

Renal profiles in extreme prematurity: a three-year review
In this study we review the serum urea and serum creatinine of 74 premature infants born under 27 weeks’ gestation over a three-year period. We follow the progression of their renal profiles from birth until discharge. We assess the impact of gestation, birth weight, gender and antenatal medications on these renal biomarkers.
Faezeh Sakhinia1
Paediatric ST7 Renal GRID Trainee
faezehsakhinia@doctors.org.uk
Chris Worth2,3
Clinical Research Fellow in Congenital Hyperinsulinism and Doctoral Researcher in Computer Science
Archana Mishra4 Neonatal Consultant
1Department of Paediatric Nephrology,
Royal Manchester Children’s Hospital
2Department of Paediatric Endocrinology, Royal Manchester Children’s Hospital
3Department of Computer Science, University of Manchester
4Department of Neonatology,
Royal Bolton Hospital
Survival rates of extremely premature infants are improving with advancing neonatal care. However, little is known about their renal physiology. Nephrogenesis begins in the fifth week of gestation and completes between weeks 34 and 36.1 Infants born before 27 weeks’ gestation are classified as extremely premature and suffer a disruption in this process.1-3 This results in an increased risk of acute kidney injury (AKI) and chronic kidney disease (CKD).2
Serum urea (SUr) and serum creatinine (SCr) are widely employed markers of renal function.1 Two decades ago, SCr commonly peaked to the hundreds in these infants.4 However, since the introduction of postnatal caffeine citrate in 2006,5 along with greater awareness of neonatal AKI,1 there has been a paucity of studies examining the pattern of renal biomarkers in extreme prematurity. In particular, there are no recent studies reviewing the renal profile of infants born under 24 weeks’ gestation.
We therefore studied the trend in SUr and SCr in extremely premature infants over a three-year period. The impact of gestation, birth weight, gender and use of antenatal magnesium sulphate and dexa-methasone on these values was assessed.
Methods
The Royal Bolton Hospital is a large tertiary neonatal unit that manages infants within the Greater Manchester area. There are around 600 admissions to the unit per year with around 30-40 babies admitted at <27 weeks’ gestation.
Retrospective data were collected for all infants born under 27 weeks’ gestation over a three-year period between January 2017 and December 2019. SUr and SCr were recorded at birth, days two and seven, and at discharge. The impact of gestation, birth weight, gender and antenatal medications was assessed.
Data were analysed using Microsoft Excel 2019 and IBM SPSS Statistics 25. Relation of gestational age on SUr and SCr was assessed using Pearson correlation. To adjust for confounding factors (gender, birth weight, administration of antenatal magnesium sulphate and dexamethasone), a linear regression analysis was undertaken.
The colorimetric urease method was used to measure SUr and the enzymatic method using creatinase was used to measure SCr on the Roche Cobas 701 system.
Ethical approval was not required since this study was a retrospective evaluation of service.
Results
Between January 2017 to December 2019, 98 extremely premature infants received treatment in the Royal Bolton Hospital neonatal unit. Of this cohort, six died prior to discharge and 18 were born at an alternate hospital. To enable accurate analysis of SUr and SCr, these infants were excluded from the study.
The remaining 74 infants were born at a mean gestation of 25+2 weeks (range 22+4 to 26+6) with 43 (58%) being male (TABLE 1). Sixty-six patients (89%) received antenatal dexamethasone and 56 (76%) received antenatal magnesium sulphate. All infants were commenced on caffeine citrate postnatally from birth until at least 34 weeks’ corrected gestation.
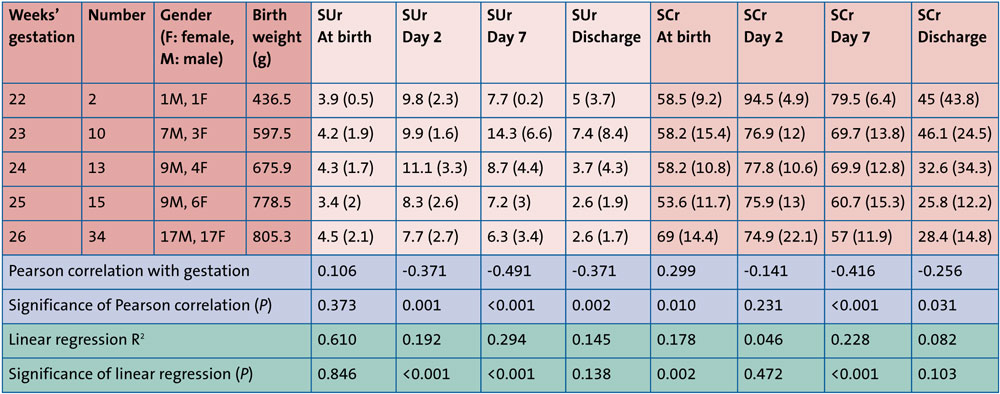
TABLE 1 Participant demographics, serum urea (SUr; mmol/L) and serum creatinine (SCr; µmol/L) in relation to gestation. Values of SUr and SCr expressed as mean (standard deviation). Pearson correlation coefficients reported with significance expressed as two-tailed p-value. Linear regression analysis included gestation, SUr, SCr, birth weight, gender and use of antenatal magnesium sulphate and dexamethasone.
SUr and SCr peaked on day two in all infants, with those born at 23 weeks showing a continuing rise in SUr until day seven (TABLE 1 and FIGURE 1).
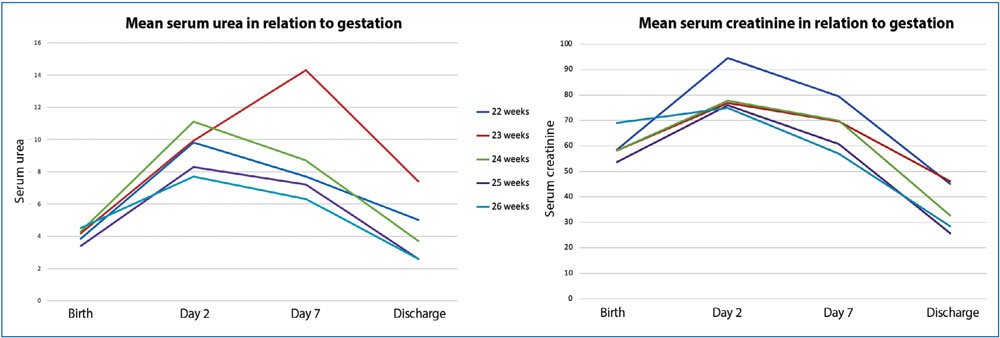
FIGURE 1 Trends in mean SUr (mmol/L) and mean SCr (µmol/L) from birth to discharge in relation to gestation.
Higher gestational age was associated with higher values of both biomarkers at birth (Pearson correlation 0.106 and 0.29, respectively) with significance seen in SCr (p=0.01) but not SUr (p=0.37). After birth, SUr and SCr consistently showed statistically significant inverse correlations with gestational age in all values but SCr on day two (TABLE 1). When adjusted for confounding factors, significance remained for all values other than those at discharge.
Linear regression analysis revealed no significant impact of: birth weight; gender; use of antenatal dexamethasone and magnesium sulphate on SUr or SCr.
Discussion
The primary objective of our study was to obtain a picture of SUr and SCr in extremely premature infants and to assess their relationship with gestational age. We demonstrated that with increasing gestation, higher values of SUr and SCr are seen at birth. Following this, there was an inverse correlation indicating that infants born at a later gestation had improved renal function post-birth. Significance of gestation on SUr and SCr on day seven of life highlights that variation of renal biomarkers cannot be solely attributed to the presence of maternal creatinine. It was not possible to measure maternal creatinine in these patients but these findings exhibit the multifactorial influences governing renal function in these vulnerable patients.
The lack of a statistically significant relationship between gestation and SCr at discharge may reflect the limitation of creatinine as an indicator of renal function in patients with low muscle mass. Alternatively, this may simply represent a normalisation of SCr after the inevitably long inpatient stay of infants born under 27 weeks’ gestation. In recent years, cystatin C has been favoured in monitoring renal function. This protein is unaffected by muscle mass and is more reliable in neonates.1 Unfortunately, this is not yet widely available but we suggest that future studies measure its relationship with gestational age.
Twenty years ago, Gallini et al assessed the renal profile of infants born under 32 weeks’ gestation, including 12 infants born under 27 weeks.4 They noted a rise in SCr in the first 36-96 hours, peaking at 128.5µmol/l on day four of life. Estimated SCr values of 60-70µmol/L at birth, 90-100µmol/L on day two and 100-110µmol/L on day seven were presented. More recently, in 2020 Monzani et al noted a mean SCr of 77.8µmol/L on day three of life in 31 infants born under 28 weeks’ gestation.3 Patients in our study had a mean SCr of 62µmol/L at birth, 76µmol/L on day two and 62µmol/L on day seven, more closely reflecting those values repor-ted by Monzani et al. This demonstrates the significant improvement in measures of renal impairment in extremely pre-mature infants over the last two decades.
Both Monzani et al and Gallini et al analysed these extremely premature infants as a group.3,4 In contrast, we have assessed renal profiles by gestational week and have also included patients born under 24 weeks’ gestation. Combined with our larger cohort this has enabled a more detailed and reliable description of the renal biochemistry of extremely premature infants managed in a modern neonatal unit. Our study was unable to assess the impact of potential confounding factors, including antenatal and postnatal nephro-toxic medications and sepsis. Future work should include these in their analyses.
Through provision of up-to-date information on renal profiles of extremely premature neonates, our data acts as a reference point for neonatologists. This baseline data will facilitate earlier recognition of AKI and dismiss assum-ptions that deranged renal function is purely secondary to extreme prematurity. We also highlight that a neonate born at 22 weeks’ gestation harbours an increased vulnerability to derangement of SUr and SCr compared with an infant born at 26 weeks’ gestation. Our findings should therefore prompt all clinicians caring for extremely premature infants to pay close attention to SUr and SCr.
Conclusions
In the 74 patients studied, mean SCr peaked at 76µmol/L on day two. SUr and SCr showed inverse correlations with increasing gestational age from day two of life. Gender, birth weight and antenatal medications showed no effect on either value.
We provide the first up-to-date detailed description of SUr and SCr in extremely premature infants by gestational age. We demonstrate that infants born at an earlier gestation have higher values of SUr and SCr after birth.
Author contributions
FS and AM designed the study while FS was involved in data collection and literature review. CW and FS analysed the data and wrote the paper. All authors were involved in the final editing process.
Or read this article in our
Tablet/iPad edition
- With increasing gestation, higher values of serum urea and creatinine are seen at birth, followed by an inverse correlation from day two of life.
- Since the introduction of caffeine citrate and better awareness of neonatal acute kidney injury, we demonstrate an improvement in renal profiles of extremely premature infants.
- We provide the first detailed description on the renal biomarkers of infants born under 24 weeks’ gestation.
Also published in Infant:
