

Is pressure support ventilation superior or more physiological as a weaning mode when compared to other conventional modes in the NICU?
Conventionally synchronised intermittent mandatory ventilation (SIMV) has been the most commonly used mode in neonatal ventilation, but other hybrid modes combining volume guarantee (VG) have gained popularity. Pressure support ventilation (PSV) has been shown to be physiologically superior for oxygen cost of breathing in adults and has also been used in paediatric populations. Its use in neonatal ventilation, though not new, is still infrequent. The physiological rationale behind its use has prompted many neonatal units to use it as a weaning mode. This article aims to review how PSV, used in isolation or with VG, compares to SIMV or assist-control when used for weaning ventilation in the neonatal population.
Amitava SurMBBS, DCH, DNB, FRCPCH
Consultant Neonatologist, Research, Audit and QI Lead, Lancashire Women and Newborn Centre, East Lancashire Hospital NHS Trust, and Honorary Senior Lecturer, Edgehill University, Ormskirk, Lancashire
The strategies of ventilation in the neonatal population have undergone a change in the last two decades with more emphasis on early non-invasive support such as CPAP, even in the extremes of gestation to reduce incidence of chronic lung disease (CLD). Invasive ventilation has also been revolutionised by the emergence of accurate flow sensors that can sense flow and pressure changes in the airway. Even when invasive ventilation is required, PTV modes, such as ACV or SIMV, are generally preferred over IMV to support spontaneous breathing.
TABLE 1 Ventilation-related abbreviations used in this article.
PTV is hypothesised to minimise patient ventilator synchrony. Earlier studies in preterm infants have reported improved gas exchange, ventilation and more consistent tidal volume delivery with synchronised ventilation compared to conventional ventilation.1-5 Although these modalities appear more physiological, very few studies have shown consistent benefits of one mode over the other. In a Cochrane meta-analysis on synchronised mechanical ventilation for newborn infants, Greenough et al2 concluded that, compared to IMV, triggered modes are associated with a shorter duration of ventilation (mean difference: −38.30 hours; 95% CI: −53.90 to −22.69). When comparing ACV with SIMV, the authors reported that duration of weaning was reduced in favour of ACV when compared to SIMV but did not reach statistical significance. In this review they also concluded that there were insufficient randomised trials comparing the other modes of ventilation for them to be recommended.
Pressure support ventilation
PSV is in principle a patient triggered flow-cycled and time-limited mode of ventilation where the ventilator provides a flow to support the triggered inspiration. There is a sharp increase in inspiratory flow, which peaks and then decelerates rapidly. At the termination point, inspiratory flow ceases and the breath cycles directly into expiration (FIGURE 1). The specific termination point is usually a function of the delivered tidal volume and is almost always when flow has decelerated to 5-15% of peak flow. Inspiratory flow delivery during PSV is variable and is proportional to the patient’s effort and pulmonary mechanics. The peak pressure is usually set by the clinician but when PSV is combined with volume targeting (PSV+VG), it varies to deliver the set tidal volume and changes according to compliance of the lung (FIGURE 2). PSV is thus a spontaneous ventilation mode in which the patient controls the rate and the inspiratory time. SIMV is used to provide a backup or safety net in the event of patient apnoea or decreased effort; however, PSV may be, and is often, used alone. These physiological benefits might reduce work of breathing and hence be potentially an attractive mode for weaning in the preterm population. In this review we seek to analyse the evidence behind this hypothesis.
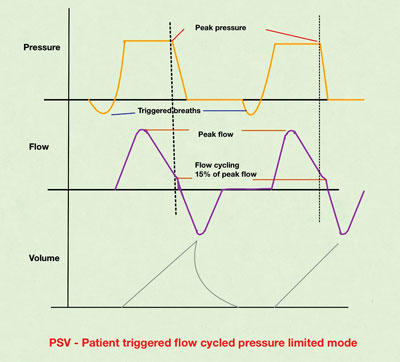
FIGURE 1 PSV mode scalar graphics.
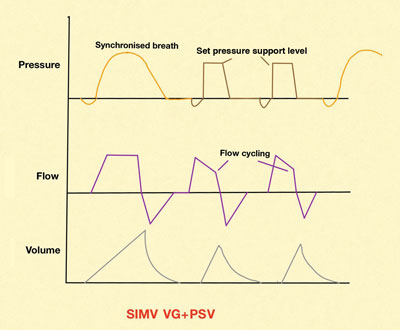
FIGURE 2 PSV combined with SIMV.
Literature search
A literature search was performed of the primary sources Pubmed, MEDLINE and EMBASE using keywords (pressure support ventilation) OR (PSV). Additional filters used were age (up to one month) and type of study (clinical trials and randomised clinical trials, RCTs). Thirty-four unique articles were identified and six are included in this review. Only the RCTs comparing PSV or PSV+VG to SIMV or ACV were selected for inclusion. Reviews and observational studies were excluded. TABLE 2 summarises the six studies with key conclusions.
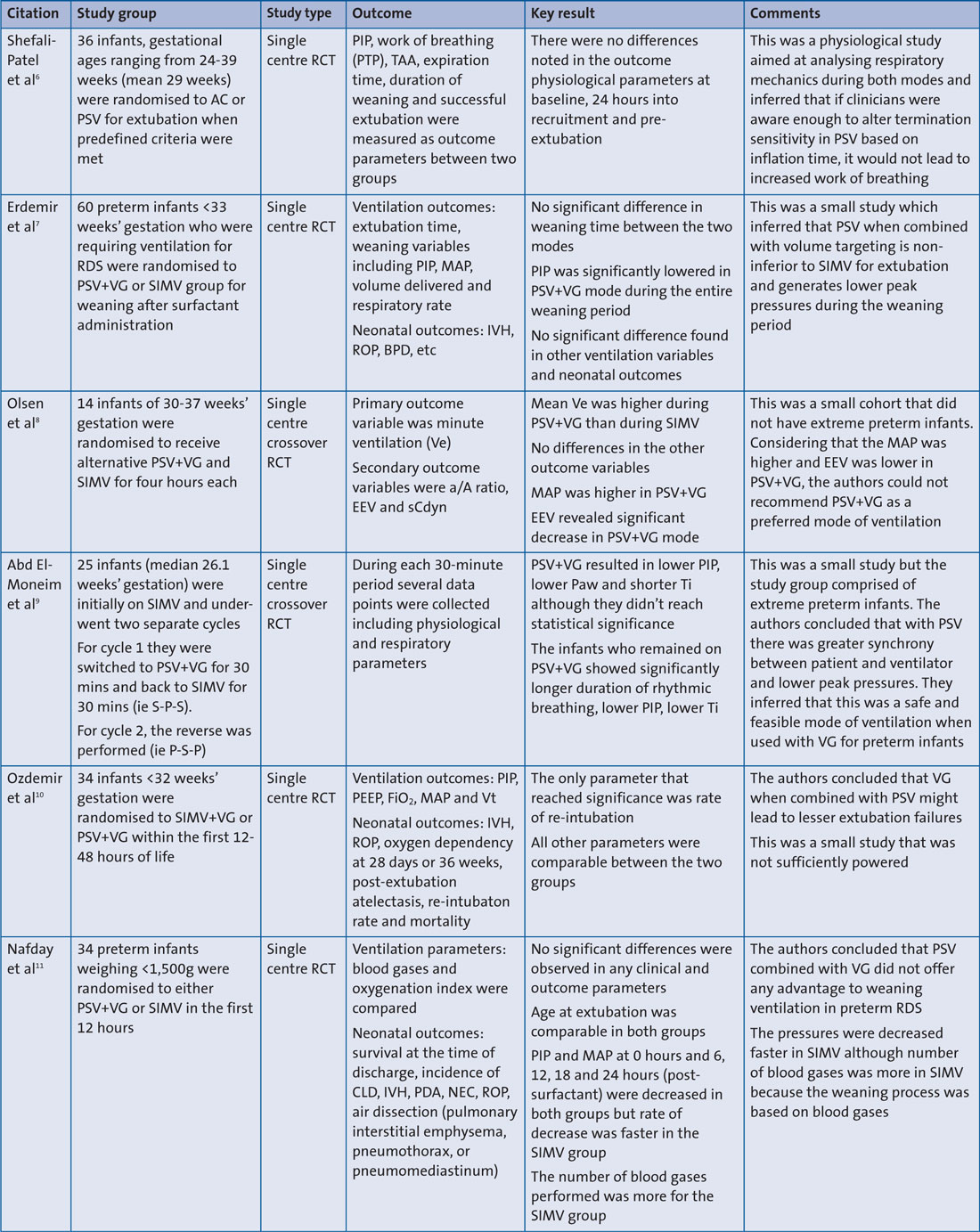
TABLE 2 A summary of the studies with important conclusions. Key: a/A ratio=arterial/alveolar oxygen tension ratio; AC=assist controlled ventilation; CLD= chronic lung disease; EEV=end expiratory volume; FiO2=fraction of inspired oxygen; IVH=intraventricular haemorrhage; MAP=mean airway pressure; NEC=necrotising enterocolitis; Paw=airway pressure; PDA= patent ductus arteriosus; PEEP=positive end expiratory pressure; PIP=peak inspiratory pressure; PSV=pressure support ventilation; PTP=pressure-time product (work of breathing); RCT=randomised controlled trial; RDS=respiratory distress syndrome; ROP=retinopathy of prematurity; sCdyn=specific dynamic compliance; SIMV=synchronised intermittent mandatory ventilation; TAA=thoraco-abdominal asynchrony; Ti=inflation time; Ve=expiratory volume; VG=volume guarantee; Vt=tidal volume.
Results and discussion
All six studies identified in this review were small single-centre RCTs reporting on a total of 169 infants. Five of these compared the hybrid mode of PSV+VG to SIMV or SIMV+VG (one study), and one study compared PSV to ACV. The outcome parameters compared were a combination of physiological and respiratory, ventilation and clinical. Considering the clinical question, three studies compared weaning time or extubation success between the modes (two SIMV vs PSV, and one ACV vs PSV). None of the studies found any difference in time to extubation. One study (Ozdemir et al10) reported on higher reintubation rates in SIMV+VG group when compared to the PSV group and concluded that post-extubation atelectasis might be higher in the former group.
All studies reported on ventilation parameters. There were conflicting results from the studies about PIP and MAP.
If one mode is physiologically superior combined to another for weaning, consistently lower peak pressures would be expected. However, two studies (Olsen et al,8 Nafday et al11) reported higher pressures in the PSV group as compared to SIMV. It is to be noted that in both of these studies VG was added in to PSV while there was no VG with the SIMV, which would mean the pressures were decreased manually in the latter mode and were automatically being adjusted according to lung compliance in the other. Also, the study by Olsen et al8 collected minute-to-minute data instead of a mean data output from the ventilator and this could easily lead to significant fluctuations. The reported tidal volume at the end of the study was, however, lower in the SIMV group as compared to PSV+VG, under-standably due to breath-to-breath variations. Two studies reported a significantly decreased PIP in the PSV group (Erdemir et al7 and El-Moneim et al12).
More detailed physiological parameters were looked into in two studies. One of them (Shefali-Patel et al6) compared PSV with ACV, and the other compared PSV+VG with SIMV. The former assessed parameters such as work of breathing and thoraco-abdominal asynchrony between two modes and inferred on a non-inferiority of PSV when compared to ACV. The study by El-Moneim et al12 reported longer periods of rhythmic breathing in the PSV+VG group (p=0.03) when compared to SIMV. Interestingly this group also published a supplement12 reporting favourable alterations in cerebral blood flow, as evidenced by decreased pulsatility index in the anterior cerebral artery (p=0.002) in infants ventilated on PSV+VG as compared to SIMV.
No studies found any difference in immediate clinical outcomes (eg pneumothorax) or long-term outcomes such as mortality, incidence of CLD and retinopathy of prematurity between PSV and ACV or SIMV. It is worthwhile mentioning that the Cochrane meta-analysis by Greenough et al13 did not report any difference in outcomes compared between PSV used independently or in conjunction with SIMV, but it did show that in preterm infants with weight between 700g and 1,000g, the days of supplementary oxygen were lower in the SIMV plus PSV group (p=0.034) as compared to SIMV alone.
The triggered modes of ventilation depend on a complex interplay of lung mechanics, patient condition, disease pathology and ventilator sensitivity. Physiologically PSV sounds attractive given the fact that there are less wasted breaths and more patient autonomy. A recent physiological meta-analysis14 also concluded that when performing spontaneous breathing test methods for extubation, PSV significantly reduced work of breathing and rapid shallow breathing index. But it has to be remembered that in the neonatal population and especially the preterm cohort, such extubation readiness testing is still not conventionally performed and the work of breathing imposed on a neonate when breathing through a high resistance circuit spontaneously with flow cycling has not been extensively tested.
Conclusion
This review finds no evidence to suggest that PSV alone or in combination with volume targeting (PSV+VG) provides any additional advantage over conventionally used SIMV or ACV when weaning the neonate from ventilation. There is, however, weak evidence to suggest its non-inferiority and that it reduces work of breathing. The studies identified were small, improperly powered, diverse in outcomes and also followed varying protocols. The physiological inferences are appealing but more detailed standardised research is required to make a definitive recommendation in its favour.
Or read this article in our
Tablet/iPad edition
- The conventional method to wean ventilation has been to reduce pressure and/or rate on SIMV or switch to SIMV from assist-control ventilation.
- PSV is a flow-cycled mode of ventilation that is being used with increasing frequency due to strong physiological rationale.
- PSV can be used in isolation or combined with SIMV and VG modes to aid extubation in preterm infants.
Also published in Infant:
