

Consideration of care in a preterm neonate with an extremely rare skeletal dysplasia
Receiving a lifelong diagnosis at birth can be viewed as the starting block from which a life is built and lived. We present the case of a preterm neonate born with a severe skeletal dysplasia in an endeavour to understand the challenges facing the different aspects of care provision, management and treatment in the special care baby unit at Calderdale Royal Hospital. Encompassing the experiences of the staff/parent relationship, we hope to initiate discussion about how best to accommodate such babies on the unit and hypothesise approaches to improving care to stand the family in good stead for their lifelong journey.
Kate F ParmenterST2 Paediatric Trainee
kate.parmenter@nhs.net
Katarzyna A Cooke
ST4 Paediatric Trainee
Amelia Penny
Senior Sister Neonatal Intensive Care Unit (QIS)
Pamela Ohadike
Consultant Paediatrician with specialist interest in neonatology
Abdul Mattara
Consultant Paediatrician with specialist interest in neonatology
Special Care Baby Unit, Calderdale Royal Hospital, Halifax
Case presentation
A male infant was delivered at 32+2 weeks gestation by an emergency caesarean section due to concerns about tailing growth and a pathological cardiotocograph (CTG). He weighed 935g (<0.4th centile). The newborn infant’s gross appearance was indicative of marked skeletal dysplasia – quadrilateral phocomelia FIGURE 1. Both forearms had underlying skeletal anatomy comparable to a humeral bone. The right had a crude elbow joint, but this was fused in an extended posture. There was a 1x1cm fleshy limb bud on the medial aspect of the right limb. This appendage was well perfused but had no motor ability. The left forearm was a short humerus alone.

FIGURE 1 Quadrilateral phocomelia on day 5 of life.
Upon examination he had only softly dysmorphic facial features. Of note, there was mild mid-facial crowding with subtle upturning of the nose and a thin upper lip. The palate was high arched with no cleft. Ears were set appropriately, and occipito-frontal circumference plotted on the 9th centile. He had a micrognathic jaw with a retrognathic position. The chin was pointed and triangular. A systemic examination was otherwise unremarkable.
He had abnormal pelvic anatomy both radiologically FIGURE 2 and pheno-typically. At birth, there was a leg limb length discrepancy of roughly 2cm. The right limb was fully mobile from the hip joint with no association to the hip itself. The limb progressed to a fleshy appendage that could be most suitably likened to an early foot growth. This again lacked skeletal growth but could be flexed with some limited rotation around the apparent joint. There were two further buds at the distal aspect of the foot with some primitive ridges of differentiation giving suggestion of two potential toes. The largest of these had indentations of a nail bed but no keratinisation.
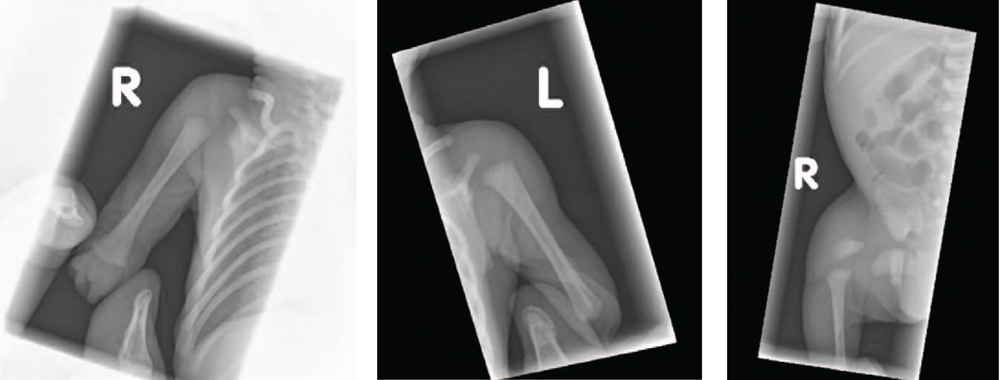
FIGURE 2 The radiographic appearance of the limbs showing marked skeletal abnormalities.
The left lower limb was extremely short; 1.5cm in length. On palpation the bone was thin and bowed. In contrast to the other appendages outlined, this bud had some underdeveloped foot bones.
Diagnosis and postnatal investigations
Antenatal concerns regarding the absence of limbs were first identified on the 20 weeks’ anomaly scan. These were later confirmed on a skeletal survey as under-development of the long bones in the upper and lower limbs, indicative of congenital quadrilateral phocomelia. Both humeri were intact with neither progressing to structures of the forearm or hand.
A postnatal ultrasound of the right hip demonstrated no femoral head, the femur itself was immature: a short segment of bony tissue completely absent from the acetabulum. On the left there was only a tibia with a few short bones distally, indicative of early foot bone formation.
Investigations after birth revealed the baby had normal appearance of his cranial contents, renal system and heart.
Genetic screening was negative for Fanconi anaemia and Roberts syndrome, both of which are characterised by limb abnormalities. DNA analysis identified a copy number variance of unknown clinical significance.
Management on the special care baby unit (SCBU)
Initially the infant required non-invasive ventilation, which was gradually weaned and discontinued on day 3 of life.
He established feeds with nasogastric tube support and then transitioned onto responsive bottle feeding by four weeks of age. He did not receive parenteral nutrition and managed increases in the volume of enteral feeds with infrequent episodes of intolerance, which did not affect his growth or weight gain.
After birth, he was screened for early onset sepsis due to pertinent risk factors of spontaneous onset of premature labour and prolonged rupture of membranes. Although screened for a second episode of suspected sepsis on day 5 of life following a profound apnoea, cultures were negative with no relative rise in inflammatory markers on serial measurement. Notably, he had no positive microbiology results over the course of his admission. He required a brief period of phototherapy treatment for physiological jaundice.
Discharge and follow-up
The baby was discharged home at 39 weeks’ corrected gestation weighing 1,710g following a 48-day stay on SCBU. The follow-up and support were arranged within a multidisciplinary team (MDT) consisting of dietitians, physiotherapists, occupational therapists and the local general paediatric team.
Challenges for neonatal care
Many logistical challenges to basic care provision arose, in particular:
- obtaining peripheral intravenous access
- recording accurate blood pressure
- pulse oximetry monitoring
- positioning to prevent pressure breakdown
- fitting nappies securely to his unique anatomy.
He was born preterm and his weight was estimated to be small for his gestation. This was further compounded by the absence of limbs, which further reduced his weight. The MDT had to decide how best to correct for this when considering his feeds and medication administration. As a consequence, there was a slight delay in commencing enteral feeds. The issue was resolved after detailed discussion among the medics, nurses, dietetics service and his parents; he would be treated as though he was a baby presenting with severe intra-uterine growth restriction.
Input from the physiotherapy and occupational therapy teams was vital in managing the baby, not only in the short term while under the care of the unit, but also looking to the long-term consider-ations for his successful growth and development. This would be essential – ensuring maximal longevity and engagement in services when outlining strategies for minimising undesirable symptoms in the future, such as spasticity and contractures. In addition, promoting early and continual momentum in progressing mobility, muscle training for appropriate functionality and directed guidance about which of the multitude of prosthetic devices would be beneficial in allowing him to reach developmental milestones.
Perhaps the biggest challenge for the neonatal team was the working relation-ship with the family. It was paramount for us to get this right in order to deliver family-centred care and set this family onto an appropriate pathway for their future lives. However, we often found the situation fraught and perhaps we made subtle mistakes that potentially damaged the relationship. It is this aspect of care that we would like to focus on in our discussion.
Discussion
Phocomelia
Phocomelia is an extremely rare birth defect characterised by severe malfor-mation of the limbs, typically shortened or absent arms and/or legs. Fingers and toes can be fused together. Defects of the eyes, nose and ears may also be present. The term phocomelia comes from the Greek for ‘seal-limbed’. First discussed in 1836 by the French naturalist Etienne Geoffroy Saint-Hilaire,1 the condition came to notoriety in the 1960s with the use of the drug thalidomide for the amelioration of morning sickness. Thalidomide’s use led to over half of the exposed population being born with morphological features, especially limb deformities.2-3 About 40% of babies with thalidomide-induced defects died in the first year of life.
Phocomelia can occur sporadically and may also be inherited in an autosomal recessive pattern with mutations linked to chromosome 8.4 Total prevalence is estimated at 0.62 per 100,000 births world-wide.5 Phocomelia is linked with learning difficulties and babies often exhibit microcephaly, micrognathia (small lower jaw), orbital hypertelorism (wide-set eyes) and a cleft lip, with or without a cleft palate.5,6 Encephalocele, hydrocephalus, bicornuate uterus, coagulopathy and structural abnormalities of the heart and kidneys have also been documented.
Treatment of the condition is supportive. An array of prosthetic devices can be used; recent advances in myoelectric limbs in patient cohorts are promising. Surgery may be able to rectify deformations of the face. Ultimately, the aim is to improve and maximise quality of life, allowing for purposeful integration into the family and wider community.
The trilogy of care
To fully understand the complexities surrounding this case, each key element in the trilogy of care provision – the parents, the baby and the neonatal unit – should be considered FIGURE 3.
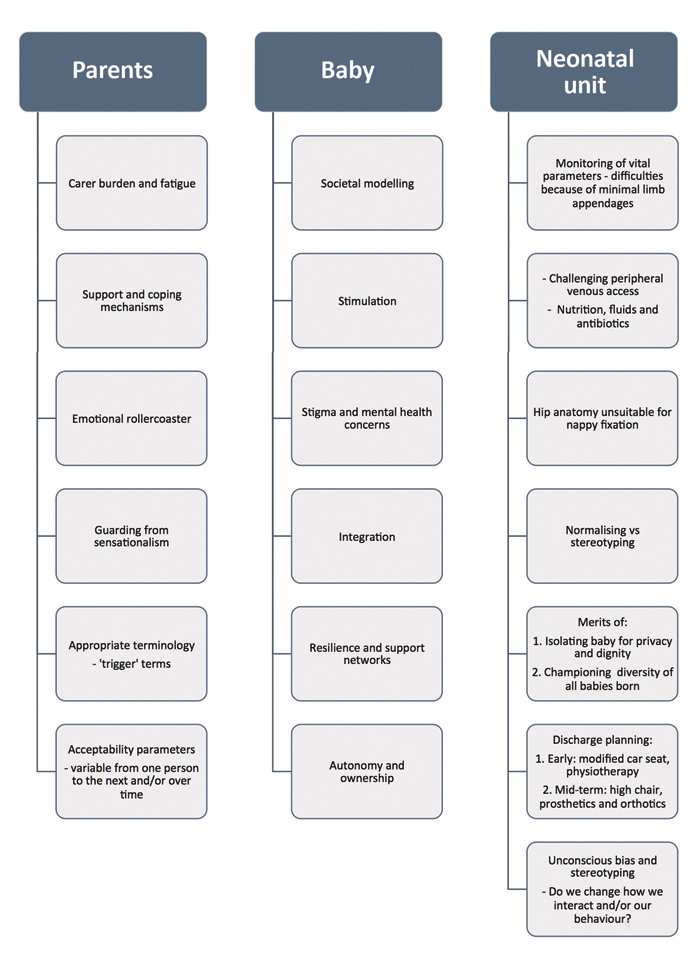
FIGURE 3 Key elements in the trilogy of care provision – challenges for the parents, the baby and the neonatal unit.
The parents
Although aware antenatally that their journey with this baby would be unlike the journey they had with their two previous sons, it is very difficult to imagine exactly how the parents would have conceptualised how much things would have to change to facilitate this new arrival.
In addition to the ‘whirlwind of emotions’ parents usually experience during pregnancy, there will have been additional stressors in having a baby born with disability and dysmorphic features. The landscape of family dynamics would be forever altered. Financially there would be new strains as their son would most likely require near-full-time care.
Upon the birth of their baby, the care burden increased as they had to look after their other children and adjust their lives to incorporate this new child. With any new baby there is a time of adaptation where the ‘routines’ (practical and emotional) of the parents and siblings must change to bring a new baby into the family circle. The parents were often absent from the ward, often coming later in the day, thus missing daily management updates. The father was an infrequent visitor, presumably because of work commitments and caring for the other children. It took the mother some time to build up to caring for her son and to touch and hold him when unclothed.
Understandably, both parents could be hostile to members of staff who uninten-tionally used certain terminology, ‘trigger’ words and phrases. This led to preferred staff caring for the baby and, on occasion, disrupted the optimum workings of the ward, potentially detrimentally affecting the care for other babies. Other parents were reprimanded if their gaze lingered too long or kind words were misconstrued as sympathy or pity. Obviously, the parents were experiencing unimaginable struggles, but this was also very challenging for the staff and other families on the unit.
It is clear that the mother was protective of her son, guarding him from sensation-alism, but there was a conflicted quality to this. On the one hand she did not want him to be a spectacle yet on occasion she acted as though he was. She expressed guilt that this had happened to her son and mentioned on more than one occasion that she had been offered a termination of the pregnancy. She appeared to go through cycles of guilt and blame. She did not engage with any other parents on the unit.
In FIGURE 4 we include a reflective log from a senior neonatal sister, which retrospectively identifies some of the challenging care themes. By highlighting these signs, we hope we can learn from this case so that we can modify our actions in future instances for the benefit of the doctor/patient relationship.
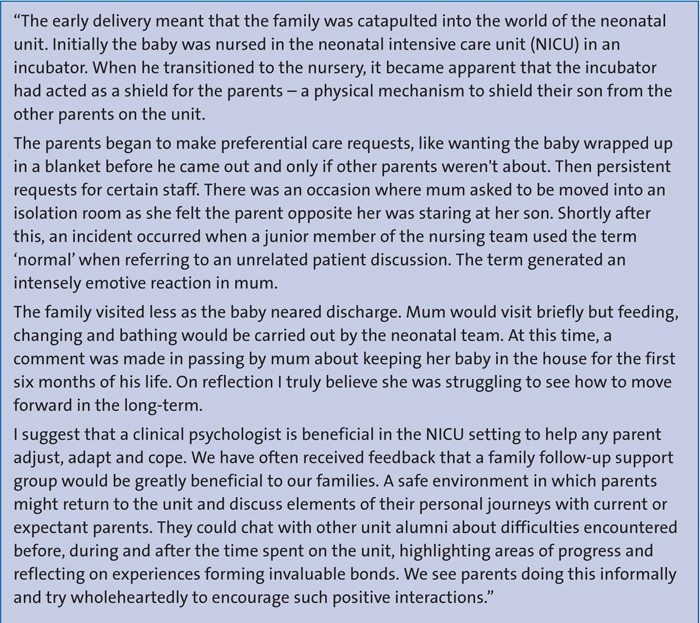
FIGURE 4 Reflections from a senior neonatal sister.
The underpinning ethos here is routed in determining why the parents had the adjustment reaction they did. It could be considered that neonatal units are undeprepared when supporting parents in such positions. These parents, if not all parents on the unit, would have probably benefitted from formal support, whether this was with the basic practicalities of unit life or regular check-ins with mental health workers and trained psychological practitioners.
In maternal mental health week in April 2018, Bliss highlighted the importance and need for more accessible psychological support on all neonatal units and called for government funding to action this imperative. It is well understood that having a baby born either preterm or in need of intensivist intervention leads to a higher incidence of postnatal depression. Recent figures indicate a dire lack of provision with 41% neonatal units having negligible access to a trained mental health worker and only 30% having any psychological support.7-9
The baby
The World Health Organization cham-pioned the International Classification of Functioning, Disability and Health (ICF) during the 54th World Health Assembly in 2001. It was approved by all 191 member states and replaced the outdated 1980 International Classification of Impairments, Disabilities, and Handicaps (ICIDH).10
In 2007 the International Classification of Functioning, Disability and Health for Children and Youth (ICF-CY) was published, which integrated developmental aspects and inclusions codes. Together these were added to document the child’s interaction with their environment more discretely and so inform on key influences aiding functioning and development.
The ICF can be broadly divided into three categories:
- body functions and structures (impairment)
- activities (limitations)
- participations (restrictions).
The ICF was designed to be a bio-psycho-social-spiritual approach in the context of ethics, human rights and legal frameworks. It is intended to be a tool through which patients, parents and healthcare professionals can work in order to implement sustained positive change in the complex and often interlinked domains of the physical, mental and social aspects of a child’s health condition. Professionals from within the MDT would observe a patient performing their daily activities and note the patient’s functional abilities. This information would then be used to determine the extent to which the individual’s abilities might be improved through therapy and to what extent the environment could be changed to facilitate performance.11 The stance is taken that a diagnosis is important in defining the causality of a disease and, to a limited extent, the prognosis. However, under-pinning and identifying limitation of function as a child grows and develops is actually what drives management planning and intervention.12
Despite these measures, for this child there will always be difficulties to overcome due to the societal modelling of education; employment, cultural and governmental imperatives; environmental and organisa-tional barriers; access to resources and parental income. Stimulation will be an integral factor in this boy’s life, helping him to reach developmental milestones and to learn how to communicate and appropriately socialise. Integration into society is imperative so as to gain access to skills and services that will improve his quality of life. Hopefully his brothers will help catapult him into language and motor skill acquisition through play and social exchange.
The neonatal unit
As a unit, we struggled to manage our relationship with the parents in this setting. We found very little in the academic literature on care themes and how to approach such cases.
With hindsight, we hypothesise how we might have inadvertently damaged the autonomy and empowerment of our parents by promoting what we thought they needed to do, rather than asking them for their position first. We risk alienating vulnerable people at a juncture where they don’t need an ‘expert’. With conditions as rare as this, the parents are the authority – not the medics.13 Healthcare professionals can potentially compound the issues by having a paternalistic and didactic inference; we ‘must know what is best for a family’ so there is a subconscious bias in the way we prescribe support and social care practices. On reflection, the more we strove to normalise her baby, the more uncomfortable the mother appeared.
We became incredibly fond of this baby and collectively he reminded us that a culture of caring is not just about the plans made on ward round. The ego of medical professionals should not harbour preconceived ideas or agendas when tackling complex dilemmas in babies born with severe disabilities.
We propose a change in the institutional attitude towards how we manage our relationships with parents in the setting of our complex care neonates FIGURE 5. We are a passenger in this journey for a very finite amount of time, often with long-lasting and wide-reaching consequences. Our role in planning for discharge should be that of a negotiator, mediating on the part of our charges to facilitate the all-important decision-making process. The mission statement universal to all neonatal units must be to individualise all the care we give and remember; the baby is out patient but this is the parents’ child. We must listen.
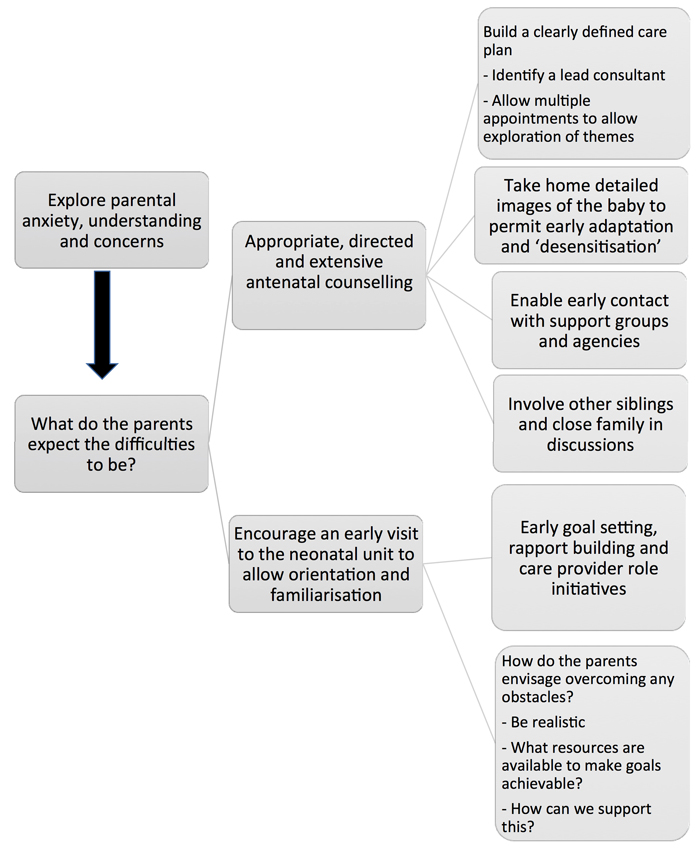
FIGURE 5 An approach to the care of babies born with an extremely rare skeletal dysplasia or those predicted to have complex care needs.
Concluding comments
Following discharge, the parents have been in contact with social services and have been delegated a case worker to help them with resource procurement. Unfortunately, follow-up with physiotherapy and occupational therapy teams has been difficult due to COVID-19 government restrictions. We are told that the baby is progressing well; he is due to be seen in the neonatal follow-up clinic.
Although the diagnosis in this case is a rare one, essentially it is unimportant to the message and learning points we aim
to convey, ie regardless of why a family may need to spend time within neonatal services, there must always be an appreciation for holistic patient and family-centred care prerogatives. We advise an early focus on appropriate antenatal counselling and introduction to support providers. A consideration for timely orientation and familiarisation of parents to the unit and MDT, with active attention to increasing access to psychological support.
Our commitment and responsibility to care should not end once families leave the acute setting – there must be robust follow up with key members of the MDT and clear signposting for parents to seek advice or guidance.
Expectations on how we provide care and ideals on exactly how this should be delivered will vary vastly. So too will the level of input families need or want at any given time or the level of support wanted from services upon discharge. It is very likely that these requirements will change over time.
Parental consent
The authors declare that parental consent was obtained for the use of these images and writing of the report; the parents have approved the content for publication in Infant.
Or read this article in our
Tablet/iPad edition
- The ways in which we manage complex care neonates can have long-lasting and wide-reaching consequences.
- Neonatal healthcare professionals must always deliver holistic patient and family-centred care.
- Our commitment and responsibility to care should not end once a family leaves the acute setting.
