

When should a neonatal death be referred to the coroner? Initiation of a guideline to aid decision making
Despite improved survival, particularly for extremely preterm infants, sadly some neonates die. When this happens, it may be appropriate to refer the death to the coroner, however, there is huge variation in practice between settings regarding the coroner referral process. After a particular case concerning several hospitals, we reviewed available evidence and produced a guideline to aid this process, involving both neonatologists and our coroner’s office, and including parental concerns. This has enabled a systematic, transparent approach that is equal for all infants.
Narendra AladangadyFRCPCH, PhD
Consultant Neonatologist and Honorary Clinical Professor in Child Health, Neonatal Unit, Homerton University Hospital NHS Foundation Trust, London, and Queen Mary University of London
n.aladangady@nhs.net
Philippa Chisholm
FRCPCH
Consultant Neonatologist, Neonatal Unit, Homerton University Hospital NHS Foundation Trust, London
Background
Neonatal intensive care units (NICUs) provide care for the sickest and most fragile infants in our society and, as healthcare professionals, we aim to support families through this intensely traumatic time in their lives. Although strides have been made to improve mortality, and there is evidence of improved survival particularly for extremely preterm infants, sadly some neonates do die.1 When this happens, we have to consider if it is appropriate to refer a neonatal death to the coroner, and if so, under which circumstances.
Often families wish for no further intrusion to their grieving, but it may be a necessary and ultimately helpful process.
A baby’s life and death are influenced by factors affecting pregnancy, labour and delivery and at times these factors also need to be taken into account when thinking about the coroner referral process.2 The process is not intended to be punitive but to bring clarity. The importance of this is not just for neonatologists but needs to be understood by obstetricians, midwives, paediatricians and general practitioners as well as the wider medical community.
In some trusts in the UK, all neonatal deaths are referred to the coroner,2,3 either as part of locally decided clinical guidelines or as mandated by local coronial offices. In others, very few are. Not all neonatal deaths are coroner’s cases; however, there is inconsistency between settings. It is important to note that staff should refer to the coroner referral process in their setting before completing a medical certificate of cause of death.
The role of the coroner is to determine the facts associated with a death – it is not their role to apportion blame.4 This is often misunderstood and leads to fear of referral. Concern that families may be put through unnecessary distress also plays a role.2
After a particular case involving several hospitals where the family had specific concerns and where the coroner should have been involved but wasn’t,5 we sought to write a guideline to aid the decision-making process. We consulted with neonatologists and our coroner’s office, reflected on the family’s experience, and produced criteria that could be applied to deaths on the neonatal unit in determining who should be referred to the coroner.
Referral to the coroner
The guidance from the Chief Coroner in the UK6 states reasons for referral to a coroner, and these categories are given in TABLE 1. The guidance also allows discretion for individual coroners to determine their own reporting arrangements.
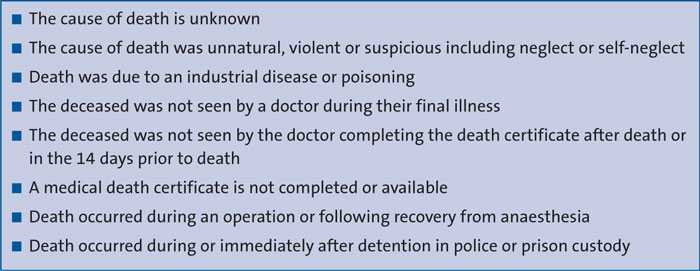
TABLE 1 Reasons to refer to a coroner after death: guidance from the Chief Coroner in the UK.6
For a baby who dies on the neonatal unit, the criteria may be harder to apply and the most likely reason for referral would be ‘cause of death is unknown’. In the context of prematurity or hypoxic ischaemic encephalopathy (HIE), the final cause of death may be known but not the cause of the precipitating event. There are many complexities to both obstetric and neonatal management, and decision making around intervention, which require careful consideration and involvement of family members. These ethical challenges can affect clarity about the appropriateness of referral to the coroner when a baby dies.
Antenatal events may impact neonatal outcome and discussion with obstetric teams should inform the decision. In addition, if a member of the team considers there were any potentially preventable conditions or concerns regarding management, then referral to the coroner should also be considered.
There are occasions when a baby is unlikely to survive irrespective of the medical care delivered, for example extreme prematurity, severe congenital abnormality, and situations where it is appropriate to limit or redirect care with full discussion with the family.7 In these situations referral to the coroner would not be deemed necessary, unless parental concerns are raised. TABLE 2 provides a guide to possible action in recognised perinatal situations, adapted from an Australian guideline.8,9 It is not exhaustive but provides principles applicable to the unique situations on a NICU.
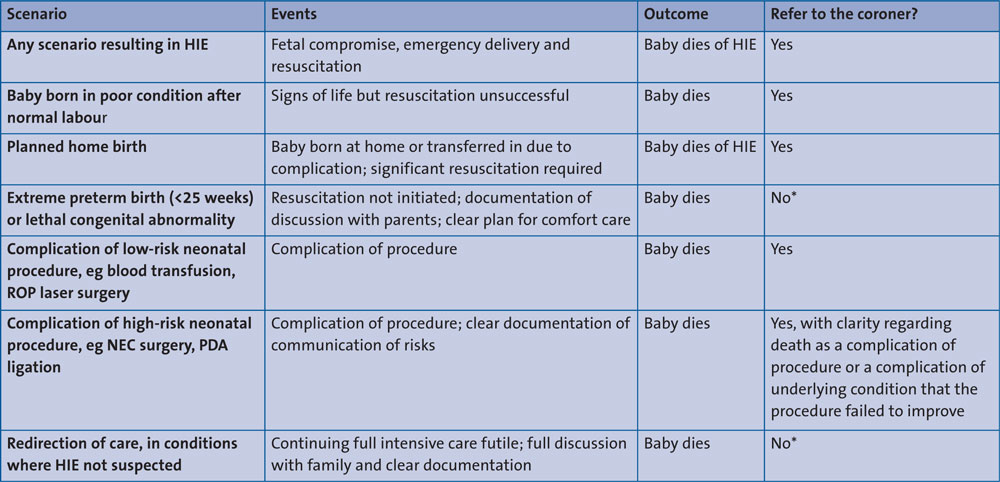
TABLE 2 Recommendations for when to refer to the coroner in different neonatal scenarios. Note, staff should be familiar with the practice in their own setting as local guidelines might state that all cases must be discussed with the coroner. *Unless there are any parental concerns. If the parents express concern about the quality of any aspect of health care or about the decision-making process, even with babies receiving palliative care, the case should be referred to the coroner. Abbreviations: HIE= hypoxic ischaemic encephalopathy, ROP=retinopathy of prematurity, NEC=necrotising enterocolitis, PDA=patent ductus arteriosus.
If there is disagreement about the cause of death or any doubt about referral, a referral to the coroner should be made. The coroner will then make the decision whether or not to accept that referral.6,10 Nomination of a neonatal consultant, such as the departmental mortality or service lead, to support the decision-making in difficult cases, will help to create consistency and avoid any possible confusion or potential complaint.
Once a referral is accepted, the coroner takes legal possession of the body and makes initial enquiries to determine if an investigation, or an inquest, is warranted.10 A coroner’s post mortem may be required. In this situation, a death certificate cannot be issued by the hospital (usually in cases where the cause of death is unknown). However, following discussion with the family and, if the cause of death is known and no concerns are raised, the coroner can allow the certificate to be issued by the treating team without a formal investigation. In this situation, the back section of the death certificate should be filled in to say the coroner has agreed to issue the certificate. This is the most common situation. The wording on the certificate must agree with the coroner’s paperwork.6
It may still be prudent and helpful to discuss post mortem with the family, even if the coroner does not accept the request.
The emerging role of the medical examiner
A new medical examiner system is being rolled-out across England and Wales and in time this might affect the coroner referral process for neonates.11 The system aims to provide greater safeguards by ensuring scrutiny of all non-coronial deaths as well as appropriate direction of deaths to the coroner. It also aims to provide better services for the bereaved and an opportunity for concerns to be raised to a doctor not involved in the care of the deceased. The role of the medical examiner offices will initially focus on the certification of deaths within the acute trust where they are based and includes improving the quality of death certification and mortality data, selection of cases for further review under local mortality arrangements, and contribution to clinical governance procedures.
Conclusion
In the challenging period after the death of a baby there can be uncertainty over whether referral to a coroner is appropriate; clear and consistent guidelines can help alleviate this. Since implementing this guideline in our neonatal unit there has been less confusion in what is communicated to families at the time of death. This aids both families and practitioners in navigating a painful period. Not all referrals are accepted by the coroner but there is a systematic, transparent approach that is equal for all infants.
Or read this article in our
Tablet/iPad edition
- Following the death of a baby there can be uncertainty over whether referral to a coroner is appropriate. Furthermore, there is inconsistency in practice between settings.
- A guideline has been developed to aid decision making for referral to the coroner in different neonatal scenarios.
Also published in Infant:
