatal unit supports many specialist services including neonatal cardiology, cardiac surgery and extracorporeal life support (ECLS). This juxtaposition of services provides an excellent opportunity to facilitate neonatal and cardiology collaboration. The RCPCH training programme allows HST trainees, with no previous time out of programme, to undertake a 6-12 month post within an allied specialty. In collaboration with paediatric cardiology, a six-month rotation with a view to commencing NoPE training was agreed with the Training Programme Director. This provided the appropriate environment to test the feasibility of NoPE training both within our centre and within the RCPCH training programme. Our HST trainee had expressed an interest in developing skills in neonatal echocardiography and had undertaken previous courses in echocardiography and cardiac morphology.
NoPE trainers
The UK framework provides a governance system for neonatologists performing echocardiography but does not define a level of experience for trainers. In our neonatal intensive care unit (NICU), NoPE clinicians have designated link paediatric cardiologists and, in accordance with a more recent consensus statement on neonatologist-performed echocardiography in Europe,10 our NoPE clinicians have practised for greater than five years, each perform >50 scans per annum and have a governance link with a paediatric cardiologist. Additionally they have expertise in a variety of areas and utilise this to guide the management of infants with congenital diaphragmatic hernia (CDH),12 PDA,13,14 pulmonary hypertension, advanced functional measurements13 and flow measurements.15,16
A link paediatric cardiologist accepted the mentoring role for our neonatal trainee and training was approved by all of our paediatric cardiologists. Teaching materials and a formative approach to assessment of echocardiography skills were developed collaboratively.
Equipment and data storage
Both the NICU and cardiology department utilise high specification ultrasound equipment (Vivid E9, GE Healthcare) with 12 and 6MHz probes, tissue Doppler and speckle tracking capability. All staff adhere to rigorous infection control procedures, thermo-respiratory care of the infant and use of ‘inline ECG’. An EchoPAC (GE Healthcare) workstation was installed in the neonatal department and linked to the cardiology server. This allowed storage of images, review and post-processing analysis and facilitated teaching and governance requirements. Approval was obtained to allow reporting of NoPE studies as neonatologist-performed studies on the hospital HeartSuite (www.heartsuite.com) database.
Education and assessment
The trainee was provided with educational literature11,17-21 and directed to interactive resources: Practical Echocardiography for the Neonatologist Parts 1 and 222 and www.tnecho.com providing interactive advice on image acquisition, assessment of common neonatal transitional or maladaptive physiology and reviews of advanced functional assessment. Experience of echo simulator training (HeartWorks (www.intelligentultrasound.com/heartworks) was also available.
Clinical training commenced with six months in paediatric cardiology ensuring competency in basic image acquisition.8 The daytime service included rotation between the ward, clinics and cardiac catheter lab. However, it was rapidly recognised that priority should be given to newborn presentations and where possible the trainee was directed to review new referrals from the NICU, including infants with suspected congenital heart disease. There were Tier 2 on-call responsibilities but these were well supported by the cardiology consultant and cardiac physiologists. In addition, attendance at weekly educational meetings and cardiac multidisciplinary meetings was required.
The 12-month neonatal attachment included clinical assessment of admissions with suspected congenital heart defects and care of infants with a range or conditions including prematurity, PDA, CDH, severe pulmonary hypertension, therapeutic hypothermia or referral for ECLS assessment. Opportunities to consolidate transthoracic echocardiography skills were achieved on most shifts. Additionally, advanced neonatal functional parameters were developed: tissue Doppler imaging; speckle tracking echocardiography, or ventricular output or flow measurements.
Formative assessments and competency levels
Case-based discussions (CBDs); directly observed procedures (DOPs) and reflective cases were chosen by both mentor and trainee to meet the documented educa-tional requirements. These were recorded on the trainee’s RCPCH e-portfolio. The CBDs could be based on the DOPs or reviewed scans with clinical history. CBDs included the physiology of the transitional circulation, options for management in a variety of clinical conditions (therapeutic hypothermia, PDA, PPHN, CDH and newborns with congenital heart disease) and the role of echocardiography in diagnosis and enhancing care.
All initial echocardiograms were supervised but as the trainee progressed they were performed independently. The majority of the echocardiograms were reviewed jointly – either with a NoPE clinician to discuss the clinical significance of functional assessment or with a cardiologist if there were concerns about congenital heart defects. This superseded our requirement for a random selection of echocardiograms every six weeks for review and audit.
Governance
The UK NoPE framework describes a governance system for established neonatal echocardiographers to which we adhered. Formal guidelines for assessing, grading and medical management of PDA were also developed, along with a standardised measurement and grading protocols for assessing PPHN. This provided an education framework for our trainee, a standardised approach for measurements and reporting and an opportunity to gather data for audit or research. In addition we developed pathways for referral to the cardiology service, which included suspicion of congenital heart defects, PDA requiring consideration for surgery, PPHN for consideration of ECLS, cases not responding to medical treatment or where the echo findings did not appear to match the clinical condition.
Outcomes
All scans, once full supervision during image acquisition was no longer required, were recorded in the trainee’s log book and completed within 12 months. They reflect early recognition that learning objectives were best met by shifting the focus away from complex anatomy to more common newborn problems. Cardiology echo-cardiographs (n=31) included only nine complex congenital cases with the remainder focusing on murmurs, PDA (pre- and post-ligation) and functional assessments in the NICU and paediatric ICU. Scans undertaken during the neonatal attachment (n=69) were predominantly PDA, PPHN, volume and functional assessment and included extremely preterm infants, therapeutic hypothermia, CDH and ECMO and contributed greatly to understanding of transitional circulations in a clinical context. Examples included emergency assessments of hypotension, the need for nitric oxide in persistent pulmonary hypotension of the newborn, assessment of PDA, and identification of coarctation of the aorta during a scan to check a peripherally inserted central catheter placement in an infant undergoing therapeutic hypothermia (FIGURE 2A-C).
Review of the process allowed us to reflect on trainee, trainer and centre requirements and we have summarised desirable characteristics of these in TABLE 2. These characteristics are well matched to previously described European guidance.11
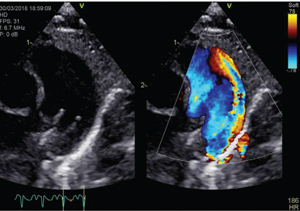
FIGURE 2A A Large haemodynamically significant PDA in a preterm infant.
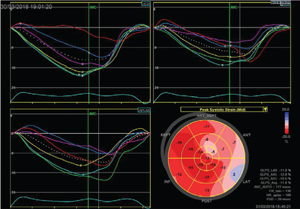
FIGURE 2B Reduced systolic left ventricular function assessed by speckle tracking in an infant with PDA.
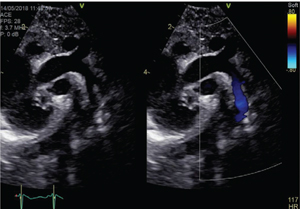
FIGURE 2C Coarctation of the aorta with accentuation of flow at the narrow segment identified when assessing line placement.
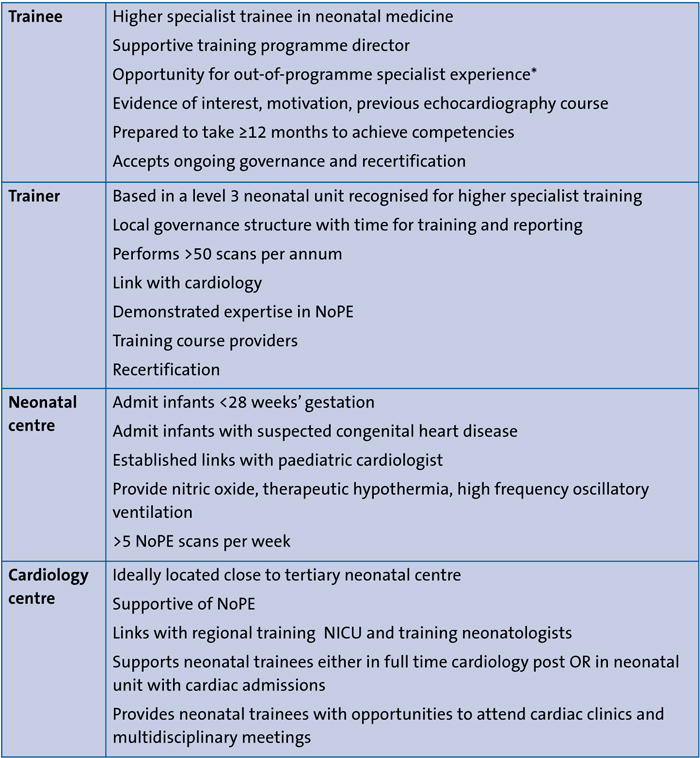
TABLE 2 Desirable characteristics for training centres, trainers and trainees. *May not be essential depending on local arrangements and previous experience but must ensure involvement in governance process.
Discussion
In our experience, a collaborative approach between paediatric cardiology and neonatology worked well and can effectively deliver NoPE training, based on the UK framework, within the current RCPCH higher specialist neonatal training structure. Benefits of developing a local training structure included establishing governance pathways with cardiology, formalised assessment protocols for common neonatal conditions (eg PDA and pulmonary hypertension) and standardised reporting templates. This ensured the delivery of prompt haemo-dynamic review in the NICU, reduced demands on paediatric cardiology and enhanced our governance processes. Although we had the advantage of co-location of both cardiology and neonatology, and our trainees found the cardiology training beneficial, this block placement approach may not be achievable across all training regions. However, the principle of a training framework with cardiology and neonatology governance (recognised neonatal and cardiology supervisors, exposure to neonates with congenital heart disease, exposure to cardiology clinics and multidisciplinary meetings, and placements in appropriate tertiary neonatal units) could be adapted to individual deaneries or regions (TABLE 2) and remain within the remit of both the UK9 and European guidance.11
The most challenging element of the UK Expert Statement is the proposal that 20% of time should be dedicated to learning echocardiography, which we were unable to deliver formally. While echocardiography may be opportunistic, the opportunity to have formal protected time for review would have been ideal. Training deaneries should recognise that the RCPCH recommends that all HSTs should have protected time to develop areas of special interest. Those developing NoPE skills could utilise this time to review images. The commitment from the trainers was also significant, and along with governance arrangements for maintaining skills,9 should be negotiated into local job plans.
Despite this, training is essentially competency-based and in our experience requires a minimum of 12 months to achieve the requirements. Ideally, trainees should identify their interest as soon as possible as attendance on basic education courses, reading and acquisition of basic image skills in advance will rapidly accelerate the learning once in the programme. However, providing links with supervisors are maintained, skill acquisition could continue over a longer period.
One deficiency of the current Expert Statement9 is the lack of distinction between core or basic echocardiography competencies and advanced competencies. We suggest core competencies should include understanding basic physics, ability to acquire and report all standard views and ability to assess both PDA and pulmonary hypertension based on established views, Doppler and M-mode interrogation. Consideration should be given to assessment of central line placement. Advanced competencies should incorporate the use of flow measurements and/or the option of novel functional measures, which we recommend are demonstrated on at least 25 studies but can be incorporated into the 100 studies.
At present there is no certification programme for neonatologist training in echocardiography in the UK or in Europe. A pan-European training programme and certification system would be welcome but may prove elusive and should not halt the delivery of training and accreditation in the UK. In the interim, the suggested UK/European framework is achievable, particularly within a service delivery model moving towards centralisation of care of the smallest infants. Regional collaboration with cardiac services is required but achievable in a variety of models. Ultimately, certification could be managed by the RCPCH or the auspices of the European Society for Paediatric Research or European Board of Neonatology.10 However, more important is a practical move towards deliverable training in NoPE in the UK, with a robust governance framework, regional formal links with paediatric cardiology and a UK certification programme.
Conclusions
NoPE is becoming an integral component of modern neonatal intensive care management. Robust training and quality assurance are critical. We present a successful pilot of a structured training programme, following the UK consensus framework. The process improved governance structures and collaboration across neonatology and paediatric cardiology. Collaboration with paediatric cardiology is essential but training is largely competency based and should be deliverable across other tertiary centres. Future considerations should be given to defining basic and advanced echocardio-graphy curriculum and development of a UK certification programme as a priority.
Or read this article in our
Tablet/iPad edition
- NoPE provides enhanced clinical care within neonatal intensive care settings.
- European and UK NoPE training statements mandate collaboration between paediatric cardiology and neonatology.
- Collaborative NoPE training can be delivered within the UK neonatal HST programme.
- Formal UK certification and NoPE training programmes should be developed.
Also published in Infant:
This year’s NeoCard conference focussed on the various aspects of neonatal perfusion assessement and its management.
