

Home oxygen in neonatal chronic lung disease
Home oxygen therapy is used to optimise growth and development in infants with chronic lung disease of prematurity. However, the treatment also carries a significant burden to the patient and family. Current guidelines are mainly based on expert consensus due to the lack of a strong evidence base, and local practices vary. We surveyed neonatal units across England and Wales to understand current practice and areas for optimisation of care.
Alison J Garde1MBBS, MA(Cantab), MRCPCH
ST5 Paediatric Registrar
Jayesh M Bhatt2
MBBS, MD, DCH, FRCPCH
Consultant Respiratory Paediatrician
Tatiana Rjabova1
MD, MRCPCH
Consultant Paediatrician with Special Interest in Neonatology
Hazel J Evans3
MD, MRCPCH, MB BCh
Consultant Respiratory Paediatrician
hazel.evans@uhs.nhs.uk
1Department of Paediatrics, Royal United Hospital, Bath
2Department of Respiratory Paediatrics, Nottingham Children’s Hospital
3Department of Respiratory Paediatrics, Southampton Children’s Hospital
Chronic lung disease of prematurity (CLDP) is the most common diagnosis for which long-term oxygen therapy (LTOT) is prescribed in children.1 This minimises periods of hypoxia in infants with CLDP, thus optimising growth and development, but is associated with a relatively high treatment burden.2
Recent guidance produced by the American Thoracic Society (ATS)3 acknowledged a striking lack of evidence regarding optimal initiation, monitoring and weaning of LTOT, and a lack of progress in the ten years since publication of the most recent British Thoracic Society (BTS) guidelines in 2009.1,3,4 This was also highlighted in the 2020 position statement published by the Thoracic Society of Australia and New Zealand on Respiratory management of infants with chronic neonatal lung disease beyond the neonatal intensive care unit (NICU), which reflected on the “Considerable variation and little objective evidence to guide the use of long-term supplemental oxygen therapy in infants with [chronic neonatal lung disease].”5
Anecdotally within the UK, the lack of a strong evidence base has resulted in wide variation in practice between centres. There is also considerable variation in the interpretation of paediatric oximetry recordings by clinicians when presented with the same dataset.6 This service evaluation aimed to understand current practice in use of LTOT for CLDP across England and Wales, to identify areas for optimisation of current care and areas requiring further research.
Methods
A ten question survey (TABLE 1) was distributed in November and December 2019 using an online survey platform via regional neonatal networks, and via British Paediatric Respiratory Society (BPRS), Paediatric Pan London Oxygen Group (PPLOG) and British Association of Perinatal Medicine (BAPM) newsletters. A covering letter explained the purpose of the survey. Participation in the survey implied consent to inclusion in this study. Respondents were asked to specify the centre they worked in. Where responses from the same centre were identified, only one respondent’s set of answers was used. The answer set with the most complete answers was used. Responses that did not recognise appropriate units or clearly defined parameters were excluded; for example, oxygen desaturation index (ODI) threshold for weaning described in percentage terms rather than an absolute number. Where centres reported using 2009 BTS guidance, results were reviewed to determine whether reported practice was in line with BTS recommendations.
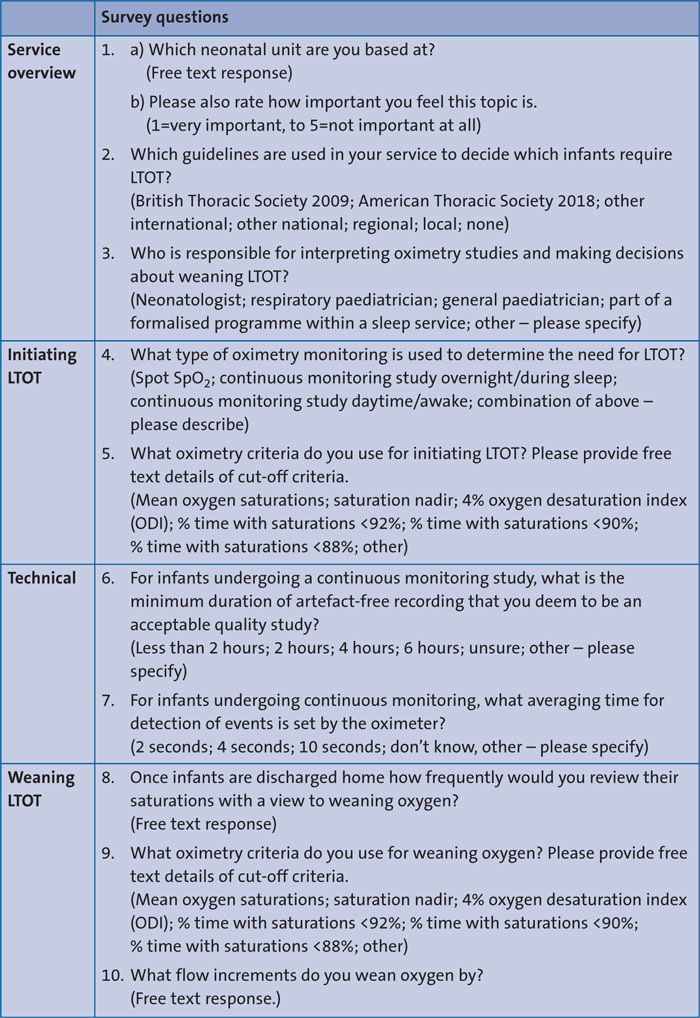
TABLE 1 The ten-question national survey on current practice around LTOT in infants with CLDP. Questions are shown subdivided by topic. Where questions were presented in a multiple choice format, answer options provided are listed in brackets; where a question required a free text response this is indicated. In the covering letter, respondents were asked to specify the thresholds they would use to decide whether an infant did/did not have an oxygen requirement (denoted as ‘cut-off criteria’). For each oximetry criterion, a free text box was provided to specify the threshold value used. Key: SpO2 = blood oxygen saturation level; ODI = oxygen desaturation index; BTS = British Thoracic Society; ATS = American Thoracic Society. ‘Spot’ saturations = one-off SpO2 check, rather than a period of continuous oximetry trace.
Results
In total, 49 responses were obtained. Five duplicate responses were identified and excluded, leaving 44 for analysis. Responses were obtained from neonatal teams from a range of rural and urban locations across England and Wales (level 3 units n=13, level 2 units n=16, level 1 units n=6, community neonatal teams n=3). Six respondents did not identify their place of work.
Service overview
Respondents were asked to specify which guideline or guidelines were used in their centre for LTOT in CLDP. The most common guidance used was the 2009 BTS guidance (45% of centres); no other national or international guidelines were used. Eleven per cent of centres used a regional guideline, 32% a local guideline, and 14% of centres reported using no guideline at all.
Decisions around initiation and weaning of LTOT were made predominantly by neonatologists (66% centres) and general paediatricians (30% of units). Respondents could select more than one option; they did so in more than half of cases, reflecting a team-based approach. The ‘other’ category (34% of centres) denoted mainly specialist nurses (26% of centres) from neonatology or respiratory teams. In only 9% of centres, decisions were made as part of a formal sleep medicine service.
Initiating LTOT
The vast majority of units (38 of 44, 86%) reported using an overnight continuous oxygen saturation trace to determine the need for LTOT. This was used on its own by 27 out of 44 centres (61%). In 11 out of 44 centres (25%) it was used in combination with either ‘spot’ oxygen saturations or daytime continuous oximetry measurements.
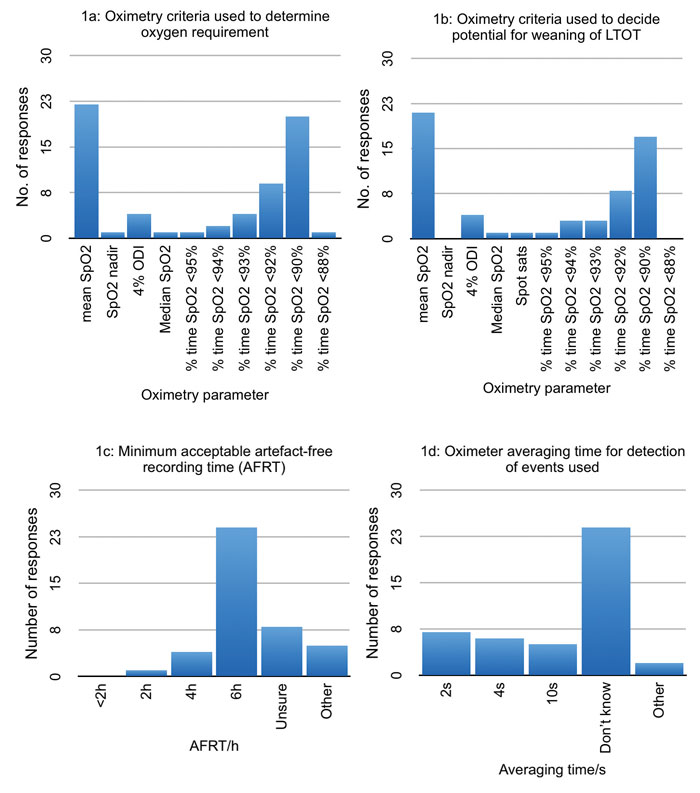
FIGURE 1A-D Bar charts showing criteria for oxygen initiation and weaning (1a, 1b) alongside technological considerations when interpreting oxygen saturation data (1c, 1d).
There was wide variation in the oximetry criteria used to determine the need to initiate LTOT in CLDP (FIGURE 1A). The commonest criteria used were mean SpO2 (50% of centres) and percentage of time with SpO2 <90% (45% of centres). Notably, centres using the same oximetry criteria to determine oxygen dependency used different cut-off thresholds: mean SpO2 threshold values ranged from 92%-97% (mode 95%). Similarly, where percentage time with SpO2 <90% was used, threshold ranged from 4% to 20% (mode 5%).This variability remained even where centres reported basing practice on the BTS guidance (n=20). In these centres, mean SpO2 thresholds ranged from 92-97% (relative to a BTS guideline recommendation of ≥93%). Threshold time with SpO2 <90% ranged from 5-10% (relative to a BTS guideline recommendation of SpO2 <90% at ≤5%) and was not reported as a criterion used in nearly 50% of these centres (9/20).
Technical aspects of oximetry
Minimum artefact-free recording time (AFRT) deemed to constitute an acceptable quality oximetry study varied widely between centres, from 2-12 hours (FIGURE 1C). Averaging time set by the oximeter was widely variable (range 2-10 seconds). Notably, 55% of respondents’ answers to the question on averaging time were ‘Don’t know’ (FIGURE 1D).
Weaning of LTOT
As might be expected, within a given centre very similar oximetry criteria and threshold values were used to determine suitability for weaning as used for initiation of LTOT (FIGURE 1B). Oxygen flow rate was weaned in decrements of 0.01L/min – 0.5L/min, depending on the centre. Where a range of decrements was used (36% of centres) these ranges were also very variable, with the maximum decrement used in some centres (0.03L/min) smaller than the minimum decrement (0.1L/min) used in other centres.
Discussion
This service evaluation demonstrates a wide variation in practice in initiation, monitoring and weaning of LTOT for infants with CLDP across England and Wales.
While most units used an overnight oximetry trace to determine the need for LTOT, the survey results demonstrate that there is wide variation in the specifics of practice around oximetry for LTOT for CLDP. Different oximetry parameters were used in different centres, and thresholds for starting or weaning oxygen varied. The most frequently reported guideline on which practice was based was that published by the BTS in 2009.1 However, centres reporting using this guidance often used different oximetry thresholds than the ones recommended by it.
Over 50% of respondents acknowledged a lack of awareness of oximeter averaging times, and we noted highly variable minimum AFRT durations deemed as ‘acceptable’. These technological considerations have been shown to affect outcome variables such as mean SpO2 or 4% ODI.7 For example, where longer oximeter averaging times are used, short-lived desaturation episodes may not be detected. This is particularly important in young infants who are susceptible to short central apnoeas resulting in brief desaturations. Additionally, longer averaging times that blunt the effect of desaturations artificially lower mean saturations, which will impact on weaning infants from oxygen when targeting specific thresholds.8-10
Finally, the variation noted in both thresholds used to determine suitability for weaning LTOT, and in size of decrements used to wean oxygen flow rate, will result in infants being treated with LTOT for longer by some centres than others.
Overall, the wide variation in practice seen in the survey results implies that some infants are being treated with LTOT for longer or shorter than is optimal for the balance of treatment benefit and burden.
Responses were voluntary and were achieved from around 25% of neonatal units in England and Wales. While we recognise that this relatively low response rate may limit the generalisability of our findings, responding units did represent the full spread of units, from tertiary NICUs to community neonatal teams; varied settings from large city to rural; and a wide geographical spread across England and Wales.
It is likely that units who believed the topic to be of value were more likely to submit information, which may skew the results. In fact, the overwhelming majority of survey respondents who rated the importance of the survey topic (n=29) rated it as ‘very important’ (24 out of 29). We therefore suspect the practice described most likely represents a best-case scenario for LTOT management of these infants. This underlines the variability in practice of even highly motivated teams.
Conclusions
This national survey demonstrated wide heterogeneity in the implementation, monitoring and weaning of LTOT for infants with CLDP. This most likely relates to a relative lack of an evidence base regarding SpO2 reference ranges and the impact of intermittent hypoxia in young infants, alongside limited understanding of key factors affecting data output. This topic, and achieving consensus in manage-ment, is seen as an area of high importance by clinicians caring for these infants. More research is needed to establish evidence-based criteria and thresholds for LTOT initiation and weaning in infants with CLDP using modern oximeters, in order to optimally balance promotion of infant growth and development with minimisation of treatment cost and burden. Research outcomes should be widely disseminated alongside oximetry education programmes.
Acknowledgements
The authors would like to thank BPRS, BAPM, PPLOG and the regional neonatal networks who circulated the survey, and all those who took the time to complete it.
Or read this article in our
Tablet/iPad edition
- Thresholds guiding decisions around initiating and weaning long-term oxygen therapy for infants with CLDP vary widely across England and Wales.
- Technical considerations affecting data output from pulse oximeters are poorly understood resulting in a wide variation in pulse oximeter settings across home oxygen services.
- Evidence-based guidance is required alongside education to inform clinicians on best practice for infants with CLDP requiring supplemental oxygen.
