

Deterioration of the Newborn Framework for Practice: more than an observation chart
Kathryn Macallister
Neonatal Registrar, University Hospitals Bristol and Weston NHS Foundation Trust
kathryn.macallister2@uhbw.nhs.uk
Shalini Ojha
Clinical Associate Professor of Child Health, University of Nottingham
Wendy Tyler
Consultant Neonatologist
On behalf of the Deterioration of the Newborn British Association of PerinatalMedicine working group
Macallister K., Ojha S., Tyler W. Deterioration of the Newborn Framework for Practice: more than an observation chart Infant 2023; 19(2): 42-44.
The Deterioration of the Newborn Framework for Practice1 was published by the British Association of Perinatal Medicine (BAPM) in January 2023 and seeks to improve the early detection of potentially unwell newborn infants and to standardise the multidisciplinary team’s approach and response.
What began as a project to review and update the Newborn Early Warning Track and Trigger (NEWTT) chart evolved into a larger piece of work in collaboration with the National Maternity and Neonatal Safety Improvement Programme (MatNeoSIP) to create a deterioration of the newborn framework to be launched alongside the new Maternity Early Warning Score tool. Together, these frameworks and tools will contribute to MatNeoSIP’s aim to improve the safety and outcomes of maternal and neonatal care by reducing unwarranted variation and provide a high-quality health care experience for all women, babies and families across maternity and neonatal care settings in England.2 This complements BAPM’s strategic aim to deliver high quality perinatal care and to provide high quality resources to improve practice.3
The guidance was developed according to the PIER framework4 (FIGURE 1) which promotes planning and preparation to identify those babies most likely to be unwell, identification of unwell babies using the NEWTT2 observation chart, structured escalation to the neonatal team and a timely and consistent response.
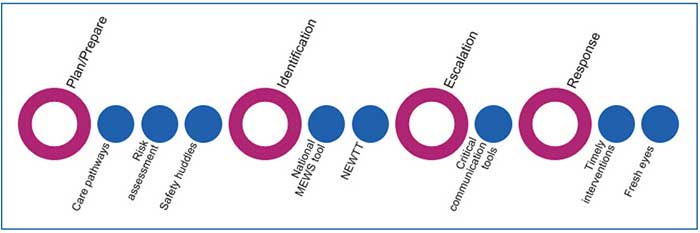
FIGURE 1 NHS National Patient Safety Improvement Programme PIER principles applied to NEWTT2.4
Which babies should be monitored using the tools?
The framework includes up-to-date guidance for all infants who are more at risk of deterioration after birth and who should therefore undergo a period of observation using the NEWTT2 chart (TABLE 1). Specific factors related to maternal health, pregnancy, delivery and the early postnatal period have been identified as warranting additional monitoring.
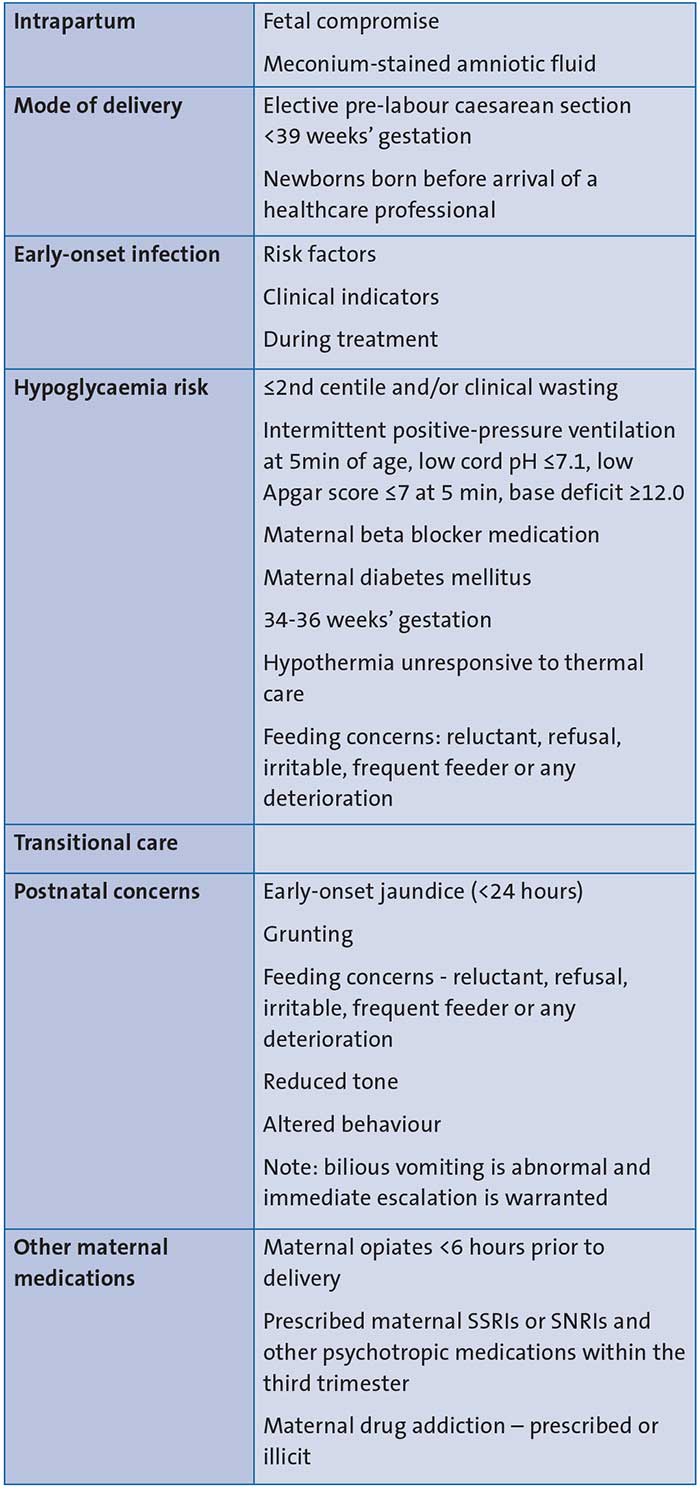
TABLE 1 Risk factors related to maternal health, pregnancy, delivery and postnatal concerns that warrant monitoring on a NEWTT2 chart. Key: SSRI=selective serotonin reuptake inhibitor; SNRI=serotonin and norepinephrine reuptake inhibitor.
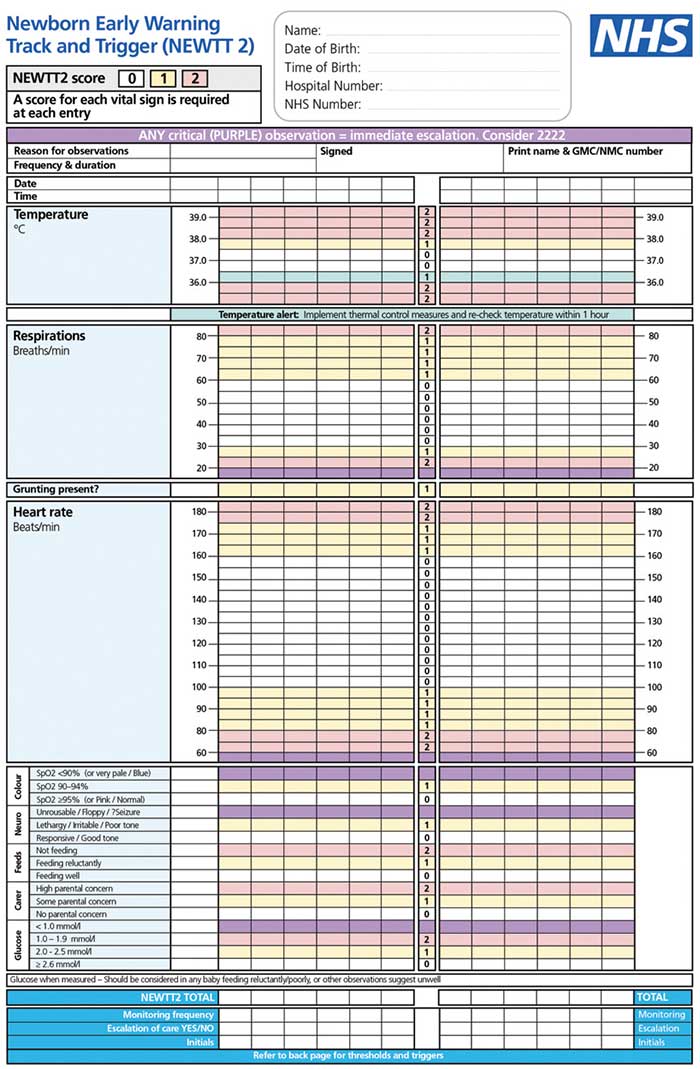
FIGURE 2 The NEWTT2 chart.
The NEWTT2 chart
The first BAPM NEWTT chart was published in 2015.5 A survey conducted in 2021 showed that 92% of UK neonatal services use a neonatal observation chart and that 79% of these used the BAPM NEWTT chart.6,7 This chart was updated in line with current available evidence and consensus opinion to create the NEWTT2 chart (FIGURE 2). This chart is available to download on the BAPM website.1 Key changes include:
Numerical score
Observations plotted on the chart are now assigned a score of 0, 1 or 2 and a ‘total NEWTT2 score’ is calculated for each set of observations. This in turn determines whether any intervention or escalation is required.
Temperature alert
A temperature of 36-36.5°C is plotted in a new blue zone on the chart with a reminder to implement thermal control measures and re-check the temperature within one hour.
Parental/carer concern
This is documented on the chart and can score 1 or 2 depending on the level of concern. The framework stresses the importance of specifically asking parents if they are worried about their baby and empowering parents to speak up if they are concerned.
Glucose
Glucose should only be measured in those infants with risk factors for impaired metabolic adaptation, altered feeding behaviour or abnormal clinical signs that may suggest hypoglycaemia. The results of any glucose measurements should be managed as per the BAPM hypoglycaemia framework,8 and a glucose value of
2.0-2.5mmol/L should be considered normal in asymptomatic term infants without risk factors for hypoglycaemia.
The escalation pathway
A key feature of the new framework is the guidance on appropriate escalation depending on a total NEWTT2 score (FIGURE 3). This aims to minimise variation in escalation timing, the seniority of neonatal/paediatric staff who are contacted and the speed of response. By defining the ‘when to escalate’, ‘who to contact’ and the expected response time, the framework aims to provide a consistent approach to babies who are potentially deteriorating regardless of their place of care.
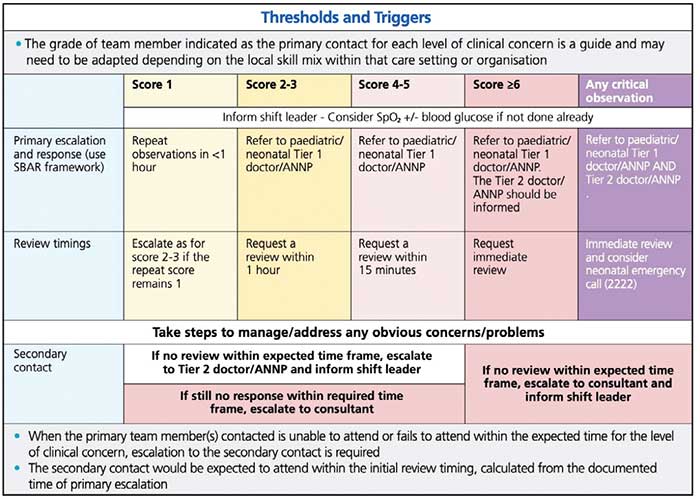
FIGURE 3 The NEWTT2 escalation pathway.
Escalation and response tools
Given the many demands placed on the perinatal team, the framework seeks to standardise and simplify the escalation and review process by providing templates for escalation and review (FIGURE 4). These can be used as paper documents or electronic forms and should replace existing documentation to streamline the review process and to act as checklists to ensure key issues are identified and acted upon. A combined escalation and review record is also available in the framework and can be downloaded from the BAPM website.1
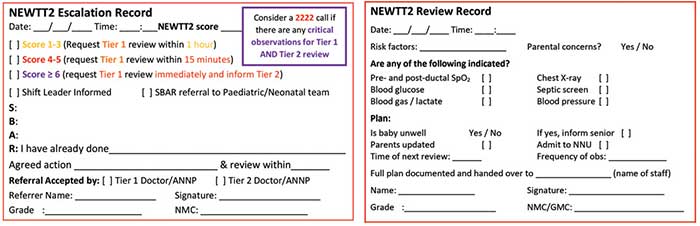
FIGURE 4 NEWTT2 escalation and review records.
Parents
Parents are placed at the heart of the new framework, with regular reminders to elicit any parental concerns and to update parents at every stage. The inclusion of parental concern as an observation on the NEWTT2 chart ensures that parents are truly listened to and that the perinatal team responds appropriately. The framework recognises the need to balance monitoring of babies to improve safety in the postnatal period with minimising disruption to the bonding between parents and their baby or babies at this very special time.
Case study
Rose is a 38 weeks’ gestation infant born through thick meconium who started grunting at birth. She was reviewed by the neonatal team at two hours of age when her NEWTT2 score was 3 (FIGURE 5), but the grunting settled at this time, and everyone agreed that Rose should stay with her parents and observations should continue. Rose remained well for a period but at 12 hours of age she was grunting, feeding poorly and had a number of abnormal physiological observations. Her total NEWTT2 score at this time was 8. The midwife contacted the neonatal tier 1 doctor for an immediate review and also informed the tier 2 doctor. They reviewed Rose promptly and she was admitted to the neonatal unit for respiratory support.
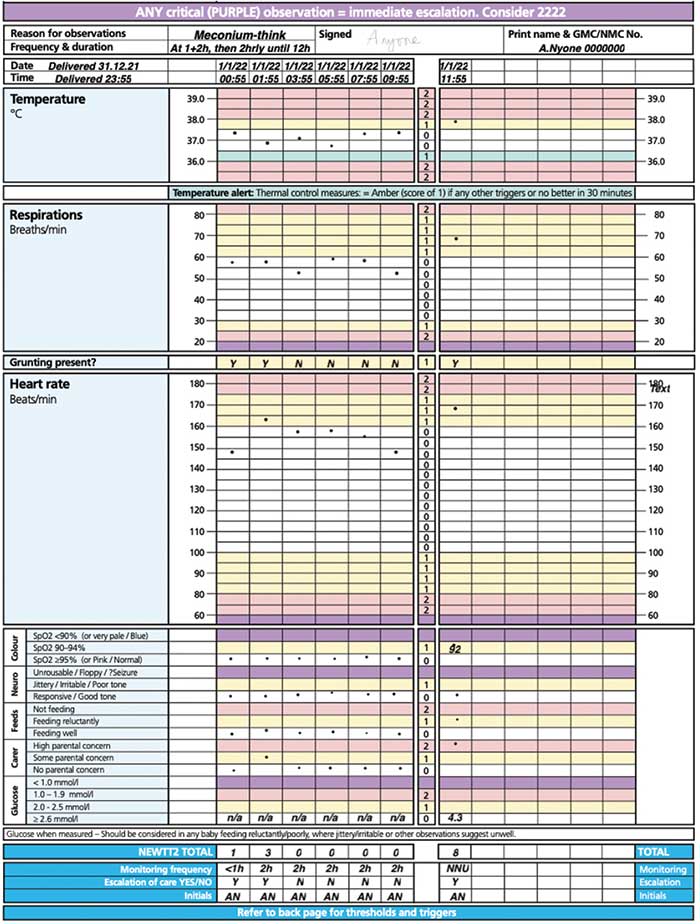
FIGURE 5 Rose’s observations on the NEWTT2 chart.
What does the future hold?
With the publication of this new framework comes a responsibility to ensure it is implemented safely across the UK and that its effectiveness is formally assessed. Ongoing work will include:
Support for NHS trusts
In England the regional Patient Safety Collaboratives will support trusts to implement the framework. Contacts for England, Scotland, Northern Ireland and Wales are on the BAPM NEWTT2 webpage.1
Digitalisation
There is ongoing work with providers to create digital observation charts and escalation and response documents.
E-learning
Health Education England will facilitate the provision of an interactive, online learning module to support healthcare professionals who will be using this framework.
Research into the utility of the framework
There is little objective evidence to demonstrate that neonatal early warning scores prevent deterioration and reduce morbidity and mortality.7 This framework relies on consensus views and previously accepted thresholds for what is normal. It is vital that the impact of introducing such a framework on the outcomes for infants and their families, and maternity and neonatal services is monitored and evaluated to provide the evidence to support future improvements in care.
Conclusion
The Deterioration of the Newborn Framework provides a comprehensive approach to the detection and management of infants at risk of becoming unwell in the postnatal period. It promotes collaborative working within the wider perinatal team and encourages staff to involve parents throughout. Analysis of the effectiveness of implementation of this framework will allow further improvements in safety for this group of patients.
Acknowledgement
The authors and BAPM would like to thank the working group, the survey and consultation respondents and all those that contributed to the development of this framework and participated in the testing phases.
Or read this article in our
Tablet/iPad edition
