

Healthcare professionals’ views to inform revision of the NEWTT tool
Early identification of clinical deterioration provides an opportunity for timely intervention that may prevent irreversible harm and death in newborn infants. Early warning scores, such as the British Association of Perinatal Medicine Newborn Early Warning Trigger and Track (BAPM NEWTT), are used for this purpose. We set out to gather opinions of UK healthcare professionals to inform a review of the BAPM NEWTT guidance and identify features that may require modification.
Shalini Ojha
Consultant Neonatologist, University Hospitals of Derby and Burton, and Clinical Associate Professor, University of Nottingham
shalini.ojha@nottingham.ac.uk
Kathryn Macallister
Neonatal GRID Trainee, BAPM Trainee EC Representative, Co-Chair NEWTT2 working group
Sara Abdula
Advanced Neonatal Nurse Practitioner, Chelsea and Westminster Hospital, London
John Madar
Consultant Neonatologist, Neonatal Unit, University Hospitals Plymouth
Oliver Rackham
Consultant Neonatologist, Glan Clwyd Hospital, Rhyl, Wales
Wendy Tyler
Consultant Neonatologist, BAPM Honorary Treasurer, Chair NEWTT2 working group
Most newborn infants thrive with warmth and feeding. They do not require observation or interventions. Others may be vulnerable and/or exposed to threats, the signs of which may not manifest immediately. Such conditions, if not identified and treated, could lead to significant and avoidable harm. Early identification of impending deterioration provides an opportunity for appropriate interventions that could prevent irreversible damage and save life.1 Inspired by the popular implementation of early warning scores (EWS) and trigger and track charts in adult and paediatric medicine, similar tools were designed for newborn infants. In 2015, the British Association of Perinatal Medicine (BAPM) published a framework for practice promoting the use of BAPM Newborn Early Warning Trigger and Track (NEWTT) chart.2 This framework is currently under review by an expert group established by BAPM.
While several studies have evaluated the impact of implementation of EWS, there is no evidence to support the assumption that use of EWS reduces mortality or other adverse outcomes.3,4 A review of EWS in neonates found four tools and reported that all were based on limited evidence and none were adequately validated.5 Although this review suggested a modified score is required, the authors did not find any evidence to support the creation of such a score. For many clinical questions, published evidence is limited, too indirect, or does not exist.6 While opinions are the lowest quality of evidence, where there is little or no systematic empirical evidence, opinions may be helpful in guiding recommendations.7 To inform the review of the BAPM NEWTT guidance, we conducted a survey of healthcare professionals in the UK and performed a mixed-methods analysis of the responses to help identify key features that require modification.
Methods
The survey questionnaire was created using the online survey dashboard available at jisc.ac.uk (Jisc, Bristol, UK) by the BAPM NEWTT review team. It was pretested by three members in January 2021. The final survey was released on 2 March 2021.
Questions were a combination of multiple response and yes/no questions with free text options for comments. The BAPM NEWTT (2015) chart includes the following:
For each of these, we asked if the respondent would like any of the listed criteria to be changed. Each question included a response to indicate that the respondent agreed with all the listed criteria. Those who opted for a change were asked what they wanted to change and how. Next, we asked if that section of the chart needed any additional element and if yes, what addition was required and why. Except for the yes/no questions, all questions allowed for multiple responses.
An initial scoping survey conducted via the neonatal networks showed that the 92% of UK neonatal services use an EWS and that 79% used the BAPM NEWTT (2015) charts. Other EWS systems in use include the Neonatal Alert, Trigger & Track8 (three hospitals), and NeoNEWS9 (six hospitals). Healthcare professionals at these centres provided their contact details for participation in further detailed surveys and emails were sent (n=62). In addition, the survey link was shared via the BAPM official Twitter account, the BAPM newsletters, social media accounts and newsletters of the Royal College of Midwives and the British Maternal and Fetal Medicine Society. The survey closed on 30 March 2021. No sample size calculation was performed and there were no limits to the number of responses that could be received.
Results
There were 432 responses including from 57/62 (92%) of the healthcare professionals emailed directly. Two blank responses were excluded, and 430 responses were analysed (90 consultant paediatrician/neonatologists; 162 midwives; 12 healthcare assistants; 34 junior doctors; 83 neonatal nurses; 42 nurse practitioners; 5 ‘others’ and 2 missing data). The levels of neonatal units at the place of work of the respondents were: neonatal intensive care unit=204, local neonatal unit=180, special care unit=40, none at site=1, other=3, missing=2.
FIGURE 1 shows the number of respon-dents who agreed with all the criteria in the BAPM NEWTT (2015) chart. The number of respondents, by professional category, who asked for specific criteria to be changed (ie removed or modified) is given in FIGURE 2.
The free text responses were analysed and categorised into themes. Themes that recurred in five or more responses were extracted and reported. Representative quotations are quoted verbatim.
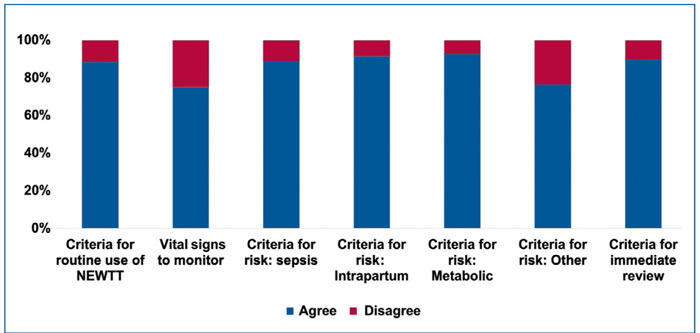
FIGURE 1 Number of respondents who agreed or disagreed with the criteria included within the categories in the BAPM NEWTT chart (2015).
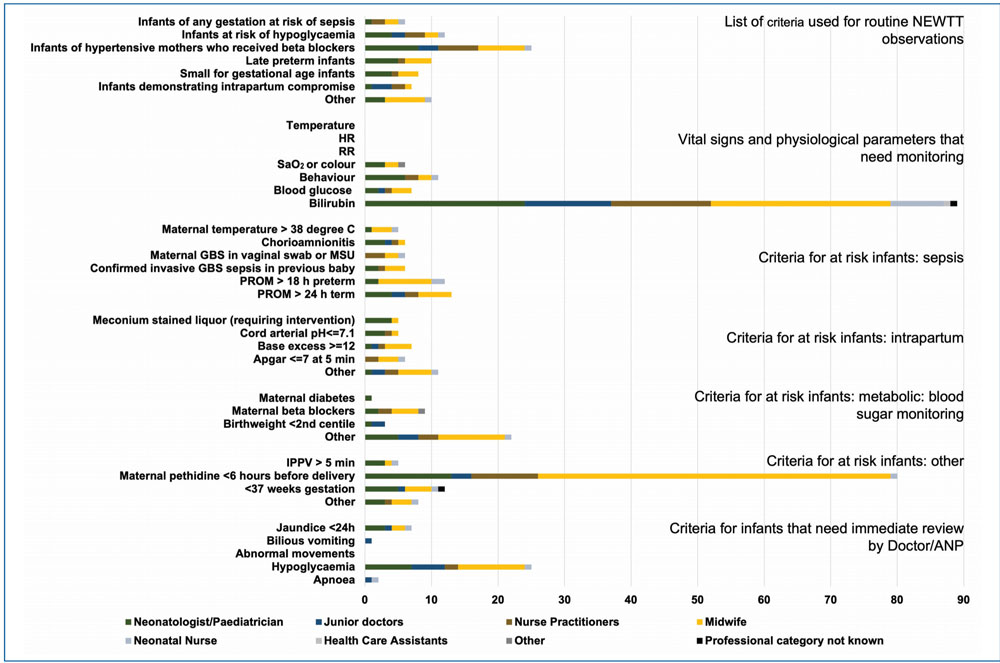
FIGURE 2 Number of respondents in each professional category who disagreed with one or more criteria included within the categories in the BAPM NEWTT chart (2015). Key: ANP=advanced nurse practitioner; GBS=Group B Streptococcus; MSU=mid-stream urine; HR=heart rate; IPPV=intermittent positive pressure ventilation; PROM=prolonged rupture of membranes; SaO2=oxygen saturation; RR=respiratory rate.
At-risk categories for routine NEWTT monitoring
When asked about the list of criteria used to select babies for routine use of NEWTT, 45/430 respondents wanted one or more categories changed or removed including 25 who wanted infants of hypertensive mothers who received beta blockers to be excluded as a separate category. 141 (33%) respondents suggested a new category. Themes identified from the free-text responses are given in TABLE 1.
Signs monitored on the NEWTT chart
The next two questions referred to the vital signs and physiological parameters that are currently monitored. As seen in FIGURE 2, all agreed that heart rate, respiratory rate, and temperature should be included. 100/430 (23%) wanted to exclude one or more of the other measures. 123/430 (29%) said they wanted a measure added. The thematic analysis of the responses to these two questions are given in TABLE 2.
Identification of infants at risk of sepsis
382/430 (89%) respondents indicated that they did not want any of the sepsis risk factors to be excluded. Among responses from those suggesting change, most pertained to the two different cut-offs for prolonged rupture of membranes and aligning the risk factors with those given in the relevant NICE (National Institute for Health and Care Excellence) guideline. For example:
- “Two different categories of PROM in the same list causes confusion” (Consultant)
- “Does not need excluding but emphasising pre-labour ROM, in line with current NICE guidance” (Consultant).
Five others suggested that maternal temperature and chorioamnionitis can be non-specific terms. For example:
- “Maternal temp: This could be caused by a number of reasons = is it likely to be sepsis?” (Midwife)
- “Chorioamnionitis is an overused term, will this be confirmed?” (Midwife).
In addition, five respondents said that babies should not need observations if the mother has received adequate intrapartum antibiotics.
95/430 (22%) respondents suggested additional criteria for sepsis. Most (32/95 responses) referred to adding the decision from the sepsis risk calculator to the criteria and 11/95 to aligning the guidance to NICE recommendations. 24/95 responses asked for maternal sepsis to be included as a risk factor, particularly when the mother is being treated with antibiotics.
Identification of infants at risk of intrapartum compromise
393/430 (91%) agree with all the criteria given as intrapartum risk factors and did not want to exclude any. 8/28 who wanted a change, asked for the criterion meconium-stained liquor (requiring intervention) to be removed. For example:
- “Meconium stained liquor - requiring intervention. I think people don’t know what this means and therefore just put babies on NEWTTs for thick mec even when uncomplicated and no intervention” (Midwife).
50/430 (12%) of respondents wanted to add a risk factor to this list. Most comments (18/50) referred to including intrapartum events such as fetal bradycardia, shoulder dystocia, maternal antepartum haemorrhage, or abruption. 8/50 responses indicated that high lactate levels on the cord blood gas or infant’s first blood gas should also be considered a risk factor for intrapartum compromise.
Identification of infants at risk of hypoglycaemia
398/430 (92.5%) agreed with all listed criteria. Several comments referred to the earlier themes that a full set of NEWTT observations are not required for all infants in this group. Similarly, there were comments that infants with a family history of a metabolic condition and infants whose mothers receive beta-blockers are generally well.
While most (303/430; 70%) did not want any additional criterion, 35 responses suggested adding large for gestational age babies.
Some respondents questioned the cut-off of birth weight below the second centile for defining small for gestational age infants.
Identification of infants at ‘other’ risks
329/430 (77%) agreed with all those listed. Among those who disagreed, 80 objections were about maternal pethidine
373/430 (88%) respondents did not want any additional criteria. 14 indicated that infants at risk of neonatal abstinence syndrome should be monitored using NEWTT.
Other themes, previously mentioned, recurred with responses suggesting NEWTT monitoring for infants with jaundice, traumatic delivery, maternal thyroid problems and poor feeding.
Identification of infants who require immediate review or ‘red category’
391/430 (91%) agreed with all the ‘red’ categories. Most (25/26) responses said that asymptomatic hypoglycaemia and jaundice do not require immediate review.
112/430 (26%) suggested additional categories. Of these, 102 suggested including acutely unwell infants such as those with significant respiratory distress, bradycardia, unresponsiveness or abnormal movements.
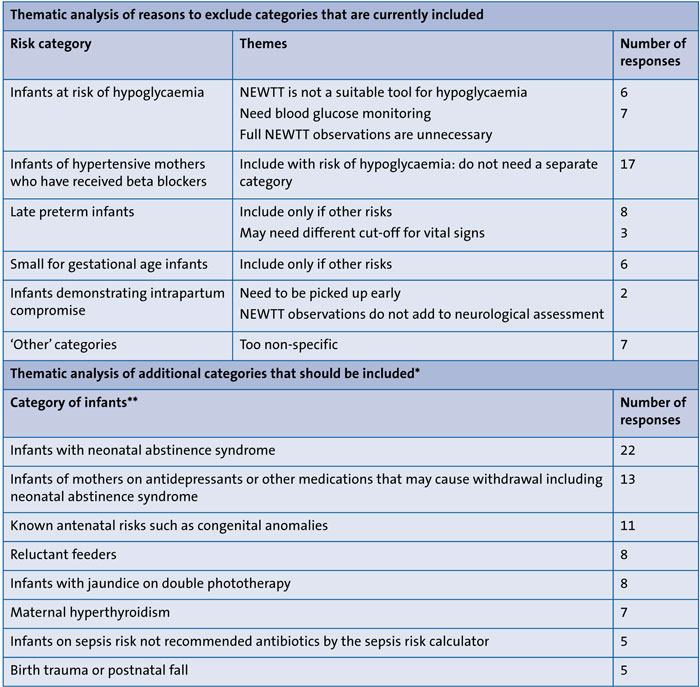
TABLE 1 Thematic analysis of response to questions about risk categories for routine use of the BAPM NEWTT charts. *Excluding 41 responses that referred to ‘infants born with thick or significant meconium-stained amniotic fluid’ and 17 other responses that suggested categories that are already included. **Other themes that received fewer than five counts: all infants (4); infants discharged from neonatal unit (3); elective c-section (2); large for gestational age infants (2); low birth weight infants (2); social concerns (2); infant of mother with COVID-19 (2); parental concern (1).
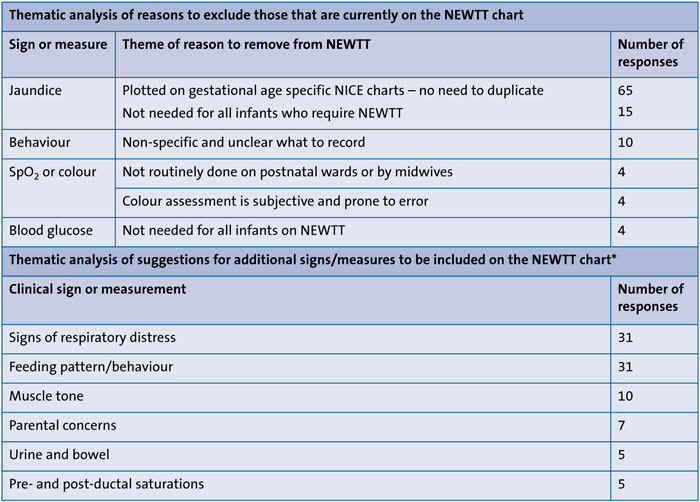
TABLE 2 Thematic analysis of responses to questions about vital signs and/or physiological measures on the BAPM NEWTT chart. *Other suggestions that received fewer than five counts: blood pressure (4); pain score (4); capillary refill time (2); healthcare professional concern (2); medications (1); does the infant look well? (1).
Other notable comments and views
In addition to the responses to specific survey questions, some notable contrasting opinions were expressed. These included:
- “I have profound concerns about the whole concept of the NEWTT chart. It is based on the idea that ‘tracking’ variables that are outside the normal physiological range can add assurance to the wellbeing of a baby. There is no scientific basis for the thinking, or the variables chosen as thresholds. I trained at a time when clinical judgement (though hard to obtain) and taking a history were more highly valued. What concerns me is that ‘tracking’ abnormal observations represents a problem – particularly in the hands of non-registered or less experienced registered staff” (Consultant).
- “All infants are at risk – everyone should be monitored to begin with and then decided if observations should continue or not” (Midwife).
Discussion
Responses to the survey reflect the opinion of healthcare professionals in the UK about the EWS and specifically the BAPM NEWTT charts in practice. The results demonstrate that of those who responded, the majority of healthcare professionals concur with the current NEWTT guidelines although some key areas for change were highlighted.
The responses suggest that categories need to be clearly defined and overlap avoided. For example, the view that infants of hypertensive mothers who receive beta-blockers do not need to be in a separate category as they are included under risks of hypoglycaemia. Similarly, themes emerged about aligning guidance with other national guidelines such as matching sepsis risk factors and jaundice management with NICE recommendations.10,11 Responses also reflected changes in practice such as the use of the sepsis risk calculator,12 which need to be taken into account when designing the new guidance. Comments also raised concerns about the definition of what needs ‘urgent’ review and that such situations should be clearly defined to balance between unnecessary alarm and appropriately escalating those who require urgent response.
The purposes and manner in which the charts are used were also questioned. We were asked to consider if full NEWTT observations were required for infants at risk of hypoglycaemia. Similarly, the utility of recording bilirubin measurements without appropriate graphs was questioned. Some conditions such as intrapartum compromise and maternal pethidine use were highlighted as clinical situations where infants would need closer observation in the first few hours after birth but would not necessarily benefit from a prolonged period of NEWTT observations.
The responses clearly demonstrate the wide differences in opinion among healthcare professionals and the paucity of evidence to support the recommendations. The limitations of this work are that similar to all surveys, the results represent opinions of individual practitioners and do not equate to evidence. Most respondents did not suggest major changes. Opinions, particularly when expressed by a small number of respondents, should not mandate change in guidance where evidence or the lack of evidence suggests otherwise. However, taking these opinions into consideration when revising the guidance can help with creating consensus and improving the acceptance of the tool. While the need to monitor infants on postnatal wards, transitional care and other low-risk areas prompts the creation of tools such as the BAPM NEWTT, their clinical efficacy in preventing adverse outcomes such as death or long-term harm remain unproven. In an area where there is very little evidence to guide practice, this survey provides an insight into how the users of the tool see it developing. The strength of this work is that it harnesses the opinions of a large sample of healthcare professionals from the whole range of disciplines involved in the care of the newborn. Taking these views into account while revising the BAPM NEWTT guidance may improve the acceptability and utility of the tool.
Conclusion
The survey provides better understanding and a subjective view of:
- knowledge of the extent of use of newborn EWS in UK neonatal practice.
- the opinion of healthcare workers on the clinical priorities relevant to the generation of newborn EWS
- information that may help improve future versions of newborn EWS.
Most healthcare professionals in the UK who responded to the survey, appear to concur with the BAPM recommendations on the use of EWS in the care of newborn infants. Several elements were identified as benefitting from review.
A revised version should include clearer instructions, avoid unnecessary recordings, and align itself with national guidance and emerging practices. In the absence of high-quality evidence, taking these views into consideration can improve the acceptability of the revised tool.
The BAPM working group has taken the views gathered through this survey into account and a revised version of the BAPM NEWTT tool will be published in 2022.
Acknowledgement
The authors extend thanks to the healthcare professionals who responded to the survey and to Kate Dinwiddy, Chief Executive of BAPM, for her help with disseminating the survey.
Or read this article in our
Tablet/iPad edition
- Neonatal early warning scores are used to identify impending deterioration in at risk newborn infants.
- Users of the BAPM NEWTT tool mostly agree with current recommendations.
- Incorporating the views of healthcare professionals who made suggestions for change may improve the acceptability of the revised tool and permit universal implementation.
Also published in Infant:
