

‘GO to Mum’: a QI project to keep mothers and babies together
This article presents a quality improvement (QI) project aimed at keeping mothers and babies together after delivery. The effectiveness of QI interventions in reducing the number of short-stay transfers of newborn term babies to the neonatal unit (NNU) due to grunting respirations is reviewed. An inter-departmental collaborative approach is described that resulted in the development of a novel programme to facilitate the safe monitoring of term newborn babies with grunting respirations in the labour and postnatal ward with their parents, averting transfer to the NNU.
Lavinia E. Raeside
Advanced Neonatal Nurse Practitioner
lavinia.raeside@ggc.scot.nhs.uk
Rhona Wilson
Advanced Neonatal Nurse Practitioner
Julie Gallagher
Charge Midwife, Labour Ward
Lesley Jackson
Consultant Neonatologist
Neonatal Unit, Royal Hospital for Children, Queen Elizabeth University Hospital, Glasgow
The problem
There is overwhelming evidence that separating mothers from their babies after birth has long-term detrimental effects on mother-baby attachment, breastfeeding and maternal health.1 Evidence supports uninterrupted skin-to-skin care for all stable babies, regardless of mode of delivery or feeding preference.2 This is further highlighted by national reports such as Best start: a five-year strategy plan for the improvement of maternity services in Scotland3 and the ATAIN programme (avoiding term admissions into neonatal units).4
There are many reasons why a baby may be at risk of becoming unwell after birth. Respiratory admissions, however, have been reported as the most frequent cause of unexpected term admissions to the NNU.5
It has been identified that over 20% of admissions of full-term babies to NNUs could be avoided. The harm caused by maternal-infant separation could be prevented by adapting services and models of care to facilitate keeping mothers and babies together.6-8
Background
Term respiratory short-stay admissions were reviewed at a regional NNU in Glasgow. Data reflected that over a period of one year, 60% of term newborn babies who were transferred to the NNU for a period of observation due to grunting respirations did not require admission and were transferred back to their mothers within four hours. These results identified a significant number of babies who were unnecessarily separated from their mother around the time of birth. This not only had an effect on maternal-infant bonding but also had an impact on flow of patients through the labour ward and acuity in the NNU and postnatal wards.
The aim of this project was to put mother and baby at the heart of a process to minimise unnecessary maternal-infant separation after birth and reduce the number of unexpected term admissions to the NNU for babies with grunting respirations.
Baseline measurements
In order to review the numbers of short-stay admissions, baseline data were reviewed over a 12-month period from May 2018 to April 2019. Data reflected that 51 term babies (60%) were transferred to the NNU for short-term observation of grunting respirations; none of these babies required admission to the NNU and were returned to their mother within four hours (FIGURE 1). Within this group, 39% (n=33) were admitted for ongoing care. These were separations that potentially could have been avoided by keeping babies with their mum under observation and frequent review.
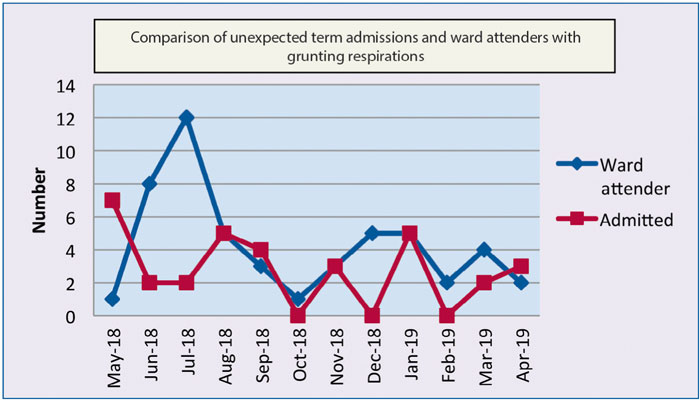
FIGURE 1 Baseline data: understanding the problem.
Aims of the project
- To study the effectiveness of QI interventions in reducing the number of short-stay transfers of newborn term babies to the NNU due to grunting respirations.
- To reduce the number of unexpected short-stay term respiratory admissions transferred to the NNU with:
– a target of 5% by August 2020
– a target of 10% by August 2021.
- To minimise maternal-infant separation, promote bonding, breastfeeding and reduce acuity in the NNU, labour ward and postnatal area.
Methods
A multidisciplinary, collaborative group was developed consisting of staff from the labour ward, delivery theatre, postnatal ward and NNU comprising neonatologists, midwives and advanced neonatal nurse practitioners (ANNP). The team’s role was to evaluate factors contributing to short-stay respiratory admissions of term babies with grunting respirations and develop a programme of care aimed at reducing the number of term babies transferred to the NNU for observation. During the first team meeting, it was decided that a pathway should be devised to enable babies with post-delivery grunting respirations to be safely cared for beside their parents.
Evidence-based measures were adopted to address the causes of short-stay respiratory admissions. In addition to the usual management of term babies with grunting respirations (eg monitoring vital signs), new processes were tested and implemented using the plan, do, study and act (PDSA) framework.
The grunting baby protocol and flow chart
The group developed a protocol for the project (FIGURE 2) with inclusion criteria as term babies (≥37 weeks’ gestation) with no risk factors, presenting with grunting respirations in the first four hours post-delivery.
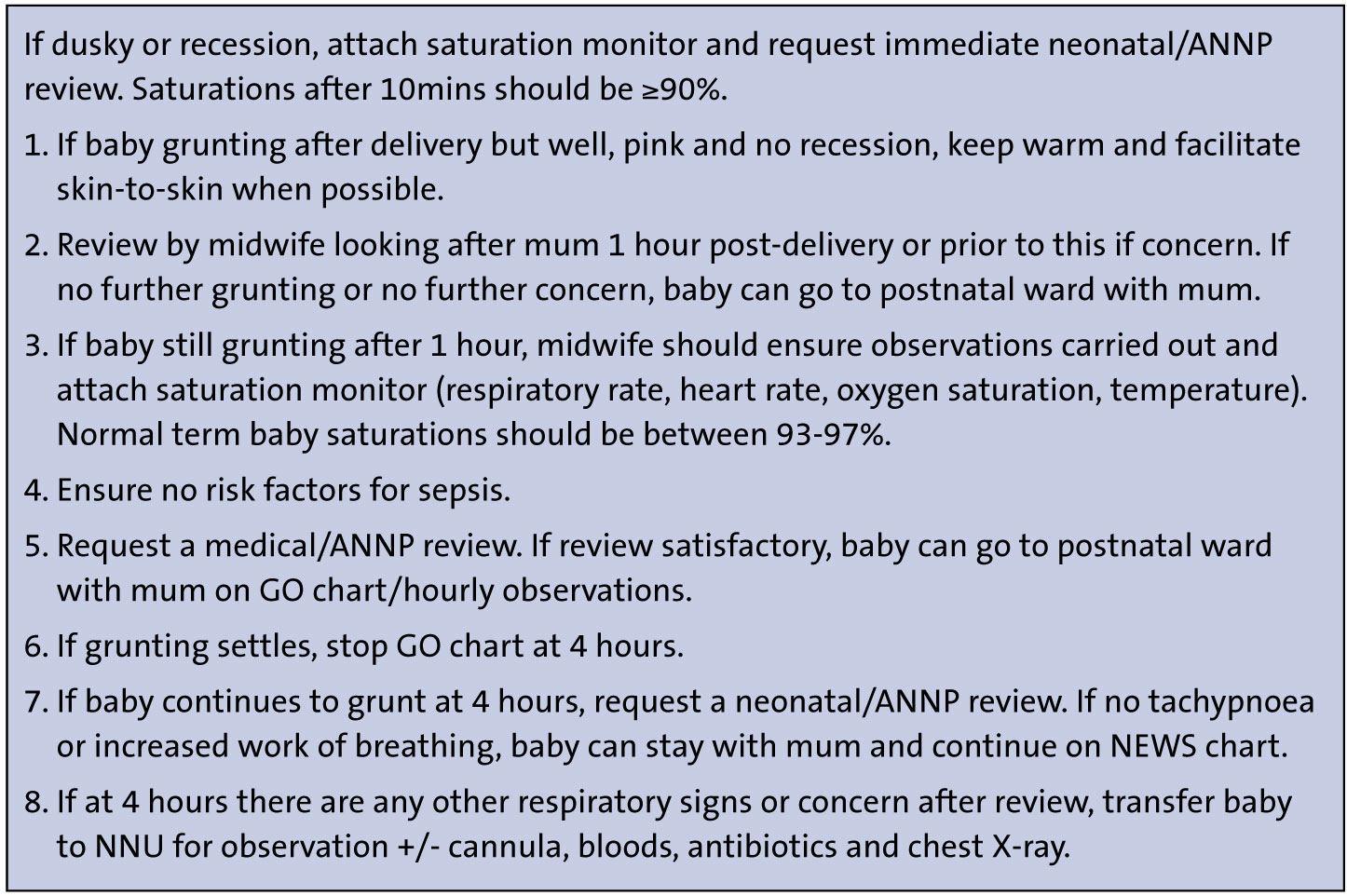
FIGURE 2 The term baby (≥37 weeks’ gestation) grunting protocol. Key: GO=grunting observations; NEWS=newborn early warning score.
For ease of use, a flow chart of the protocol was produced. Numerous versions of the flow chart were discussed and it was decided that a traffic light system would be the best way to highlight quick and efficient escalation of care, if required (FIGURE 3).
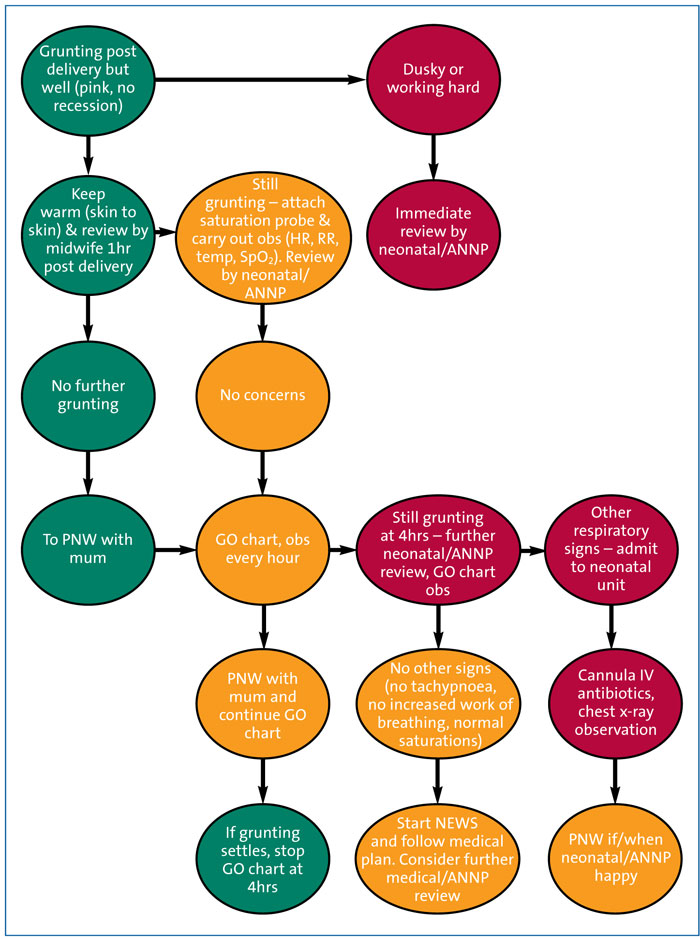
FIGURE 3 The grunting baby flow chart. Key: PNW=postnatal ward; obs=observations; HR=heart rate; RR=respiration rate; SpO2=oxygen saturation; ANNP=advanced neonatal nurse practitioner; NEWS=newborn early warning score; GO=grunting observations.
Both the agreed protocol and flow chart were added to the GO – grunting observations – chart to ensure uniformity. The ‘GO to Mum’ chart consisted of patient details and an observation chart for vital signs and oxygen saturation. These observations were recorded and documented on the GO chart at hourly intervals while in labour ward and continued in the postnatal wards.
Once the GO chart format was agreed, training sessions on the use of the chart and saturation monitoring were arranged. Extra saturation monitors were purchased to ensure the availability of required equipment. A patient information leaflet (PIL) for parents was produced and tested with postnatal women. The PIL had information explaining what the ‘GO to Mum’ programme involved, what caused their baby’s grunting respirations and what parents could do to help be involved in their baby’s care.
Once all staff involved in the care of grunting babies were trained in the use of the GO charts, the protocol, flow chart and correct monitoring, a 30-day countdown was initiated, which was displayed in all areas so that the launch date was known well in advance. These posters had the GO logo and countdown date for all staff to see. Champions within each area were appointed to ensure good communication and to ensure the collection of data. The project was also highlighted at all nursing and medical handovers.
Strategy
During the first two months following the launch, early tests of change were identified using the PDSA cycle of change. Data were collected before, during and after each intervention. A total of three PDSA cycles were conducted and each was followed by a review of the data and modifications to the GO documentation prior to the next cycle.
The primary outcome measure was the incidence of babies transferred to the NNU for short-stay review due to grunting respirations. Secondary outcomes were any adverse events and the number of admissions to the NNU within this group.
PDSA cycle 1 intervention
The GO protocol and design was developed for introduction into each clinical area, incorporating the guideline and algorithm for management of the baby with grunting respirations. This consisted of entry criteria for the GO programme, timing of neonatal reviews, observations and red flags for immediate referral for review. The aim was to improve the midwives’ confidence in managing a baby with grunting respirations in the labour ward and the postnatal area, while ensuring that babies were appropriately and safely managed. Vital signs monitoring (including oxygen saturation) was carried out hourly for four hours. Any deviations from normal were reported to the neonatal staff and an immediate review requested. If the baby was still grunting at four hours, a neonatal review was carried out with a management plan.
Information was circulated around the clinical areas in staff and patient areas. Feedback was invited from all members of staff.
PDSA cycle 2 intervention
Following the first PDSA cycle, the data were reviewed and the GO algorithm and the timings of observations were modified in accordance with staff feedback. The PILs were circulated in all clinical areas. Posters and a run chart with updated monthly data were placed on notice boards for staff to review.
PDSA cycle 3 intervention
After the second cycle it was noted that the GO observation charts were being filed in the case notes making access for data collection difficult. A note was therefore stapled to the GO charts to remind staff to file charts in the GO file box and not the patient case notes. A walk round was carried out by members of the GO team to all of the clinical areas to update staff on progress, troubleshoot any questions and maintain momentum.
Results
The GO to Mum project began in August 2019 as a collaboration between the labour ward, postnatal ward, delivery theatre and NNU. Between August 2019 and February 2021, 146 term babies who met the entry criteria were included in the GO to Mum project. The cohort demographics can be seen in TABLE 1. The majority of babies were delivered by elective caesarean section at 39 to 39+6 weeks’ gestation with a birth weight of 3.00-3.49kg.
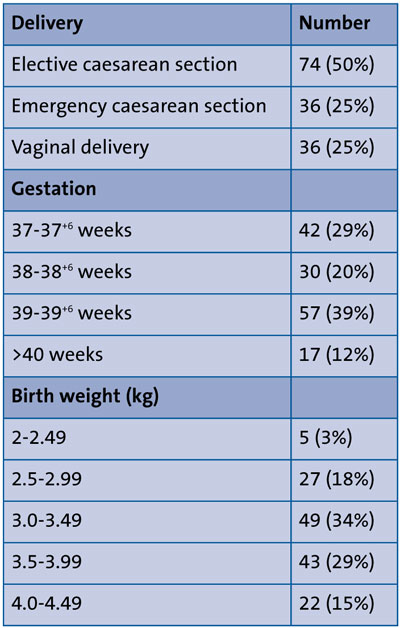
TABLE 1 The cohort demographics (n=146).
Within the group, 128 (88%) babies stayed with their mum in the labour or postnatal ward under the GO protocol. Eighteen (12%) babies were transferred to the NNU; 15 (10%) were admitted and three returned to mum within four hours. Comparison of the baseline median of babies transferred to the NNU for short-stay review with grunting respirations and returned to mum within four hours before and after the GO programme, reflects a decrease in episodes from four per month to zero (FIGURE 4).
With regard to babies requiring admiss-ion to the NNU following commencement on the GO programme with grunting respirations, data reflected a decrease in the baseline median from three episodes per month to one (FIGURE 5). No adverse events were reported during this period.
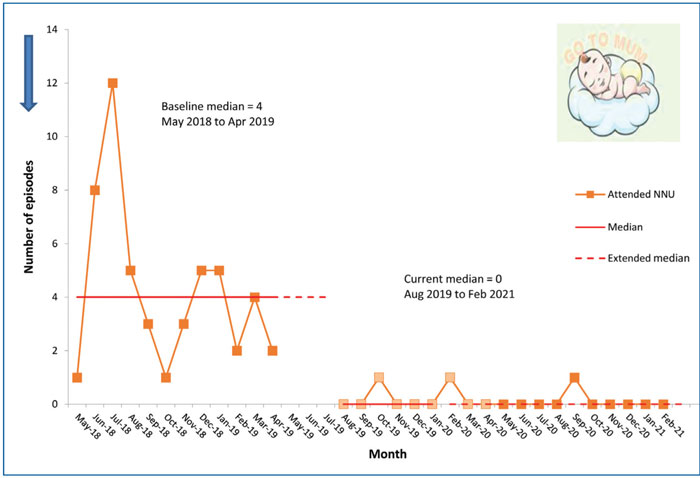
FIGURE 4 Term neonates with grunting respirations: short-stay review in NNU. Comparison of the baseline median of babies transferred to the NNU for short-stay review and returned to mum within four hours before and after the GO programme, reflects a decrease in episodes from four per month to zero.
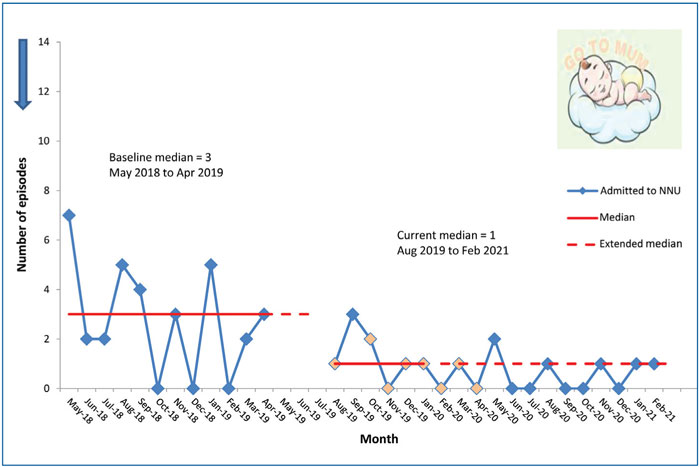
FIGURE 5 Term neonates with grunting respirations admitted to the NNU.
The incidence of transfer to the NNU for short-stay review of grunting respirations decreased from 51 in the year prior to implementation of the programme to 18, constituting a 64% improvement. The target of 10% reduction by August 2021 was exceeded.
Discussion
This QI project reviewed and changed practice and management of short-stay babies with grunting respirations, resulting in a 64% reduction in numbers transferred to the NNU. The results reflect that the majority of babies entered into the protocol were delivered by elective caesarean section – a low-risk category with no risk factors. There were no adverse events reported in babies on the programme, supporting the aim of the project to reduce unnecessary maternal-infant separation and safely monitor babies at the mother’s bedside.
Challenges and successes
Engaging staff groups in different clinical areas can often be difficult, particularly in high acuity areas; nevertheless, inter-departmental working and communication was vital for the success of the project. Maintaining momentum was important, particularly with the backdrop of coronavirus and the high levels of stress and anxiety experienced by both parents and staff. Staff turnover had to be addressed with members of the clinical teams often changing and medical, midwifery and nursing staff rotating in each department. Ongoing education sessions were, therefore, imperative and identifying champions within each area proved crucial for early engagement and ongoing staff education and support to maintain momentum.
An important factor in the success of the project was the effect of a clear and consistent guideline and algorithm for management of the babies in the labour ward and postnatal area. In the early stages it was challenging for staff to get to grips with the documentation but as they became familiar with the new protocols it got easier and implementing minor adjustments following each PDSA cycle proved effective in gathering data and simplifying the process. Initial concern with workload eased as staff became familiar and more confident with the new protocol.
Early on in the project it became evident that the number of babies being transferred to the NNU was reducing and there was an improvement in patient flow through the labour ward to the postnatal areas. The midwives showed confidence in their management and babies were referred and reviewed appropriately.
The changes made after each PDSA cycle included modifying the GO observation chart in line with comments from the midwives, and filing of the GO charts. Working patterns were reviewed resulting in an increased awareness of varying issues in each department, which were addressed. The information posters and run charts were regularly updated for staff to see the difference in the number of transfers. This helped to improve communication and engage staff, as did regular virtual meetings within the team.
Parent feedback assisted by the PIL was very positive. Parents appeared to be well informed of the protocol and were comfortable having their baby monitored by their bedside in the labour or postnatal wards. This project was conducted during the coronavirus lockdown when visitors were not allowed and fathers were not permitted to access the postnatal areas; it was, therefore, even more important to prevent maternal-infant separation at this most difficult time.
Future developments
The GO programme is now embedded within the clinical areas. Data collection is conducted on a quarterly basis and will be extended to six-monthly after 12 months of positive data. Ongoing reliability of the process will be reviewed. The aim of this project was to reduce short-stay reviews in the NNU due to grunting respirations; the long-term intention is to integrate this work with the overall goal of reducing unplanned term admissions to the NNU.
Conclusion
By adopting an inter-departmental collaborative approach, a novel programme was developed that facilitated the safe monitoring of term newborn babies with their mothers in the labour ward and postnatal area. The implementation of evidence-based best practice resulted in a significant reduction in babies transferred to the neonatal unit for short stay review due to grunting respirations. The GO to Mum project reduced the unnecessary separation of mothers and babies in the immediate period after delivery when the initiation of maternal-infant bonding and breastfeeding is most important. This practice is now embedded in our institution as a standard of care.
Acknowledgement
The authors would like to acknowledge all members of the GO to Mum team, which included midwives in the labour ward, obstetric theatres, postnatal ward, and the NNU for enthusiasm in implementation and ongoing support of the project. The authors would also like to thank The Quality Improvement Team, Clinical Governance Support Unit, Greater Glasgow and Clyde, for advice and guidance throughout the project.
Or read this article in our
Tablet/iPad edition
- The implementation of evidence-based best practice resulted in a significant reduction in babies transferred to the NNU for short-stay review due to grunting respirations.
- This prevented unnecessary separation of mother and baby following delivery.
Also published in Infant:
