

Impact of COVID-19 on term admissions to neonatal care
This article analyses a retrospective study of the impact that the COVID-19 pandemic has had on term admissions to the neonatal intensive care unit (NICU) at Sunderland Royal Hospital. Using data gathered between 1 January 2020 and 31 December 2020, the results from this repeat audit are compared with admission data from previous years and with figures from NHS England. This audit considers the impact of the pandemic on term admissions to the NICU, with a focus on social causes and other potentially avoidable reasons for admission.
James M. Hardy
Medical Student
Newcastle University Medical School
Sabina Iqbal
Medical Student
Newcastle University Medical School
Ruppa M. Geethanath
Neonatal Consultant, Neonatal Intensive Care Unit, Sunderland Royal Hospital
ruppa.geethanath@nhs.net
Background
NICUs are primarily designed and equipped to manage preterm infants yet, despite this, three out of every five (62%) neonates admitted to the neonatal unit are born at full term.1 More than 20% of these term admissions could be avoided2 and these beds could be used by those with greater medical needs, such as extreme preterm infants. Importantly, mother and baby are separated in the process, which can have a significant impact on bonding, breastfeeding and development.3,4
Avoiding Term Admissions into Neonatal units (ATAIN) is an initiative launched by NHS England, which looks to minimise avoidable admissions.5 ATAIN focuses on four main causes for admission:
- respiratory conditions
- jaundice
- hypoxic ischaemic encephalopathy (HIE)
- hypoglycaemia.
Sunderland Royal Hospital (SRH) has been found to have disproportionately high term admissions for social reasons when compared to the UK average. The importance of highlighting these social admissions as a fifth area of focus for continued development at SRH has been described in previous audits.6,7
The aim of this audit is to identify reasons for term admissions, draw comparisons with available data and suggest recommendations for future practice. This article will also focus on the impact that COVID-19 had on NICU admissions in 2020.
Methodology
Audits at SRH NICU continue to identify trends and areas for improvement when repeated yearly. Therefore, this is the latest retrospective study to analyse admission patterns. Findings in this article are compared with previous audits published in Infant in 2015 and 2016.6,7 The audit was registered with South Tyneside and Sunderland NHS Foundation Trust. The data were selected to include all term neonates (≥37 weeks’ gestation) admitted to the NICU between 1 January 2020 and 31 December 2020, irrespective of the level of neonatal care.
We selected term infants that were inborn or admitted (readmissions) from home, removing those born at other hospitals. The decision to exclude these infants from the study population was made because transfers from other hospitals are admitted for medical needs that SRH can support. Therefore, infants transferred from other hospitals are likely to have been unavoidable admissions and unsuitable for consideration.
BadgerNet was used to identify patients for the study population. The application software, MediTech, was used to gather information from neonatal discharge summaries and maternal health records. This was collated using a proforma in Microsoft Excel. Factors recorded included:
- gestational age
- source of referral (ie inborn, born elsewhere or from home)
- reason for admission and discharge diagnosis
- level and duration of respiratory and/or inotropic support
- mode of delivery
- if the patient was born by caesarean section (C-section):
- whether this was elective or emergency
- the reason for the C-section
- if it was elective and the mother was eligible for antenatal steroids (ANS; before 39 weeks’ gestation), were they given?
- duration of stay
- use of antibiotics
- outcome, ie discharge or transfer.
These variables allowed for an in-depth analysis of the neonates’ time on the unit and reasons for admission. The results were then compared to previous years and the national NHS England data to identify any trends. These UK figures are derived from those provided by NHS England and the Neonatal Data Analysis Unit (NDAU) between 2011 and 2013.8 The NDAU reviews the data held by the National Neonatal Research Database (NNRD), which gather figures from neonatal units across the UK.
Results
There were 123 term admissions to the NICU between 1 January 2020 and 31 December 2020. This represents 34% (123/357) of all admissions to the NICU in 2020. Of these 123 term admissions, 105 were inborn or admitted from home. The 18 babies that were born at other sites were excluded as they were deemed unavoidable. While the proportion of term admissions to SRH had been steadily falling between 2014 and 2019, the results for 2020 show a rise of 6% from the previous year. These trends are shown in FIGURE 1.
Of the selected term admissions, the gestational age at birth was most commonly 37 weeks (32%) followed by 39 weeks (27%), which is shown in FIGURE 2. None of the infants were born after 42 weeks and all gestational ages were known. The mean gestational age was 38.6 weeks. There were fewer births between 38-39 weeks and 41-42 weeks (14% and 9%, respectively).
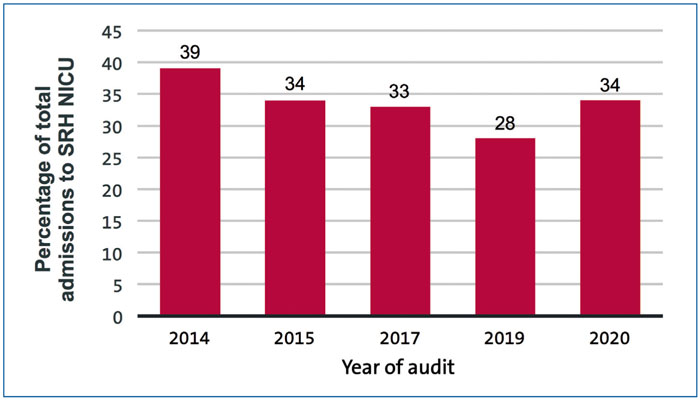
FIGURE 1 Term admissions as a percentage of total admissions between 2014-2020.6,7 Note, no audits were carried out in 2016 and 2018.
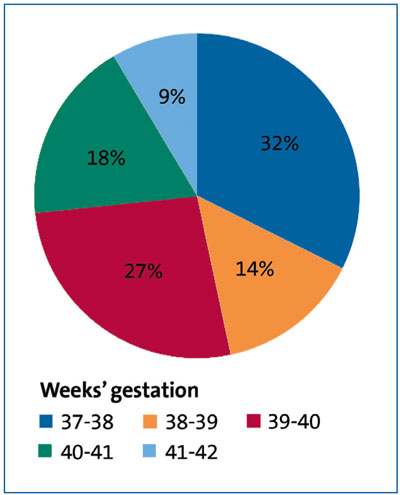
FIGURE 2 The gestational ages at birth of term infants admitted to the NICU. These infants were inborn and/or admitted from home (%, n=105).
The primary reasons for admission were compiled using the MediTech database and its discharge summaries. We then compared our results against previous years and those provided by the NDAU for NHS England, shown in TABLE 1.
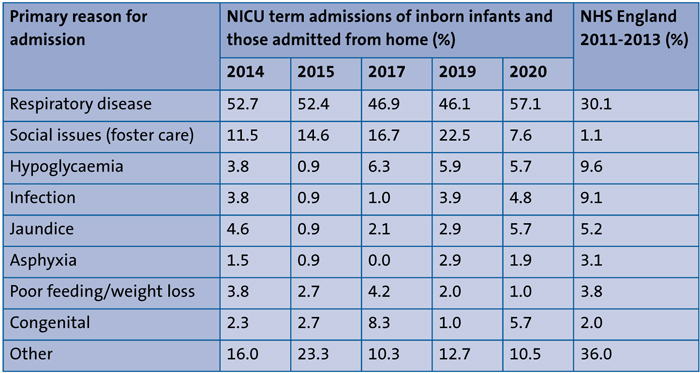
TABLE 1 The main reasons for term admissions to the NICU in 2020, compared with previous years at SRH and NHS England data.6-8
The most common reason for admission continued to be respiratory disease in 2020 (57.1%), which is in-line with previous years at SRH. The proportion at SRH NICU has been noted to be higher than the NHS England data figure of 30.1% in previous audits. There has also been a 2.8% increase in the proportion of admissions for jaundice when compared with 2019.
Social issues (ie foster care) remain the second highest reason for admission. These social admissions have decreased by 65% between 2019 (22.5%) and 2020 (7.6%). Despite this, social admissions at SRH remain higher than the national average (1.1%) so this continues to be an area for improvement. None of the social admissions required respiratory or cardiovascular support, demonstrating that the medical needs of social admissions are, in most cases, minor.
Six of the eight social admissions were related to maternal substance misuse. Two babies required stays of 19 and 30 days for neonatal abstinence syndrome (NAS) withdrawal. All social admissions stayed for at least two days until they were fostered or placed under a child safeguarding plan (supervision and social worker). The average duration of stay for social admissions was eight days, which may reflect the extremes of stay for withdrawal. The median length of stay was three days, showing that most babies stayed for a shorter time.
Admissions for hypoglycaemia and infection were 5.7% and 4.8%, respectively, which remains lower than the NHS England figures of 9.6% and 9.1%.
Additionally, 31% of term admissions were delivered by C-section and two-thirds of these C-sections were emergency (category 1 or 2). There were nine elective C-sections for term admissions. Five of these nine mothers were eligible for ANS, according to the guidelines. Royal College of Obstetricians and Gynaecologists guidelines state that ANS should be given to all elective C-sections before 39 weeks’ gestation.9 All five of these eligible mothers received ANS in line with the guidelines.
Ultimately, of the 105 babies admitted to the NICU, 92 were discharged home, eight were discharged to foster care and five transferred to another hospital.
There appear to be some discrepancies between the data gathered at SRH NICU and NHS England figures. One of the possible reasons could be errors in data entry. NHS England have acknowledged that there are some inconsistencies in their data. Of note, ‘other’ accounts for 19.4% of the 2011-2013 NHS England data, and 9.5% is classified as ‘missing’. These ‘missing’ admissions may have increased the proportions of respiratory or social admissions, for example, had they been correctly documented.
It is worth noting that there were likely to have been admissions to SRH NICU for asphyxia in 2017. It is believed that there may have been an error when categorising admissions as ‘asphyxia’ when this should include infants with HIE. This may reflect inconsistencies in data gathering between each year of re-audit.
Limitations
Some limitations have been identified in this paper, one of them is the data is from a single hospital and the extent to which these findings might be replicated to other neonatal units may be limited. Another limitation is the methods used to decide categories; some of the babies had unknown discharge diagnoses or vague descriptors, which often had many contributing factors. For example, there were some unclear discharge diagnoses such as ‘presumed sepsis’.
Some admissions had multiple contributing reasons and complex diagnoses. This made it more difficult to categorise the admissions and decide whether they were avoidable.
Ultimately, the NHS England data for term admissions is very much outdated (2011-2013), and so is less useful for comparison with the recent SRH NICU data. It also combines data from three years, while the audits at SRH only analyse single years. Some of the NHS England data could be considered inaccurate, as evidenced by 0.2% of ‘term’ admissions having ‘preterm’ as their reason for admission. Furthermore, ‘cardiovascular disease’ and ‘cardiac disease’ were used as separate categories, despite there not being a clear distinction between them. As discussed, 9.5% of the NHS England data are categorised as ‘missing’, demonstrating that some data may have been recorded inaccurately or omitted altogether.
Discussion
While it has been reassuring to see term admissions dropping over recent years, results from 2020 have shown an increase. The reason for this 6% increase in the proportion of term admissions between 2019 and 2020 is unclear. It could be related to staffing shortages during the pandemic, or due to the impact of COVID-19 on health habits, lifestyle and antenatal care.
The number of term admissions due to social reasons has been steady at Sunderland over the years but the average number of days these babies spend in the neonatal unit has reduced as a result of quality improvement measures undertaken in previous years. This included having multiple multidisciplinary team meetings involving midwifery, neonatal and children’s services to have timely, robust birthing plans in place – supervised parenting, finding foster care placements early on, etc. Sunderland children’s services received an ‘outstanding’ rating from Ofsted in 2021 following the number of improvements it made after it received ‘improvement needed’ rating earlier in 2019.
While the figures for social admissions (7.6%) continue to be higher than the national average (1.1%), SRH has seen improvements to its safeguarding services over recent years. It is also worth noting that admission rates have been found to double in the most deprived areas when compared with the most affluent.11 Therefore, it might be useful to view these figures in the socioeconomic context of the healthcare setting at Sunderland and South Tyneside.
Respiratory admissions are the most common reason for admission at SRH (57.1%) and nationally (30.1%). There has been a substantial increase compared to 2019 (up by 11%). This could be a result of inconsistencies in data gathering at Sunderland. ‘Respiratory disease’ includes respiratory presentations of infections at SRH, so this may extend to a wider population than in NHS figures. Infants were only classified as having infections if they were given antibiotics for greater than five days or if they had a positive blood culture.
Jaundice admissions have almost doubled between 2019 and 2020 (from 2.9% to 5.7%). This may be attributable to the impact of COVID-19 on access to breastfeeding support in the early postnatal period. These provisions are believed to have been affected by the reshuffling during the pandemic.
When combining admissions for hypoglycaemia and infection, there is a smaller proportion at SRH (10.5%) when compared with NHS England data (18.7%). This may be due, in part, to the ATAIN programme. This is to be expected given its impact since the NHS England data were gathered in 2011-2013. Additionally, improved care may reflect the success of local protocols and a multidisciplinary approach at SRH. For example, maternal care teams are involved in identifying those at risk for hypoglycaemia and administering prophylactic treatments to those with antenatal infections.
Furthermore, it is reassuring to see that ANS have been given to all mothers who are eligible, according to SRH guidelines (before 39 weeks’ gestation). Continuing to administer ANS to those eligible will reduce avoidable respiratory admissions. ANS have also been shown to reduce neonatal morbidity by reducing respiratory distress syndrome,9 which is common in term infants born by C-section.
The inaccuracies identified in the NHS England data have indicated the need for another national study which is more accurate and, therefore, more comparable with SRH data. As described in previous audits,6,7 this would require national improvements to data entry on an individual healthcare professional level.
As this would be a significant undertaking, it may be more practical to suggest comparisons to study populations on a smaller scale. Collating data from other tertiary units in the region may allow for more accurate comparisons to be drawn.
Impact of COVID-19 on neonatal services
There was not a significant infection rate of COVID-19 for infants admitted to the NICU at SRH in 2020. The most recognisable impact was the restriction of parental visits, thereby limiting the physical contact between parents and their babies.
The other main consequence of COVID-19 in the community was the negative impact on the establishment and continuation of breastfeeding. Possibly, the lockdown constraints prevented mothers from seeking breastfeeding support, which could have delayed establishing breastfeeding. This could have resulted in dehydration and exaggerated jaundice in neonates in the community leading to readmissions to the neonatal unit.
Moreover, there were members of staff in the neonatal unit that were isolating or shielding at times, resulting in staff shortages. The staffing impact on neonatal services was mitigated in part with the redeployment of staff from the paediatric ward and the employment of bank staff to work in the neonatal unit. An audit of staffing in the neonatal unit confirmed that the staff shortage did not have any major impact on the provision of neonatal services at SRH.
Conclusion and recommendations
This audit has shown that SRH has seen substantial improvements to its rate of social admissions in 2020, despite the uncertainties with the COVID-19 pandemic. These social admissions are among other avoidable causes that have been targeted to improve neonatal care for those with greater clinical needs. At SRH, term admission due to social reasons is the second commonest reason for admission to the neonatal unit. Most babies admitted for social reasons are well babies and are admitted here as a place of safety rather than for medical needs. While there is no dedicated transitional care ward at SRH, there is provision of transitional care in the postnatal ward. If we had a dedicated transitional care area manned by nurses/midwives, we could utilise the neonatal beds for those who need them for medical reasons.
SRH has found that establishing birth arrangements for safeguarding before delivery (in line with guidelines) helps to prevent delays in discharge paperwork. To further these improvements, the support available for social workers in Sunderland should continue to be expanded. These measures could reduce admissions for safeguarding by ensuring a smooth transition to foster care.
Targeting drug misuse would also be beneficial, as a large proportion of social admissions relate to maternal substance abuse and NAS, although this will require dedicated support. NAS often requires prolonged admissions, so addressing the root of the problem could reduce the length of stay for these babies.
Furthermore, less serious conditions should continue to be treated on the postnatal ward, such as mild uncomplicated jaundice. As well as following established guidelines and standardised pathways, additional training could be provided for maternity services. This would allow for midwifery-led transitional care that helps to preserve NICU beds for those with greater medical needs while keeping mother and baby together.
Identifying and addressing modifiable risk factors in pregnancy may reduce avoidable term admissions. For example, optimal control of maternal gestational diabetes (GDM) may decrease the likelihood of adverse outcomes in the neonatal period, such as birth injuries and neonatal hypoglycaemia. Placing emphasis on discouraging unnecessary elective C-sections and continuing to administer ANS when required is important. These measures will help to prevent avoidable respiratory admissions from rising further.
Finally, the analyses to-date need to be reviewed. It is important to address inaccuracies of data entry on a provider level, as was established in previous audits.6,7 There ought to be further research that establishes what could be changed on an individual, local and national level. Continuing to highlight trends at SRH and decide plans that improve outcomes is a top priority going forward.
Or read this article in our
Tablet/iPad edition
- Term admissions as a percentage of all admissions to the NICU at SRH decreased between 2014 and 2019; however, there was an increase of 6% in 2020.
- The proportion of term infants admitted to SRH NICU for social reasons continues to be higher than the national average, though it decreased greatly between 2019 and 2020.
- Respiratory disease admissions increased in 2020, contributing to 57.1% of term admissions.
- Antenatal steroids were given to all eligible term mothers who underwent elective C-section before 39 weeks’ gestation in 2020 at SRH, as per national guidelines.
Also published in Infant:
