

A structured approach to facilitate the reintroduction of parents in transport during the SARS-CoV-2 pandemic
In response to the COVID-19 pandemic, transport teams ceased taking parents with them on neonatal transfers except in exceptional circumstances. With the easing of lockdown, the Acute Neonatal Transfer Service of the East of England (ANTS) recognises how important it is for parents to be involved in their baby’s journey and has developed a set of recommendations to mitigate the risk of horizontal transmission of SARS-CoV-2 in transport.
Sarah Rattigan
RGN, RSCN, 405, 998, DPSN, BA(Hons),
PGDip, MSc, MIHM
Clinical Service Manager
sarah.rattigan@nhs.net
Rachel Perry
RGN, RSCN, 405, 998
Senior Sister
rachel.perry@addenbrookes.nhs.uk
Sajeev Job
MBBS, DCH, MRCPCH, MRCPS, FRCPCH
Consultant Neonatologist and
ANTS Clinical Lead
Acute Neonatal Transfer service (ANTS) hosted by Cambridge University Hospitals NHS Trust
The Acute Neonatal Transfer Service, ANTS, hosted by Cambridge University Hospitals Foundation Trust serves as the neonatal transport team covering 17 hospitals in the East of England. The ANTS team has the responsibility to transfer any baby born to a mother who has had her antenatal care booked in the East of England. These transfers include both emergencies and stable repatriations and often involve travelling outside the East of England to ensure that the critically unwell neonate remains within their agreed neonatal care pathway.
The ANTS team comprises senior nurses and doctors with specific training in transfer medicine. St John Ambulance provides dedicated vehicles, and the ambulances are driven by front line drivers who are experts at a driving style suitable for sick babies, including driving with blue lights. Within the team are the emergency bed service (EBS) coordinators who provide a bed bureau service for in utero as well as ex utero cot location.
In 2009, the Toolkit for Neonatal Services1 recommended where possible that parents should have the opportunity to accompany their baby during transfer. Bliss’ Transfer of Premature and Sick Babies2 highlights the importance of ensuring that all parents are involved as much as possible if their baby needs to be transferred to try to minimise any stress and anxiety they feel over the transfer. Having been one of the first teams to implement parents travelling, the accepted practice within ANTS is to offer at least one parent the opportunity to travel with their baby. In 2019 the practice changed following careful review to allow both parents the opportunity to travel. This was subject to careful assessment to ensure that the parents and staff were all safe, in particular a mother who had recently delivered.
Parents in neonatal transfer during the SARS-CoV-2 pandemic
At the start of the SARS-CoV-2 pandemic there was a lot of uncertainty about transmission rates and risks of horizontal and vertical transmission of the virus. In line with national advice and guidance,3,4 the practice of parents accompanying their baby in transport ceased due to the potential risk to team members from the unknown impact of infection and also in anticipation of staffing challenges/availability due to sickness and self isolation. At the same time, visiting in neonatal units was also severely restricted or terminated.5
The early review of COVID-19 related literature and publications from case reports demonstrated that SARS-CoV-2 is transmitted through droplet or contact transmission. Droplet transmission is thought to include speaking, breathing, sneezing and coughing,6 and SARS-CoV-2 has been shown to be more stable (up to 72 hours) on contact surfaces made of plastic and stainless steel.7 The interior of the transfer vehicle and transport incubator are therefore potential sources of transmission, being largely made of these materials.
Reintroduction of parents in neonatal transfers with the ANTS team
At the start of the UK pandemic, the Neonatal Transport Group released guidance on neonatal transfer of suspected or confirmed COVID-19 infection and since then ANTS developed additional recommendations for consideration by neonatal transfer teams.8,9 With the easing of lockdown, the ANTS team has reconsidered parents accompanying their babies in transfers. We recognise how important it is for parents to be involved with their baby’s journey as much as possible and the consensus of the team was to recommence the parents in transfer service where it was safe to do so. However, this requires individualised assessment at the time of transfer and is multifactorial based on the health and needs of the parents, staff and baby.
Knowledge about localised areas of intervention or lockdown is used when assessing the situation. This involves careful risk assessment, measuring of core body temperature by taking a tympanic temperature, a new guideline for parents in transfer and individualised situational decision making.
The first priority and duty of care during the pandemic risk period has had to be the safety of the team, as risk of COVID-19 transmission has the potential to affect the service and staffing levels. The ANTS team undertaking the transfer, in consultation with the wider team, must make a decision in each case as to whether it is appropriate and safe to transport one parent with the baby in the ambulance.
Recommendations for neonatal transfer teams
The team developed the following four sets of recommendations to mitigate the risk of horizontal transmission in transport:
Recommendation 1: assessing risk
- Use of a standardised risk assessment tool for transport (FIGURE 1).
- Recording the tympanic temperature of the parent.
- Criteria evidencing low risk of transmission.
- Open questions about contacts.
- Risk assessment for all staff.
- Daily discussion of local areas of concern within the region, as identified by Public Health England.
- Check with the referring unit if they have any concerns, and the maternity unit for any results from the mother.
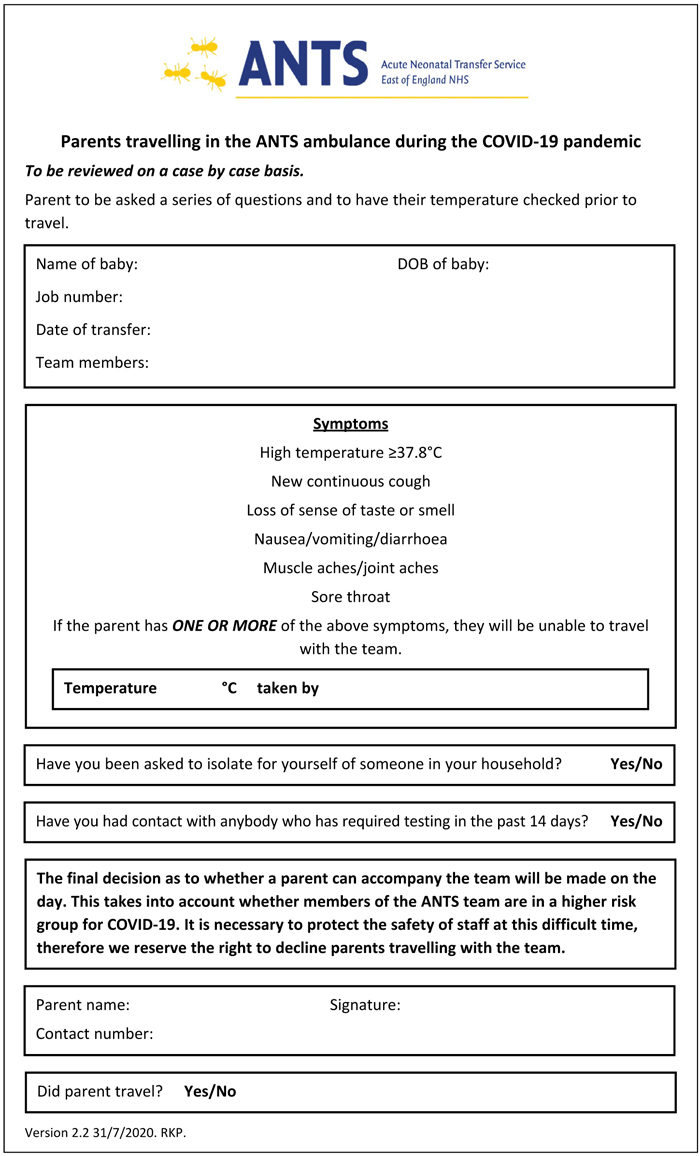
FIGURE 1 A standardised risk assessment tool for transport.
Recommendation 2: infection prevention measures
- Fluid resistant surgical masks for all staff and parents. The parents’ own masks should not be used due to unknown efficacy of transmission prevention.
- Eye protection available for staff (masks or visors) – optional.
- Hand sanitiser available and used on entering/exiting the vehicle.
- Wiping down of all surfaces between transfers.
- Incubators double cleaned between transfers.
- Incubators deep cleaned for known contaminants.
- Incubators treated with UV light monthly.
Recommendation 3: equipment
- Source tympanic thermometers suitable for adult patients (one per incubator, FIGURE 2).
- Arrange stock of disposables for the thermometers.
- Competency assessment of all staff in the use of a new piece of equipment.
- Corporate approval for use of a new clinical intervention procedure.

FIGURE 2 Taking the temperature of a parent.
Recommendation 4: communication
- Communicate within the team, network and neonatal units about expectations and restrictions, enforcing that it will be a decision made on an individual basis according to many factors.
- Develop a guideline to support practice.
- Make an agreement with the parent that they must inform the ANTS team of any infection concerns within 14 days of transfer.
- Obtain occupational health advice about impact on the team if a parent is subsequently found to be COVID-19 positive.
- Seek agreement from the infection control advisors about mitigating measures and use of personal protective equipment (PPE).
- Inform parents of the need to travel back-wards and wearing a mask (FIGURE 3).
- Understand the receiving unit’s visiting and residents’ policy so that the parents know what to expect – this may influence whether they travel with the team or independently.

FIGURE 3 A parent in the ambulance with transport team members.
Further considerations
The ANTS team recognises the importance of reintroducing the practice of taking parents on transfers. There needs to be careful consideration of how this can be implemented in a safe and timely manner, this includes acknowledging the presence of a variation in practice between neonatal units and trusts with regard to self-isolation and PPE policies. It would be best to have robust processes in place to ensure there is no unit or parental perception of undue bias or preferential treatment by staff.
With the easing of lockdown and at the time of writing, 20 parents have travelled with the team. Having commenced taking parents on transfers, the staff report that it has been a positive experience. Anyone from the team can perform the parent’s risk assessment and temperature readings and in many cases the St John Ambulance drivers take this on to allow for the clinical team to focus on the baby’s care.
Or read this article in our
Tablet/iPad edition
- Where possible, parents should have the opportunity to accompany their baby during transfer.
- The ANTS team has recommenced the parents in transfer service on an individ-ualised basis where it is safe to do so.
- A series of recommendations to guide careful assessment of each case has been developed.
- These recommendations will minimise horizontal spread of SARS-CoV-2 during neonatal transfer.
Also published in Infant:
