

Intra-thoracic lesions mimicking congenital diaphragmatic hernia
Congenital diaphragmatic hernia (CDH) is a complex condition characterised by a defect in the diaphragm through which the abdominal contents can herniate leading to compromise of fetal lung and cardiovascular development. In this article, we present three cases of suspected CDH in newborn infants in which further evaluation excluded CDH and confirmed alternate diagnoses.
Annie Colthorpe1,2
Neonatal Grid Trainee
Anthony Emmerson1,2
Consultant Neonatologist
Susan Kamupira1,2
Consultant Neonatologist
Nick Lansdale1,3
Consultant Paediatric Surgeon
Kristin Tanney1,2
Consultant Neonatologist
1The Manchester Centre for Neonatal Surgery, Manchester University NHS
Foundation Trust
2Newborn Intensive Care Unit, Saint Mary’s Hospital, Manchester
3Paediatric and Neonatal Surgery, Royal Manchester Children’s Hospital
CDH is a complex condition requiring careful medical and surgical management. It is characterised by a defect in the diaphragm through which the abdominal contents such as stomach, intestines, liver and other visceral organs can herniate, leading to compromise of fetal lung and cardiovascular development. Diaphragmatic defects most commonly occur postero-laterally (Bochdalek-type CDH) and most frequently on the left side of the chest. A less common type of CDH is the Morgagni defect, which occurs anteriorly. Central defects are rarer still.1,2 Diagnosis of CDH is made either antenatally during routine ultrasound scans or postnatally, most often by plain chest radiograph following signs of respiratory distress in an infant.
We present three cases of suspected CDH in newborn infants transferred to a regional surgical neonatal intensive care unit (NICU). However, in these cases further evaluation and imaging excluded CDH and confirmed alternate diagnoses, highlighting the potential diagnostic uncertainty of plain radiography.
Infant A
Infant A was born at 36 weeks’ gestation with antenatally-diagnosed CDH and complex congenital cardiac defects (complete atrioventricular septal defect, unbalanced ventricles and double outlet right ventricle). She was intubated and ventilated immediately after birth. An initial chest X-ray was atypical for a Bochdalek-type CDH but a central Morgagni defect was suspected (FIGURE 1A). A barium contrast study confirmed congenital hiatus hernia and malpositioned duodenum (FIGURE 1B). A nasojejunal tube was passed to permit safe feeding, but surgical intervention was not undertaken due to the complex cardiac pathology. The infant was supported with palliative care and passed away at three months of age.

FIGURE 1a A chest X-ray post-nasojejunal tube insertion suggesting central Morgagni defect.

FIGURE 1b Barium contrast showing hiatus hernia.
Infant B
Infant B was born at 35 weeks’ gestation in good condition. He later developed respiratory distress requiring continuous positive airway pressure (CPAP) therapy. An initial chest X-ray suggested CDH and the infant was transferred to the surgical NICU (FIGURE 2A). A thoracic computed tomography (CT) scan with contrast was performed owing to the atypical chest X-ray and this demonstrated pulmonary interstitial emphysema secondary to surfactant-deficient lung disease, with a large locule of air posterior to the heart (FIGURE 2B). Respiratory support was gradually weaned. Repeat plain radiography demonstrated improved appearances and the infant was discharged home at 12 days of age.
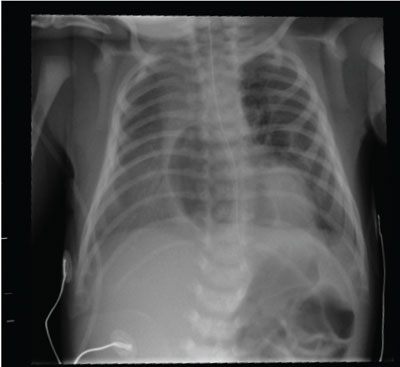
FIGURE 2a Chest x-ray with area of lucency around the mediastinum suggesting CDH.
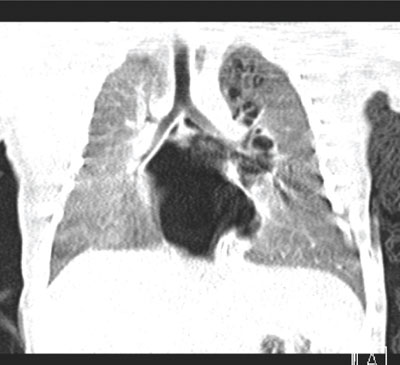
FIGURE 2b A thoracic CT scan showing pulmonary interstitial emphysema, especially visible in the left upper lobe.
Infant C
Infant C was born at 32+0 weeks’ gestation and required early CPAP support. With increasing oxygen requirements, she received surfactant (Curosurf) via the less invasive surfactant administration (LISA) technique on day 2 of life. She improved clinically and was gradually weaned off CPAP while feeds were increased. Bilious gastric aspirates were noted on day 4 and a chest X-ray was suspicious of CDH, with a lucency across the diaphragm (FIGURE 3A). She was further investigated with a thoracic CT scan and found to have posterior pneumomediastinum (FIGURE 3B). This resolved without further intervention.
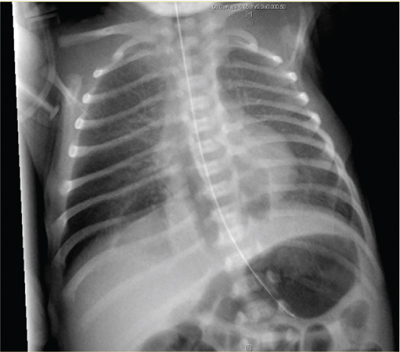
FIGURE 3a A chest X-ray showing an area of lucency across the diaphragm.
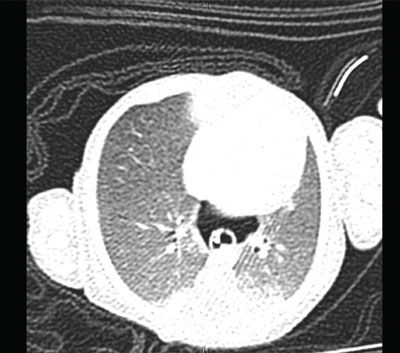
FIGURE 3b A thoracic CT scan showing posterior pneumomediastinum.
Conclusion
These cases illustrate that antenatal findings and initial postnatal chest X-rays can be misleading when considering the diagnosis of CDH. A common feature here was the central location of the lucent area (gas) around the diaphragm: this led to further imaging in each case and allowed the correct diagnoses to be made.
Learning points
- Consider additional causes of central lucency on plain chest radiographs, such as mediastinal air, emphysema and bullae as well as herniation in the case of CDH and hiatus hernia.
- Always insert a nasogastric tube (NGT) prior to performing a chest X-ray for respiratory distress. In Infant A, deviation of the NGT towards the right-hand side below the diaphragm suggested a midline diaphragmatic defect.
Parental consent
The authors would like to thank the parents of the three infants described, who have given their consent for their babies’ images to be shown.
Or read this article in our
Tablet/iPad edition
- Chest X-rays may be misleading when considering a diagnosis of CDH.
- If there is diagnostic uncertainty and/or when considering surgical intervention, additional imaging can be beneficial.
Also published in Infant:
