

Less invasive surfactant administration (LISA): experience from a local neonatal unit
This article reviews the background of the less invasive surfactant administration (LISA) technique, the methods used in our local neonatal unit, and a comparison with practice in other units. It provides a brief review of the evidence for the use of routine sedation in LISA and the use of pain scores in the neonatal unit. We demonstrate how we have successfully introduced the LISA technique into our local neonatal unit, thereby reducing the need for neonatal transfer to a neonatal intensive care unit.
Cara L. Owens
Paediatric Specialty Doctor
cara.owens@aapct.scot.nhs.uk
Raju Sunderesan
Paediatric Consultant
raju.sundersan@aapct.scot.nhs.uk
Ayrshire Maternity Unit, University Hospital Crosshouse, Kilmarnock
Surfactant administration is a very common and important procedure in the neonatal unit.1 It provides timely respiratory assistance to the neonate, without which serious complications might arise, some fatal. The majority of infants born at less than 32 weeks’ gestation develop respiratory distress syndrome (RDS). Historically the strategy to manage RDS has been to intubate and administer surfactant. However, it is well known that mechanical ventilation is one of the main risk factors of bronchopulmonary dysplasia (BPD) and reducing mechanical ventilation is one of the ways to limit the risk of BPD. Therefore, there is an additional imperative to make the delivery of surfactant as non-intrusive as possible, preferably without recourse to anaesthetic.
Over the years, clinicians have strived to develop techniques to administer surfactant without endotracheal intubation and this has become possible with the advent of LISA techniques.2-5 Although LISA techniques have become popular, practice is varied around the world in regards to the timing of procedure and the use of pre-medication. Therefore, the purpose of this study is to review our unit’s practice over the two years since we intro-duced the LISA technique and compare our practice to other centres.
We are a local neonatal unit in Kilmarnock, Scotland, and began using the LISA technique in July 2018. We wanted to build upon the reasons why LISA had been implemented; to analyse the specific techniques used and the outcomes for the infants who received this treatment. We retrospectively reviewed all neonates who had undergone surfactant administration via the LISA technique over a two-year period (July 2018 to July 2020). We also used an online survey tool to collect information on the practice of LISA in other neonatal units around the world.
Historical perspective
Surfactant is not always straightforward to deliver. By the mid-2000s, the INSURE (INtubation-SURfactant-Extubation) strategy had become common practice. This involved early administration of surfactant, followed by brief ventilation and extubation to continuous positive airway pressure (CPAP) therapy. It resulted in a lower risk of subsequent mechanical ventilation and a reduced oxygen need in the following 28 days.6 However, it soon became apparent that even a short period of mechanical ventilation increased the risk of BPD.7 To minimise this risk, methods of delivering surfactant without the need for intubation and sedation began to develop; this became known as minimally invasive surfactant therapy (MIST).
Danish neonatologist Henrik Verder was the first to use a gastric tube to instil surfactant in a spontaneously breathing infant in 1992 and this was rekindled in 2003 by Angela Kribs in Cologne. This method is, therefore, called the Cologne method and involves the insertion of a flexible tube (eg a nasogastric feeding tube) with the use of Magill’s forceps. German neonatologists were among the first to successfully trial ‘avoidance of mechanical ventilation and non-intubated surfactant administration’8,9 and other European countries quickly followed suit.
In 2011, Prof Peter Dargaville in Hobart, Australia, used a stiffer vascular catheter to administer surfactant.10 This is popularly known as the ‘Hobart method’. Presently, purpose built semi-rigid surfactant instillation catheters are available (LISAcath, Chiesi; Surfcath, Vygon) and this method has become popular.
A meta-analysis of LISA procedures in 2017 by Aldana-Aguirre et al11 showed an overall reduction in death and BPD at 36 weeks. Similarly, Wu et al’s meta-analysis showed that LISA reduced the need for mechanical ventilation by half and reduced BPD by 30%.12 As per the European consensus in 2019, LISA is gaining acceptance as the preferred mode of surfactant administration for spontaneously breathing infants on non-invasive respiratory support. The recommended dose of surfactant is 100-200mg/kg, with a repeat dose of 100mg/kg if required, to a maximum dose of 400mg/kg per course.13,14
Use of sedation
Assessing levels of discomfort in neonates is notoriously difficult and often subjective although there are various scoring tools in use. These involve a combination of observation of the baby’s facial expressions, objective measurements (including vital signs) and the behaviour of the infant. To date, there is no universal approach to neonatal pain assessment. Validated pain scales include:
- N-PASS: neonatal pain, agitation, and sedation scale
- COMFORT-neo: alertness, calmness/agitation, respirations, physical movement, heart rate, blood pressure, muscle tone and facial tension
- CRIES: cry, requirement for more oxygen, increased vital signs, expression, and sleeplessness.
Although pre-medication use prior to endotracheal intubation is considered a standard of care, there is debate about the use of sedation during LISA with practice varying between different units. Most centres prefer non-pharmacological methods of comforting the infant with positioning, swaddling and breast milk.
A variety of medications (eg fentanyl, ketamine and propofol) have been studied and, while they help in comforting the infant, they have the potential for suppressing breathing, which may necessitate intubation with acute and long-term side effects (eg fentanyl can cause chest wall rigidity and respiratory depression).15
There have been very few randomised controlled trials (RCTs) on the use of sedation during LISA. There has been recent interest in propofol due to its rapid onset and short action.16 It has been shown to be a suitable sedative for non-emergency neonatal intubation.17 In an RCT, Dekker et al studied the use of propofol during MIST in infants between 26 and 36 weeks’ gestation. The outcome demonstrated that, although low-dose sedation increased comfort (using standardised COMFORT-neo scores), it increased the need for ongoing non-invasive ventilation.15 Similarly, Tauzin et al showed an increase in the frequency of mechanical ventilation within the first 72 hours of life in infants who received propofol compared with those that did not receive pre-medication.18
Presently there is no consensus throughout the neonatal community in regards to the use of sedation during LISA. A UK-wide survey found that 49% of units did not use sedation or pre-medication. Of those that did, the most common was fentanyl (31.1%); 20% use sucrose.19 A survey of European neonatal departments in 2017 showed that 52% of units used sedation as routine.20
Our experience
Our unit is a level 2 local neonatal unit and we began using the LISA technique in July 2018. We recorded our practice for 24 months (17 July 2018 to 16 July 2020). To allow consistent analysis of the technique, we created a data collection form for infants treated with LISA. Additionally, we examined our patient records using Badger software to identify all patients who had received surfactant during their stay. Any infant on non-invasive respiratory support with a persistent oxygen requirement of more than 30% was deemed eligible for LISA.
When we first introduced LISA in our unit it was a consultant-only procedure, however, as we gained experience our registrars and advanced neonatal nurse practitioners (ANNPs) began to perform the procedure. At the outset, the LISAcath from Chiesi was the only catheter available. More recently, we also have access to the Surfcath from Vygon. Catheter insertion was specified at 2cm at vocal cords for preterm infants and 3cm for near-term infants (FIGURE 1).

FIGURE 1 Insertion of Surfcath. This catheter has a characteristic 2cm angled black tip.
Our pathway for the LISA technique
We created a pathway for the LISA technique (FIGURE 2). The infant would remain on non-invasive ventilation support (CPAP/nasal high-flow) during the procedure. We found that there were fewer incidents of oxygen desaturations when infants remained on high flow during placement of the LISA catheter, however, due to its bulkiness, CPAP needed to be disconnected while placing the catheter. With the infant in a supine position and head in the midline, surfactant was administered in small aliquots over a five-minute period.
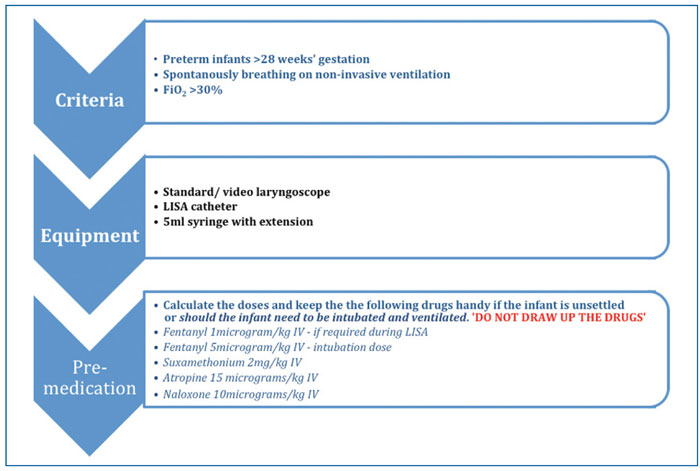
FIGURE 2 The LISA pathway.
Our journey so far
Twenty-five infants received surfactant using the LISA technique during the two-year period of data collection. The majority of the infants were less than 34 weeks’ gestation (FIGURE 3) with an average weight of 1.58kg. All infants required non-invasive respiratory support prior to the LISA procedure, with 23 infants receiving nasal CPAP and two receiving nasal cannula high flow oxygen. The average oxygen requirement pre-procedure was 43.8% (range 28-79%).
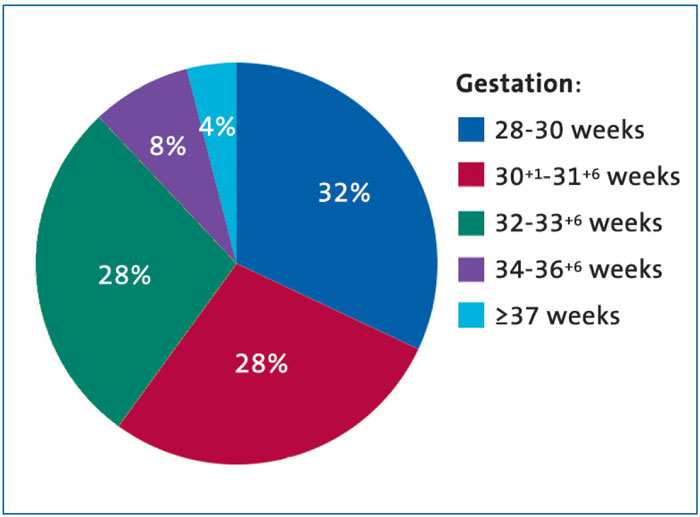
FIGURE 3 The gestational age distribution of the infants in the study.
The mean age in hours when LISA was carried out was just over nine hours (range = 0.58-45 hours). Fifteen infants received LISA using video assist, while a standard laryngoscope was the preferred choice for the remainder. The LISA procedure was carried out by a consultant or specialty doctor in 12 cases, trainees (ST3-8) in 11 cases and by an ANNP in two cases. In all cases, the procedure was completed within two attempts; there were no failed procedures.
All the procedures were performed without routine sedation and in the majority, the infants were comfortable during the procedure with stable observations. However, in two cases the infants were judged to be distressed and received fentanyl. Seven infants recorded oxygen desaturations and a further five infants had oxygen desaturation with bradycardia, which resolved following an increase in oxygen and transient interruption in surfactant delivery. The procedure was completed once the observations normalised. The average oxygen requirement following the procedure decreased with time as is shown in FIGURE 4. At four hours post-procedure, the average oxygen requirement was 27.2% (range = 21-75%).
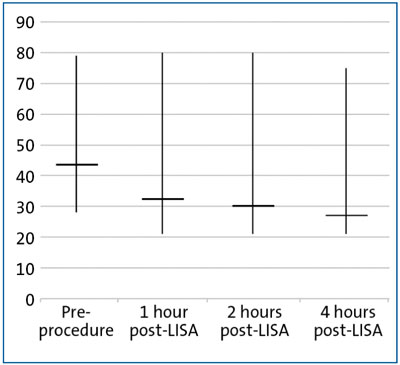
FIGURE 4 Average oxygen requirements (%) before and after LISA. Averages shown with ranges.
LISA was successful in most cases, however, five infants required mechanical ventilation within 48 hours post-LISA. The average time interval between LISA and intubation was 12.7 hours (range = 0.5-38 hours). One infant required a further dose of surfactant via LISA.
A review of international practice
We also gathered information on LISA practices from different neonatal units around the world using an online survey. The recipients were identified from our own colleague contacts. Specifically, we looked at the use of pre-medication and any subsequent adverse effects, including a need for mechanical ventilation. We sent out questionnaires to 42 units, and received 18 responses (43% response rate) from nine different countries (FIGURE 5).
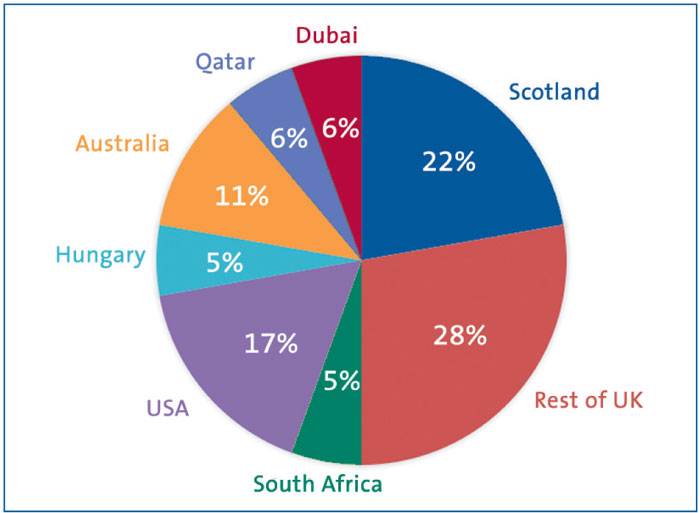
FIGURE 5 The response to the LISA questionnaire, by country.
The units comprised level 2 and level 3 neonatal care. Twelve of the units reported using LISA, including one that used a modified technique with a size 2 endo-tracheal tube while the infant remains on CPAP. One unit used MIST with a feeding tube to deliver surfactant. Five units do not use LISA.
Most units used 28-34 weeks’ gestation as an eligibility criterion, along with increasing oxygen requirement, although three units had no specific cut off. For six units, LISA is a consultant-only procedure, with the remaining units allowing trainees and ANNPs to carry out the procedure.
Most units reported having performed at least 15 procedures with a unit in Hungary reporting more than 100 procedures. Only four units reported the use of routine sedation; interestingly, the unit in South Africa uses midazolam while the team in Hungary uses nalbuphine. None of the units reported any major adverse effects.
Discussion
We have accumulated a convincing case for the use of LISA over the two years that it has been used in our department. Of the 25 patients given LISA, only five required subsequent mechanical ventilation. By reducing the need for invasive ventilation, the LISA procedure diminishes the risk of preterm lung injury, with a consequent reduction in time spent in intensive care and in the neonatal unit overall.
Although the use of sedation has been a point of contention, in our experience most infants coped well without sedation. Fentanyl was required in only two cases (both at beyond 36 weeks’ gestation). Anecdotally, larger near-term infants can appear more distressed during the procedure and are therefore more likely to need sedation. Two thirds of the responding units were not routinely giving sedation and these findings were reassuring as they mirror our practice.
Assessing pain and discomfort can be difficult in neonates. We are considering formally implementing the pain score (N-PASS score) system to measure comfort during the procedure.
Use of a video laryngoscope has been invaluable while performing the LISA technique and intubation. In our experience, the video laryngoscope allows accurate placement of the catheter tip due to much improved visualisation of the vocal cords. This ensures optimum delivery of the surfactant, facilitating equal distribution to both lungs. Additionally, it gives training-grade doctors and ANNPs the confidence to carry out the procedure by permitting a view visible to the supervising consultant.
The data from other units allowed us to compare our practice. Level 3 units reported the highest number of LISA procedures and the skill level of the administrator replicated our own practice with LISA. As units become more familiar with the LISA technique, it should be possible for junior staff to acquire this skill.
We have demonstrated that we have safely and effectively introduced the LISA technique into our level 2 local neonatal unit. This is important for the future planning of neonatal services and reduces the need for neonatal transfer to a level 3 neonatal intensive care unit.
Conclusion
The LISA technique offers a viable alternative administration of surfactant that can save many infants from the need for intubation and mechanical ventilation. The introduction of LISA to our unit has contributed to a change in practice towards fewer preterm infants requiring mechanical ventilation.
Our data represent a small subset and the selection of survey recipients is based on our contacts. Further data collation is needed to clarify remaining uncertainties regarding the use of pre-medication. A suggested further area of interest would concern how units routinely assess neonatal pain.
There is renewed interest in exploring novel methods of surfactant administration. We need to strive for the safe administration of surfactant and by collectively examining our practices we can move forward and improve the care we offer to our infants.
Acknowledgement
The authors wish to thank Dr Frances Butterworth (Paediatric Specialist Trainee) for her help in the initial data collection, the respondents to the survey, and all those involved in the clinical care at Ayrshire Maternity Unit for aiding the data collection.
Or read this article in our
Tablet/iPad edition
- The LISA technique has good success rates for administering surfactant to neonates without the need for mechanical ventilation.
- We analysed our practice over two years since introduction, specifically looking at those infants needing sedation.
- In general, routine sedation is not needed in preterm infants.
- LISA can be carried out safely and effectively in smaller local neonatal units.
Also published in Infant:
