

Comparing international survival rates of extremely preterm infants: the impact of variation in reporting signs of life
There is wide international variation in reported survival rates of extremely preterm infants. However, some of this variation might be related to local differences in decisions about whether a baby born at the threshold of survival is considered to be live-born and consequently whether the death is reported as a stillbirth or neonatal death. This variation results in biased comparisons of survival rates.
Lucy K. Smith
PhD
Senior Research Fellow, The Infant Mortality and Morbidity Studies (TIMMS), Department of Health Sciences, University of Leicester
lucy.smith@le.ac.uk
Background
Reported survival rates for babies born at the threshold of survival vary widely between countries, with reported survival in Japan1 and Sweden2 considerably higher than the UK3 and elsewhere. A multinational study team was interested in the possibility that some of this international variation might be related to local differences as to whether a baby was reported as showing signs of life. This Infant article is an overview of a paper exploring survival in seven high income countries including the UK, Japan and Sweden, which was published in Pediatrics.4
As researchers and healthcare professionals it is important that when we make comparisons of survival rates between different countries, we ensure we are comparing ‘like with like’ to avoid misinterpretation. One often overlooked issue is the impact of how we report deaths of babies at the threshold of survival. In some countries, babies may only be considered to be ‘live-born’ if they survive a certain period of time after birth; they weigh more than a specified birth-weight; they are older than a particular gestational age; or there is a decision to provide active treatment. In other countries a baby may be classified as live-born if they show a fleeting sign of life irrespective of their weight and gestational age. This difference in approach affects whether a death is reported as a stillbirth or neonatal death. Since standard neonatal mortality rates only include babies born alive and exclude antepartum and intrapartum deaths, the variation we see in reported survival rates between countries may be partially explained by differences in how deaths are classified at extremely early gestations. In this article the term stillbirth refers to any baby born showing no signs of life irrespective of gestational age, which differs from the UK legal definition of stillbirth which only includes births showing no signs of life from 24+0 weeks of gestational age.
What this study aimed to do
The study aimed to explore survival of babies born between 22+0 and 25+6 weeks of gestational age. Seven high income countries took part: the UK, the US, Canada, Finland, Norway, Sweden and Japan. This study benefits from using national population-based data from each country, removing the problems associated with comparing outcomes from single hospitals, networks of hospitals, or geographically limited populations. The study used the most recent national and population-based birth registry data available in 2017 (this varied between countries – for more detail refer to Smith et al 20184). The number of births by gestational age was obtained along with detailed information on the timing of death (including antepartum stillbirth, intrapartum stillbirth, death within one hour of birth, death within seven days of birth, death within 28 days of birth).
In the UK these data were provided by MBRRACE-UK (Mothers and Babies: Reducing Risk through Audits and Confidential Enquiries across the UK, www.npeu.ox.ac.uk/mbrrace-uk). This article focuses on three outcomes:
- stillbirth
- neonatal death (death of a live-born baby within 28 days of birth)
- live births surviving to 28 days and over.
Further analyses of the timing of death are explored in Smith et al 2018.4
Survival of live births to 28 days of age
Firstly the survival of babies to 28 days was calculated in the standard way – as a percentage of live births (FIGURE 1a). Survival varied at 22 weeks, from very low percentages in Canada (4%), Finland (6%) and the UK (8%) to considerably higher percentages in Sweden (47%) and Japan (57%). Survival improved for those babies born at 23 weeks across all of the countries but wide differences remained. In Canada, Norway and the UK, 20 to 36% of babies survived to 28 days while again rates in Sweden and Japan were much higher at 70% and 79%. Survival increased at 24 and 25 weeks of gestational age and there was less variation between countries.
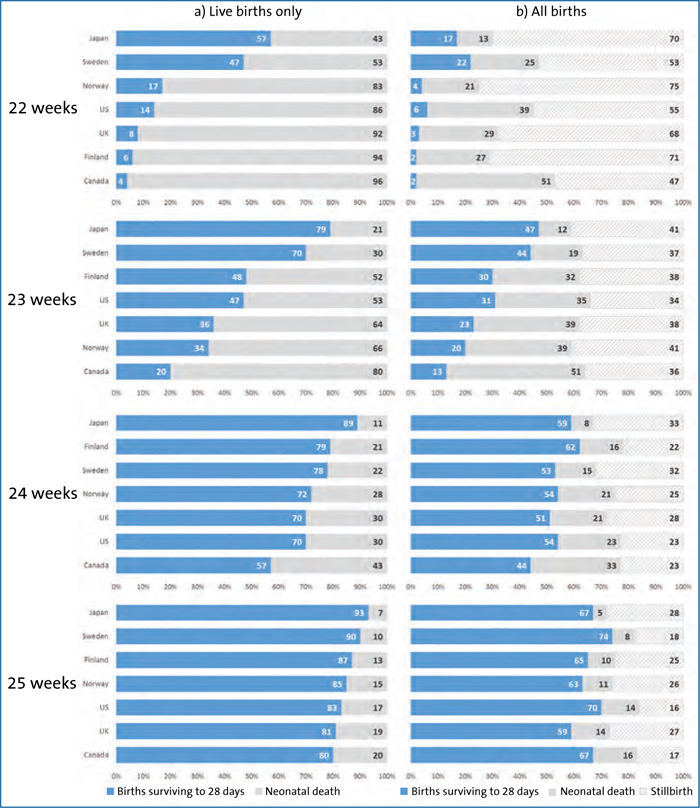
FIGURE 1 Births surviving to 28 days of life as a percentage of (a) live births only and (b) all births by gestational age and country of birth.
Survival of all births to 28 days of age
Next, survival to 28 days was calculated but this time as a percentage of all births, ie stillbirths and live births (FIGURE 1b). At 22 weeks, rates of survival ranged from 2% in Canada and Finland, 3% in the UK to 17% in Japan and 22% in Sweden. This suggested less marked differences between the seven countries. This related to differences in the reporting of births as live-born or stillborn. Canada reported only 47% of births as stillborn compared to 70% in Japan and 75% in Norway. Japan showed the biggest change in survival rates when calculated using all births (17%) compared to using live births (57%), which reflects the relatively high number of births reported as stillborn. However, despite the reduced variation when including all births, international differences in survival were still evident and Japan and Sweden had the highest survival rates based on both denominators.
The percentage of births reported as stillborn were similar for all countries at 23 weeks, ranging from 34% (US) to 41% (Norway and Japan). Therefore the study found that much of the variation in survival rates between countries persisted when survival was calculated as a percentage of all births ranging between 13% in Canada, 23% in the UK and 44% in Sweden and 47% in Japan. Throughout all gestational ages Japan had a higher rate of stillbirths compared to live births and this impacted on the variation seen in survival based on all births or live births only.
What does this mean?
Most importantly, the findings here underline the need for caution when comparing neonatal survival at 22 weeks based on live births. The study highlights the impact of differences in how deaths are classified as stillbirths or neonatal deaths or reported survival to 28 days. Calculating survival as a percentage of all live births has often been thought to avoid the problems of bias seen in studies comparing survival of babies admitted for neonatal intensive care, as admission criteria vary between hospitals, regions and countries.5 However, here we see that criteria for determining whether a baby shows signs of life are also likely to vary and result in biased comparisons.
International differences in the classification of babies as stillbirths or neonatal deaths at 22 weeks are likely to reflect perceptions of viability and may arise from religious and cultural values and the legal environment around registration of deaths. However even after accounting for variations in classification, survival remained higher in Japan and Sweden. While the team did not have access to information on resuscitation and the initiation of intensive care in this study, it is probable that survival relates to differences between countries in initiation of active treatment for babies at the threshold of survival, and whether and when invasive life-supporting care is withheld or withdrawn.
Variation in how deaths are classified is also seen between healthcare providers in the UK.6 While a national framework exists to help guide clinicians approach the management of babies born extremely preterm, no such guidelines are available to assist health professionals in their clinical interpretation of the World Health Organization definition of live birth, regarding how to assess signs of life in these tiny babies. A multi-agency group organised by MBRRACE-UK is currently bringing health professionals, parent groups and government representatives together with the aim of achieving consensus on recommending how signs of life should be assessed at the threshold of survival in order to increase consistency in approach nationally. MBRRACE-UK will also be releasing a report in 2019, providing up-to-date UK data on survival of extremely preterm babies up to one year of age.
Conclusion
Wide variation exists between countries in the neonatal survival rates of babies born at 22-25 weeks’ gestation when considered as a percentage of live births. However, when considered as a percentage of all live births and stillbirths, these differences are diminished. This indicates that some of the differences, rather than relating to the provision of care, may relate to differences in whether babies are considered to be live-born.
Funding and acknowledgements
Lucy Smith is funded by a National Institute for Health Research (NIHR) Career Development Fellowship. This article presents independent research funded by the NIHR. The views expressed are those of the author and not necessarily those of the NHS, NIHR or the Department of Health and Social Care.
The author would like to say thank you to all the other members of the study team: Naho Morisaki, Nils-Halvdan Morken, Mika Gissler, Paromita Deb-Rinker, Jocelyn Rouleau, Stellan Hakansson, Michael R. Kramer and Michael S. Kramer.
Or read this article in our
Tablet/iPad edition
- Reported survival rates for extremely preterm infants vary widely between countries.
- A recent study indicates that this variation may relate to differences in which babies are classified as live-born.
- There is a need for caution when comparing neonatal survival based on live-born babies at extremely early gestations.
Also published in Infant:
