

Nocturnal sleep architecture of preterm infants in the NICU
Sleep is the main behavioural state of the preterm infant and a prerequisite for normal neuronal maturation and cortical development. Neonatal electroencephalography (EEG) is a useful cot-side tool providing a unique view of sleep state organisation. This observational study describes the sleep architecture of mid to late preterm infants in a neonatal intensive care unit (NICU) setting. As the preservation of sleep supports neuronal maturation, routine overnight disturbances are recorded and quantified.
Mary Anne Ryan1,2
RGN/RSCN/RM, PhD Student
maryanne.ryan@ucc.ie
Sean Mathieson1,2
PhD, Clinical Physiologist
Vicki Livingstone1,2
PhD, Biostatistician
Marc Paul O’Sullivan1,2
PhD, Postdoctoral Researcher
Eugene Dempsey1,2,3
MD, FRCPI, Professor of Paediatrics and Consultant Neonatologist
Geraldine Boylan1,2
PhD, Professor of Neonatal Physiology and Director of the INFANT Research Centre
Sleep is a prerequisite for neuronal maturation, normal growth, development, cognitive function and memory consolidation at any age but particularly during the accelerated period of brain development that occurs in the last trimester. Sleep architecture or sleep organisation in the healthy newborn infant is characterised by regular sleep-wake cycling (SWC), alternating between periods of active sleep (AS) (precursor of rapid eye movement sleep, REM), quiet sleep (QS) (precursor of non-rapid eye movement sleep, NREM), indeterminate (IS) or transitional sleep (TS) (showing features of both AS and QS) and wakefulness (W). Continuous video encephalography (vEEG) during sleep allows for the accurate identification of SWC.
Moderate to late preterm infants (MLP) are defined as infants with a gestational age between 32 and 36+6 weeks at birth.1 This single homogenous group are the largest and fastest-growing proportion of the preterm infant population and represent 75-80% of all preterm births. This study aims to describe the nocturnal sleep architecture of MLP in the NICU and to quantify the number and purpose of SWC interruptions during this period.
Sleep architecture development
While both AS and QS are prerequisites for neuronal development, the contribution and role of each are likely to be different and unique to gestational age. AS is the dominant state in the MLP with the percentage of QS increasing with advancing gestational age.2,3 Sleep state organisation evolves with maturity during which fluctuations or cycling between sleep states support the normal neuro-developmental process and is considered a surrogate marker for neurological wellbeing.4-6 SWC patterns are clearly recognisable on EEG from 31 weeks’ gestation7 although elements of differen-tiated states precede this time frame. Delayed cycling or disorganised sleep in the low-risk preterm infant is associated with neurological dysfunction such as poor emotional regulation and cognitive development.5,8,9 Sleep state may be determined based on behavioural analysis and/or visual analysis of EEG activity.
Behaviour sleep analysis
Behavioural sleep state analysis focuses on attributes of the infant, presenting a unique pattern of behaviour for each sleep state (TABLE 1).10 These states are readily observable and can be reviewed later if video is used with EEG monitoring.
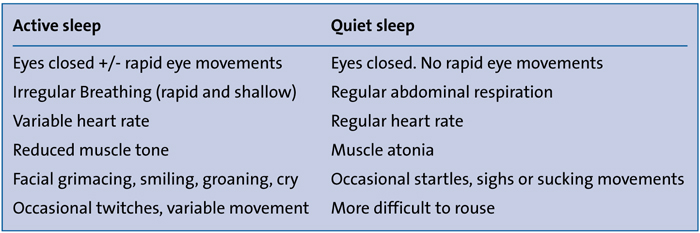
TABLE 1 Behavioural features of sleep.
Behavioural observations during sleep in a preterm infant are less obvious in comparison to the term born infant. Difficulty identifying the exact timing and onset of AS and QS may arise due to frequent body movements and rapid alterations between states in the preterm infant.11,12 A decrease in body movements and respiratory patterns becoming more regular reflect the preterm infant’s neurological maturation.
Visual analysis of sleep on EEG
EEG provides an opportunity to gain further insight into the complex nature of sleep, particularly the microstructure. While interpretation of the complex features of the immature preterm EEG requires a specialist neurophysiologist, sleep state identification may be achieved with minimal cot-side training/education and is a useful marker of brain function and maturity.13
Prior to evaluation of the EEG, information pertaining to gestational age at birth, postmenstrual age (PMA), medication and physiological condition is crucial. Non-cerebral changes in the EEG may be due to artefact due to technical (eg rhythmic vibration caused by a high frequency ventilator) or physiological (eg sucking or movement related or muscle related or blinking)14 causes and may be sustained, transient or repetitive. Correct identification of artefacts will ensure accurate interpretation of recordings.15,16
Modern EEG devices display both the raw EEG and a compressed EEG trend called the amplitude-integrated electro-encephalogram (aEEG), as seen in FIGURES 1-4. The aEEG is derived from the raw EEG by filtering and processing the signal to produce a compressed representation of the maximum and minimum amplitude range of the EEG. The narrower band areas of aEEG represent the low amplitude high-frequency activity that occurs in AS and W and the wider band representing QS. Long-term trends or SWC over many hours are best seen on aEEG.
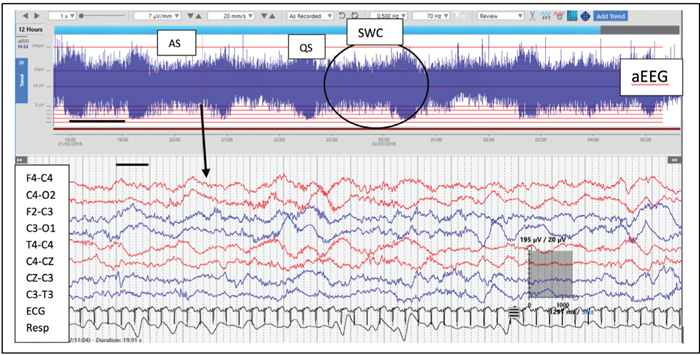
FIGURE 1 Active sleep. Infant born at 33+3 weeks’ gestation, recorded at 35+5 weeks’ PMA (day 16 of life). One complete SWC circled on aEEG. Raw EEG showing high frequency continuous activity of low to medium amplitude. Irregular respirations observed.
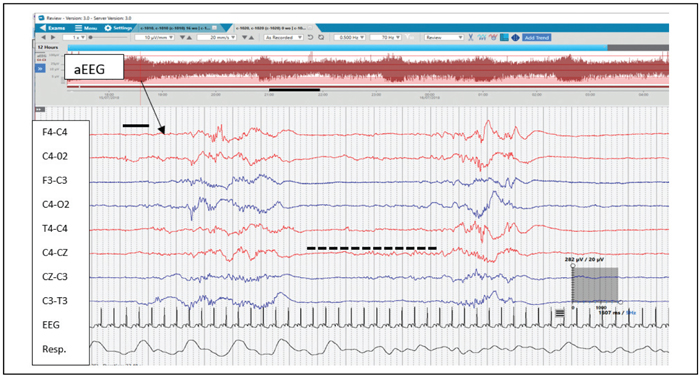
FIGURE 2 EEG recording during QS. Infant 36+3 weeks gestation at birth and recorded at 36+5 weeks’ PMA (day 3 of life). The broken black line indicates the IBI duration. An IBI or period of discontinuity for 5 seconds is evident in and within normal range for a this gestational age infant.
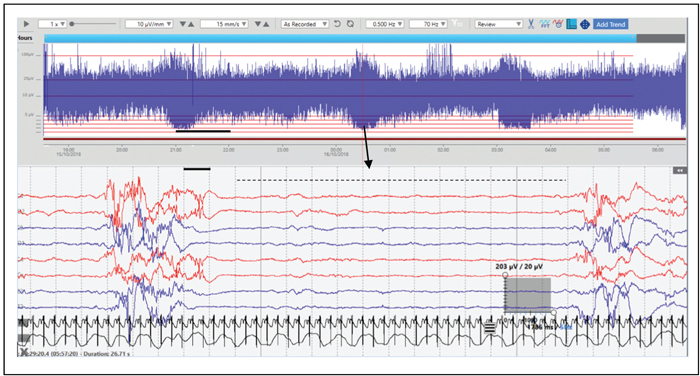
FIGURE 3 EEG recording during QS. Infant 33+6 weeks’ gestation at birth and recorded at 35+5 weeks’ PMA (day 13 of life). A more immature EEG in comparison to that illustrated in FIGURE 2. A longer IBI of approximately 13 seconds is seen.
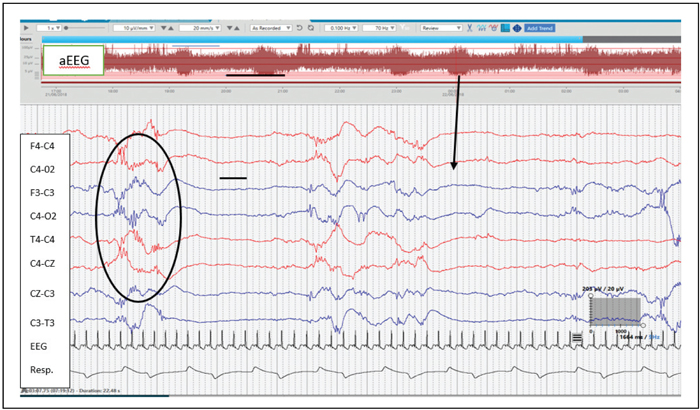
FIGURE 4 Delta brushes – a characteristic feature of the preterm EEG indicated in the black circle. Delta brushes are seen as delta wave activity (<4Hz) with superimposed fast activity.
In the healthy MLP infant, EEG background activity varies and is dependent on sleep state and degree of prematurity.2,16 Knowledge of age-appropriate features of prematurity will assist in assessing sleep states on the EEG. In general terms, the EEG can be assessed within the following parameters:
Frequency of brain wave activity per second (Hz). The four main frequencies of interest in neonates are: delta activity, which has a frequency of 4Hz or less; theta 4-7Hz; alpha 8-13Hz, and beta activity of 13-30Hz. Higher frequencies exist but are minimally present in neonatal EEG.
Amplitude or size of the waveforms. On the EEG amplitude is measured in microvolts (µV). Amplitude may be described as low (0-25µV), moderate (as 25-75µV) or high (>75µV). In FIGURE 1 the amplitude of the recording during AS is low to medium. In FIGURES 2 and 3 the amplitude in QS is low with intermittent bursts of high amplitude activity.
Continuity of background activity. This describes whether EEG activity is continuously present or is intermittent (discontinuous). The amount of continuity increases with advancing gestational age and is dependent on sleep state. From 32 weeks’ gestation, continuous activity is evident in AS (FIGURE 1) In QS, discontinuity is seen on EEG of the preterm infant, which reduces with advancing gestational age (FIGURES 2 and 3).
Origin (location) of activity. For example, frontal, temporal, parietal, occipital or central.
Degree of synchrony and symmetry. The extent of synchrony (brain wave activity of similar type occurring simultaneously over both hemispheres) and symmetry (similar EEG amplitude and frequency content over both hemispheres) of EEG activity.
The EEG in AS in the MLP infant shows continuous low to moderate amplitude, higher frequency activity with frequent physiological artefacts due to movement and REM activity (FIGURE 1). In QS, periods of low voltage activity alternating with periods of higher amplitude activity (bursts) are seen (FIGURES 2 and 3). The period between bursts of activity is termed the interburst interval (IBI). In healthy preterm infants, the IBI decreases with advancing age as the EEG becomes more continuous.17 The expected IBI for MLP is 10-15 seconds at 34 weeks’ PMA and <10 seconds at 36 weeks’ PMA. The black broken line on FIGURES 3 and 4 highlights the duration of the IBI.
Spontaneous activity transients are independent waveforms of activity, acknowledged as having distinct functional properties, evident on EEG and associated with particular gestational age.2,16,18 The most recognisable spontaneous activity of the preterm EEG are delta brushes, which are seen as slow delta waves (1-2Hz) with an amplitude of 100-200uV (peaking at 34-35 weeks’ PMA) with superimposed fast or high-frequency alpha or beta activity.13,19 The peak frequency of this superimposed activity is 16-20Hz between 32-35 weeks’ PMA, falling to 10-15Hz from 36 weeks’ PMA.20 Delta brush activity occurs in both AS and QS (more dominant in QS of the MLP) with the fast frequencies most frequently appearing in the ascending arm of the delta wave.16 The presence of delta brushes is most evident between 32-35 weeks’ PMA and disappearing by 38-42 weeks’ PMA (FIGURE 4).21
The disappearance of delta brushes occurs in conjunction with the development of clear sleep state differentiation, suggesting an association with neuronal maturation and development.20,22 Other normal spontaneous transient waveforms of prematurity include: premature temporal theta; encoches frontales, and anterior slow dysrhythmia, as described by Pavlidis et al and Andre et al.13,16 The aim of this study was to identify and quantify SWC on EEG of a cohort of MLP infants and quantify sleep disturbances overnight in the neonatal unit.
Methods
This is a single centre observational study focusing on sleep patterns of healthy MLP infants who required admission to the neonatal unit at Cork University Maternity Hospital (CUMH), which has a birth rate of approximately 7,500 babies per year. All infants with a gestational age of 32-36+6 weeks at birth, who were clinically stable with no actual or suspected congenital or chromosomal abnormality and no neurological concerns were eligible for inclusion in the study. Ethical approval was granted by the Cork Research Ethics Committee.
All EEGs were performed in a quiet area of the neonatal unit between 16.00hrs and 18.00hrs for a minimum of 12hrs. A reduced neonatal montage was used based on a standardised international 10/20 system of electrode placement propor-tional to skull size.23,24 Electrode positions included F3, F4, C3, C4, T3, T4, O1, O2, Cz, reference (R) and ground (G) with ECG and an abdominal respiratory sensor was also applied. Impedances were <10kΩ before the commencement of EEG recording. All efforts were made to keep EEG artefact at a minimum for accurate interpretation of recording.
A SWC was defined as the commence-ment or onset of AS followed by QS (+/- IS) with cycling between states occurring until awakening. Sleep states were annotated by a research nurse (Mary Anne Ryan – MR) with extensive EEG experience and based on vEEG which combined typical infant behaviours and visual analysis of EEG activity. Annotations from a random sample of recordings were also independently reviewed by two neuro-physiologists to verify sleep annotations by MR. SWC was quantified by visual inspection of the EEG and the duration of all sleep-wake states and feeding periods were annotated on each recording. As per unit policy, no routine procedures or examinations were carried out overnight and the neonatal unit standard of care was not altered throughout the monitoring.
All recordings were reviewed by a neurophysiologist for any abnormal incidental findings. All recordings were then pseudo-anonymised before transfer to a secure server for long-term storage.
Statistical analysis was performed using IBM SPSS Statistics (version 25.0, IBM Corp, Armonk, NY, USA). Continuous variables were described using the median and interquartile range (IQR) and categorical variables using frequency and percentage. For infants who fed orally with ≤1 nasogastric tube (NGT) feed overnight, a random-effects model was used to investigate if the duration of oral feeding (feed given closest to midnight) differed by type of awakening (interrupted versus spontaneous). Type of awakening was a fixed effect in the model, subject was a random effect and an unstructured co-variance was used. The Mann-Whitney U test was used to investigate if the duration of oral feeding differed by sleep state from which the infant was woken (quiet versus active). All tests were two-sided and a p-value of <0.05 was considered statistically significant.
Results
Informed parental consent was obtained for 117 MLP infants. Due to early discharge home or transfer to provincial hospital (14 infants), later exclusion criteria (two infants) or poor quality EEG (three infants), 98 overnight vEEGs were available for analysis. All participants were clinically stable at the time of the recording. Demographical data and overnight SWC of infants are shown in TABLE 2. The number of male and females were similar (52 males, 46 females) the majority of whom were nursed in a cot (80.6%).
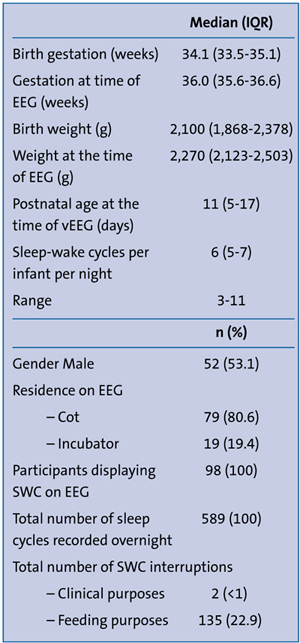
TABLE 2 Demographic data and overnight SWC recorded over a 12hr period (n=98).
SWC was identified on the EEG recording of all participants. The median (IQR) number of SWCs overnight was 6 (5-7) (TABLE 2). Of the total overnight SWCs recorded (n=589), 23.3% (n=137) were interrupted. On two occasions sleep was interrupted for clinical reasons. The remaining interruptions were exclusively for feeding and occurred during both AS (77.8%) and QS (22.2%).
Feeds were given either orally (78.8%) or via a NGT (21.2%, TABLE 3). On 68.8% (194/282) of occasions when infants were being fed orally, the infant woke spontaneously prior to the feed. For the remaining 31.2% (88/282) of occasions, infants were actively woken. When infants were fed via a NGT, they had their sleep disturbed prior to the NGT feed on 61.8% (47/76) of occasions. For the remaining 38.2% (29/76) of occasions, infants were undisturbed and slept throughout the NGT feed (TABLE 3).
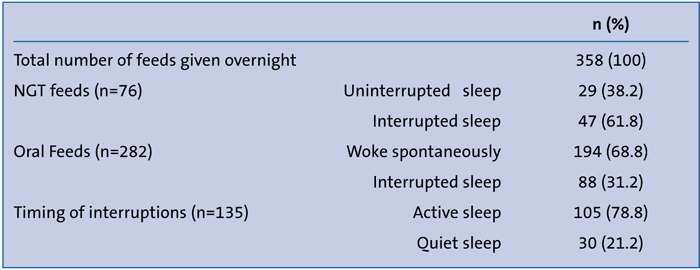
TABLE 3 Overnight feeding interruptions.
Based on the feed given closest to midnight, the duration of the oral feed was significantly longer when the baby was interrupted from their sleep compared to when the infant woke spontaneously (n=83). The estimated average feed duration was 24.13 minutes (95% confidence interval: 20.55 to 27.71) when the baby was interrupted from their sleep and 17.85 minutes (95% confidence interval: 15.38 to 20.31) when they woke spontaneously (difference in means: 6.28 minutes; 95% confidence interval: 2.22 to 10.35 minutes; p=0.003).
Further analysis investigated if the duration of feeding depended on the sleep state from which the infant was interrupted (AS versus QS). A total of 44 babies were included (n=34 in the AS group, n=10 in the QS group). Although the feeding duration was higher in the group woken from QS (median: 28.0; IQR: 15.8 to 40.8) than the group woken from AS (median: 22.5; IQR: 14.0 to 26.3), the difference between groups was not statistically significant (p=0.102).
Discussion
All MLP infants in this study displayed periods of AS, QS and W with SWC seen on all recordings.25,26 Interruption of overnight sleep was primarily for feeding purposes (both oral and NGT feeds) and equates to interruption of 23.3% of all overnight SWC. It is not unreasonable to assume an increase in this percentage of interruptions may occur during daytime hours when routine procedures and examinations are carried out. In a study carried out by Levy et al,27 vEEG monitoring of clinically stable near-term and term infants in the NICU (n=25) showed that provider contact occurred for 27%
(65 minutes) of the four hours of recording time and only 50% of infants engaged in a full SWC prior to interruption for care. Similar to our study, the majority of infant contact/disturbances occurred during AS, a state which has a greater association with the growth and development of complex neural networks.28,29
MLP infants frequently display disorganised feeding behaviours with difficulties evident in ability to coordinate ‘suck, swallow and breathe’ when feeding.30 This factor is reflected in this study as 21.2% of feeds were given via NGT (n=76). Feeding ability may be further diluted by inadequate sleep in the NICU impacting clinical condition, growth and development, neurobehaviour and the establishment of oral feeding.30,31 Sleep disturbances for routine care in the NICU affects brain maturation,27 hence in the absence of clinical need, disturbing sleep for routine care when the infant is not actively feeding warrants further research.
In the absence of specific direction, the mode, frequency and schedule of feeds and sleep interruptions are very much guided by the bedside nurse and relate to feeding volumes taken/tolerated. Longer feed duration, as reported here when sleep is interrupted, has a knock-on effect on human resources, duration of stay, cost to the healthcare provider and warrants further consideration. Allowing a growing preterm to wake spontaneously for feeding will ensure little interruption to the natural course of a SWC, which may positively impact neurodevelopmental outcome. However, further research is warranted in relation to the impact of this practice on nursing resources, parental visiting and overall health and wellbeing of the infant.
A healthy in utero environment provides optimal conditions for normal central nervous system development.32 Preterm birth brings with it a sudden change in the quality and intensity of sensory information received, which may lead to disrupted and fragmented sleep, impacting sleep organisation and developmental outcome.27,33 Prolonged and continuous exposure to the multisensory environment and stress-related events of the neonatal unit and/or sleep interruptions may impact not only the physiological status but the long-term neurodevelopmental outcome of the preterm infant, including long-term sensory processing disorders.12,29,34-38 Preterm birth is associated with significant morbidity29,39 including long-term consequences, such as difficulties with cognition, language development, motor skills, behaviour and overall physiological wellbeing.8,29,37,40 A priority to creating a culture of ‘sleep protection’ requires knowledge about SWC and recognition of sleep states, which will assist in identifying the appropriate timing of handling for infant cares.6,13,25,41 Despite being closest to the point of care of the preterm infant in the NICU, a low level of knowledge of behavioural features and sleep state identification has been found among neonatal nurses and this may lead to misinterpretation of sleep activity (ie active sleep) for wakening.42
Strengths of this study include the number of participants, similar clinical status, duration and timing of overnight vEEG and the use of video-supported visual observation with respiratory monitoring supporting sleep state identification, ie rapid irregular respirations in AS (REM) with slower regular breathing in QS (NREM).2 A limitation of this study is its focus on overnight sleep only. Further research should incorporate a full 24-hour monitoring period, providing insight into both day and night SWC and interruptions observed. The prognostic value of EEG in uncomplicated medically stable MLP infants remains unclear.13,43 Hence the significance of outcome to the number of SWC seen on EEG. The duration of each sleep state has yet to be determined and will constitute part of a future study.
In conclusion
EEG provides detailed real-time information about brain activity of preterm infants and the changes that occur during sleep wake cycling. Sleep disturbances may affect the development and organisation of sleep-wake patterns of the preterm infant and impact sleep state organisation and potentially long- and short-term developmental outcomes.
Preterm infants are at risk of adverse neurological development especially during the critical phase of brain development that occurs during the MLP period. Preserving and supporting optimal sleep organisation among infants will support a normal neural pathway of development and help improve long- and short-term outcomes. This study has provided an introduction to preterm infant states as seen in vEEG, providing a window through which we can view brain activity during each sleep state.
This study has quantified overnight SWC and interruptions. With minimal exception, overnight disruptions to sleep were found to be a consequence of routine care, accounting for disturbance to 23.3% of the total SWC recorded. Reducing this number and preserving sleep provides an opportunity to enhance brain development but presents a real operational challenge in the NICU.
Acknowledgements
This work was supported by the INFANT Research Centre Ireland and a Science Foundation Ireland research centre award (12/RC/2272). The authors are extremely grateful to the parents of the infants who participated in this study. Further thanks are offered to staff in the neonatal unit at CUMH for their support with this study.
Or read this article in our
Tablet/iPad edition
- Disturbances of nocturnal sleep in preterm infants were frequent in the NICU, predominantly for feeding.
- Infants who woke spontaneously, fed more efficiently within a shorter time-frame compared to infants who were disturbed from their sleep for feeding.
- Optimising sleep in the NICU will support the normal trajectory of development.
Also published in Infant:
