

Minimising COVID-19 transmission risk during neonatal transport: a practical approach from ANTS
The Acute Neonatal Transfer Service of the East of England (ANTS) has been involved in the transfer of four suspected or confirmed neonatal SARS-CoV-2 (COVID-19) cases. Through this unique clinical experience and related educational activities, we have constructed additional practical recommendations aimed at minimising horizontal SARS-CoV-2 spread during neonatal transfer. Here we present these recommendations for consideration by neonatal transport teams and neonatal units managing neonatal COVID-19 transfers.
Sarah WaltonNeonatal Grid Trainee, ST8
sarah.walton@nhs.net
Sonia Garnell
ANTS Senior Sister
Sarah Rattigan
ANTS Clinical Manager
Sajeev Job
Neonatal Consultant and ANTS Clinical Lead
Susan Broster
Neonatal Consultant and Deputy Medical Director Cambridge University Hospitals NHSFT
The Acute Neonatal Transfer Service, Addenbrooke’s Hospital, Cambridge
Background
There are 14 regional neonatal transfer teams working across the UK. They have the unique role of moving babies between hospitals: babies will be transferred from their local hospitals into specialist or tertiary units if they need ongoing intensive care and transferred back to their local hospital when their clinical condition improves. ANTS is hosted by Cambridge University Hospitals NHS Foundation Trust and comprises a team of senior neonatal doctors and nurses with specific expertise in neonatal transfer, emergency bed service co-ordinators, and ambulance drivers who together are responsible for emergency transfers and repatriation of neonates between the 17 hospitals within the East of England region and beyond.
Evidence from China and the UK shows, respectively, that 9% and 5% of babies born to mothers hospitalised with COVID-19 test positive for SARS-CoV-2,1,2 and there have been cases of neonatal COVID-19 reported in the literature.3 However, there have been no literature reports of managing suspected or confirmed neonatal COVID-19 during transfer of babies between hospitals, making guideline creation in this area uniquely challenging.
The National Neonatal Transport Group (NTG) released guidance on neonatal transfer of suspected or confirmed COVID-19 infection at the start of the UK’s pandemic.4 Since then, ANTS has moved four suspected or confirmed neonatal COVID-19 cases. From this unique clinical experience, in conjunction with an educational programme of simulation and timely debriefs (FIGURE 1), ANTS has developed additional recommendations for consideration by neonatal transfer teams and units involved in neonatal COVID-19 transfers. These are novel, practical recommendations intended to supplement existing COVID-19 equipment advice on, for example, use of personal protective equipment (PPE) or using closed suction systems. Our recommendations, when used in combination with guidance published by the NTG,4 the European Society of Paediatric and Neonatal Intensive Care (ESPNIC),5 and the Royal College of Paediatrics and Child Health (RCPCH),6 aim to minimise risk of horizontal SARS-CoV-2 spread during transfer of suspected or confirmed neonatal COVID-19 cases.
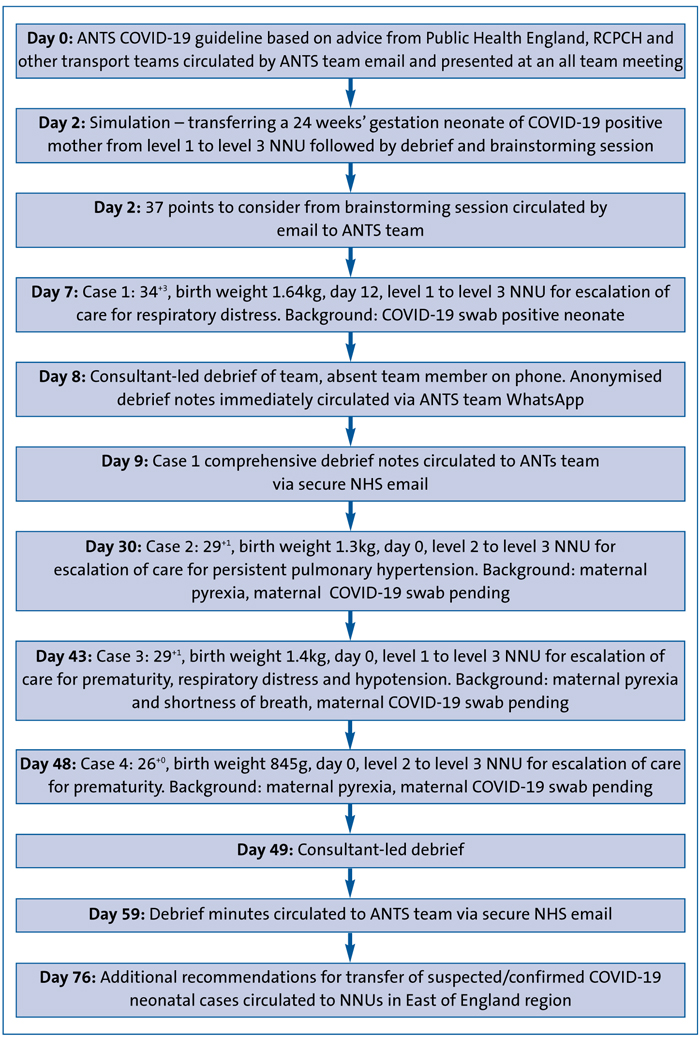
FIGURE 1 A timeline of COVID-19 educational and clinical events within the ANTS team. Key: RCPCH=Royal College of Paediatrics and Child Health, Leicester, NNU= neonatal unit.
Recommendations for neonatal transport teams
The following steps are recommended for neonatal transport teams.
Educate the team
- Simulate transfer of suspected/confirmed COVID-19 cases.
- Hold a timely debrief following simulation and clinical cases.
- Share learning with your team and regional neonatal units.
- Contact your tertiary units to clarify their COVID-19 infection control policies, disseminate these policies to the transport team.
Stock the ambulance
- Each neonatal transport ambulance should be stocked with readymade PPE packs. Include a fit tested mask (trust-specific), visor (or goggles), surgical cap, gown and a disposable pen. Items should be enclosed in a plastic bag. Gloves should not be included in the PPE pack as appropriately sized gloves will need to be selected on donning at the referring unit.
- Ensure each ambulance has a small, portable wipeable white board and pens (see the following section for purpose) and a plastic cover for the transport team’s mobile phone.
On arrival at the referring hospital
- Leave personal effects including bags, lanyards, lunch boxes/water bottles and pen in the ambulance cab.
- Change out of personal uniform and into scrubs if not already done before departing base.
- Place mobile phone within a wipeable case.
- Retrieve a PPE pack for each team member and a white board/pens.
- Consider taking handover, reviewing images and bloods prior to entering isolation (depending on whether this will be possible once inside isolation).
- The driver should remain ‘clean’. The drag bag (containing emergency equipment) and back pack (containing drug bag, controlled drugs and routine equipment) stays with the driver outside the isolation room.
- Non-essential equipment from the drawers of the transport incubator should be decanted into plastic bags to stay with the driver outside the isolation room.
During transfer
- To ensure the driver remains clean and appropriately distanced, the clinical team, nurses and doctors should operate the ambulance tail lift (following prior training). The drag bag, back pack, and the plastic bags with unused equipment should remain clean with the driver in the ambulance cab.
- Consider the risks and benefits of using the ambulance air-conditioning during transfer.
- Call the receiving unit ahead of your arrival and ask for an escort to be arranged. The transport team should call ahead to the receiving unit to agree a safe point of entry to the hospital and to give an estimated arrival time to help timely planning of the escort.
Following completion of transfer
- Upon return to base, the team should shower and change back into uniform. The shower gel, towels, and fresh scrubs should be stored in a cupboard outside the transport office.
Recommendations for neonatal units
The following steps are recommended for neonatal units:
Carefully consider isolation room features
- The isolation room should be large enough to allow the transport incubator to be pulled alongside the unit’s incubator and for the door to completely close behind it.
- Avoid placing COVID-19 cases in isolation rooms next to the main entrance or exit to the neonatal unit. If unavoidable, consider temporarily changing the neonatal unit entrance/exit to minimise visitors passing by the isolation room.
- Provide donning and doffing facilities outside and within the isolation room, respectively. Stick-up poster guidance on these processes outside and inside the isolation room.
- Consider a buddy system for donning and doffing.
- You will need facilities for doffing masks outside the isolation room and a hand hygiene station within and outside the room.
Minimise isolation room door opening
- The transport team should have a small, portable whiteboard and pens to write requests for equipment and drugs on. This can be shown to the team outside the isolation room via a window or windowed door and avoids unnecessary door opening (FIGURE 2).
- Consider having a pre-prepared ‘COVID-19 trolley’ ready at all times on your unit. This should be stocked with common neonatal nursing and medical equipment. Consider including blood gas, cannulation, naso/orogastric tubes, nappy change equipment, a sharps bin, IV/oral syringes, flushes, gauze, dressings, tape, alcohol wipes, trays, spare pens and continuation sheets. This can be wheeled into the isolation room for emergency COVID-19 admissions.
- Based on information from Public Health England (PHE) on clearance of infectious particles after an aerosol generating procedure (AGP),7 door opening should be avoided for at least 20 minutes following an AGP. PHE continues to review its guidance around AGPs, however, in this uncertain environment we continue to use 20 minutes as a safe timeframe.
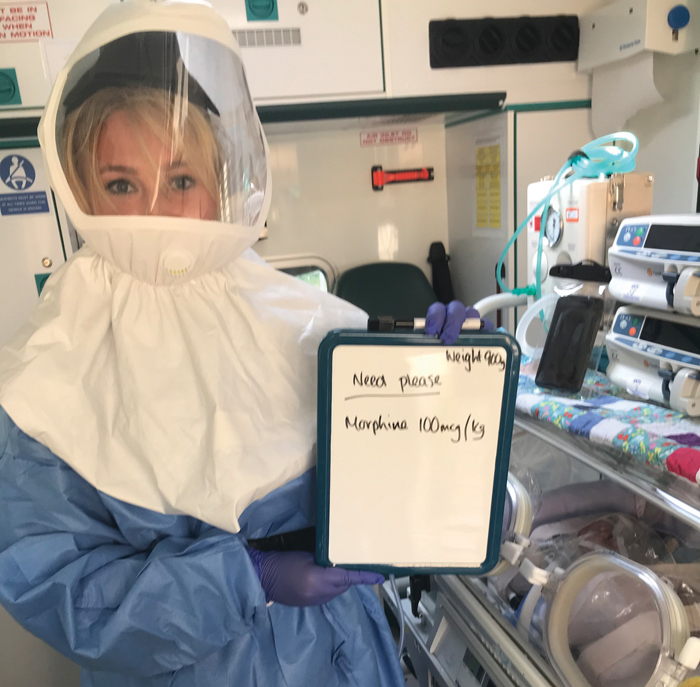
FIGURE 2 Transport team member with full PPE and a small, portable whiteboard.
Managing paperwork
- Local paperwork should not leave the isolation room for photocopying.
- The transport team can take their paperwork with them within the incubator tray. The paperwork will stay with the baby at the receiving unit. Photographs of the paperwork required for the transport team’s records should be taken on a dedicated transport team secure mobile phone and printed-off back at the transport team’s base.
Planning safe movement of the transport team through the hospital
- Let the transport team know if you want them to doff and re-don prior to moving through the hospital with the neonate. You are likely to need to provide replace-ment PPE for them in this instance.
- Ask your porters/security to escort the transport team with the neonate to or from the neonatal unit (depending on whether you are the receiving or referring unit). ANTS have found this invaluable for clearing crowds and guiding the team on approved COVID-19 routes/lifts.
Summary
Our recommendations are based on our limited current clinical experience and are not an exhaustive list. They are likely to be adapted with increasing clinical experience and evidence, and should be used in conjunction with existing local, national and international guidance on managing and transferring suspected or confirmed neonatal COVID-19 cases.
The expedient educational approach illustrated seems anecdotally to have improved ANTS medical and nursing team confidence in managing suspected or confirmed neonatal COVID-19 transfers and research into this is ongoing.
Or read this article in our
Tablet/iPad edition
- Neonatal transport teams and units may be involved in moving suspected or confirmed neonatal COVID-19 cases.
- Guidance on managing such transfers has already been published by the NTG and ESPNIC. ANTS has compiled additional practical recommendations from its experiences.
- Together these recommendations will minimise horizontal SARS-CoV-2 spread during neonatal transfer.
Also published in Infant:
