

Changing referral patterns, reduced feeding-related problems and changes in breastfeeding during COVID-19
Due to the current global pandemic, the maternity services at Jessop Wing, Sheffield Teaching Hospitals NHS Foundation Trust, have had to place restrictions on visitors to the hospital environment. During this time, we have seen a significant decrease in the number of term babies referred with common feeding-related problems, while also noting an increase in breastfeeding rates at discharge. We explore the possible reasons for this and what lessons may be learned.
Anne E Bean
MBChB, MRCPCH, PGDip, PGCert
Neonatal Registrar and Leadership Fellow
anne.bean1@nhs.net
Caryl Skene
BSc(Hons), MSc, DMed Sci, RN, RM
Lead Nurse for Clinical Excellence
Eleanor Peirce
MBChB, MRCPCH, PGDip, PGCert
Neonatal Registrar
Simon J Clark
BM, MSc, MRCP, FRCPCH, MD
Consultant Neonatologist
Jessop Wing, Sheffield Teaching Hospitals NHS Foundation Trust
The novel coronavirus SARS-CoV-2, causing the disease COVID-19, has been declared a pandemic by the World Health Organization (WHO). It has impacted significantly on the way both maternity and neonatal services currently operate in the UK and globally. To date, there have been over eight million confirmed cases of COVID-19 worldwide.1
This pandemic has had far reaching and too often tragic consequences. However, in our single centre experience, we have found some other less expected outcomes of the pandemic.
Local adaptations to maternity and newborn care services
There have been several changes implemented in the maternity unit aimed at reducing the number of people circulating within the hospital environment in an effort to reduce the risk of infection with and transmission of SARS-CoV-2. Since March 2020, in line with public health and professional guidance,2,3 there have been restrictions in place on all maternity wards, both antenatal and postnatal, meaning visitors are only able to come to the wards in exceptional circumstances. Parents are not considered to be visitors on the neonatal unit; however, as advised by the British Association of Perinatal Medicine (BAPM),3 a proportionate restriction has been put in place, so that only individual parents should attend the unit at any one time, other than in exceptional circumstances.
During labour, birthing partners can be present; however, after the baby is born birthing partners must then leave the hospital. While this has been a challenging time for both staff and parents, it has also facilitated a greater amount of uninterrupted time for women to spend with their babies, both in the maternity unit and when they go home.
It has been recommended to pregnant women that breastfeeding is safe and remains the recommended method of feeding during the pandemic. This has been agreed by the Royal College of Obstetricians and Gynaecologists (RCOG), United Nations International Emergency Fund (Unicef) and the WHO.3-5 This is also supported by the current lack of evidence that COVID-19 infection can be passed through breast milk6 and the wealth of evidence that breastfeeding reduces the risk of babies developing infectious diseases.
The Rapid Access Clinic
The Rapid Access Clinic (RAC) at the Jessop Wing was first developed in 2011. It is an Advanced Neonatal Nurse Practitioner-led service designed to reduce the number of hospital readmissions while aiming to address the increasing desire for early postnatal discharge.7 The service runs on a daily basis and offers a telephone consultation service and the ability to then have an appointment for babies to be assessed with their mothers and receive support from a member of the specialist infant feeding team, if required. Babies are referred by the community midwifery team following their routine reviews. Weighing of babies continues during this time on day 3 and 5 after discharge. The babies who are seen in clinic are most commonly referred with jaundice, feeding difficulties, weight loss or a combination of these problems. A small number of babies are seen for other reasons. Babies can be referred for weight loss up to 10 days of age and jaundice up to seven days. After this time, or if acutely unwell, they would be seen in the local children’s hospital.
Methods
Data are collected for audit purposes for all referrals and attendances at the RAC. This includes information on the following:
- reason for referral
- mode of feeding
- birth weight
- current weight
- degree of weight loss
- outcome of referral.
We reviewed the data collected during March and April 2020 and compared this with data collected in the same time frame in 2019. Subsequently we made contact with colleagues at the local children’s hospital to ensure that patients were not presenting later with the problems. We also discussed with midwifery colleagues to collect qualitative reports as to why they felt there had been a change in referral patterns.
Results
During the period of March and April 2020 there was a marked reduction in the number of referrals to the RAC and subsequently babies seen in the clinic (FIGURE 1). When these data were further evaluated, we found that this downward trend was particularly notable in both jaundice and weight loss referrals.
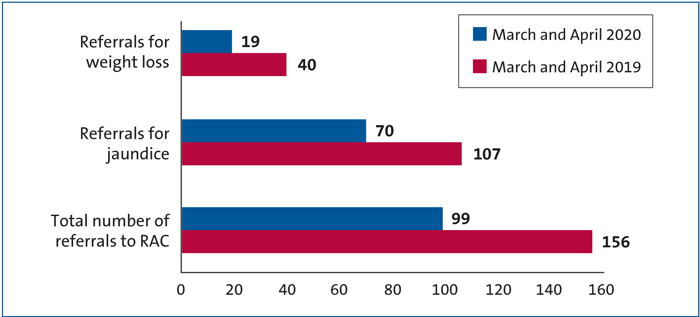
FIGURE 1 The number of babies seen in the RAC at the Jessop Wing in March and April 2019 compared with 2020.
Importantly, there was no increase in neonatal admissions to the local children’s hospital with jaundice, weight loss or breastfeeding-related problems.
The March and April RAC referrals for 2019 and 2020 were each combined; 2019 showed 156 referrals from 889 discharges (17.5%) compared with 2020 results of 99 from 917 discharges (10.8%). Fisher’s exact test was then used to assess statistical significance, which showed this to be significant (p=0.0001).
Similar comparisons were performed with referrals for jaundice, with 107 referrals from 889 discharges in 2019 (12%) compared with 70 referrals from 917 discharges in 2020 (7.6%). Statistical significance was shown (p=0.002).
A weight loss comparison was also performed. In 2019 there were 40 referrals from 889 discharges (4.4%) and in 2020, 19 referrals from 917 discharges (2.1%). Once more, this was statistically significant (p=0.005).
Breastfeeding rates
We reviewed breastfeeding rates on the postnatal ward at discharge for all women. When March and April 2020 rates were compared to the same period in 2019, an increase was noted (FIGURE 2).
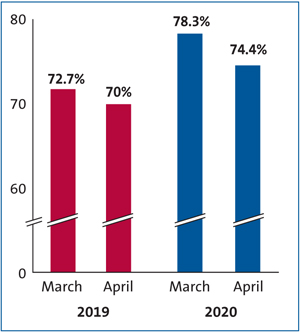
FIGURE 2 A comparison of percentage of women breastfeeding at discharge from the postnatal ward between March and April 2019 and 2020.
The March and April breastfeeding rates were then combined for 2019 showing 635 women breastfeeding at discharge out of a total of 889 (71.4%) women discharged from the postnatal ward. In March and April 2020, a total of 701 out of 917 women were breastfeeding at discharge from the postnatal ward (76.4%). Fisher’s exact test was used to assess statistical significance, which showed this to be significant (p=0.0158).
Midwifery colleagues in the community and in the hospital setting were then asked why they felt these changes had occurred. Overall, it was commonly suggested that the changes may be due to women feeling more able to devote prolonged periods of time to breastfeeding as the number of visitors they receive has, in most cases, dramatically reduced. Some of these comments are summarised in FIGURE 3.
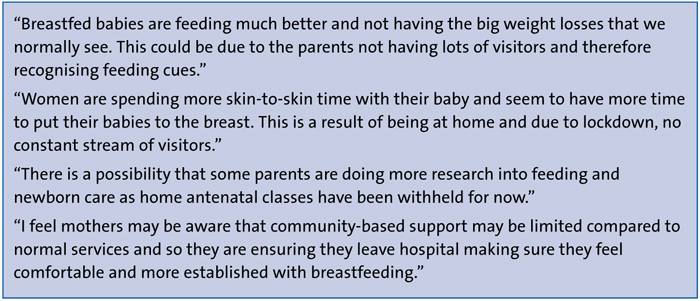
FIGURE 3 Some opinions of community and hospital midwives.
Discussion
Our data suggest that successful breastfeeding may have increased during lockdown.
It is possible that women may have tried to avoid being sent to the RAC due to concerns about the transmission of COVID-19 in the hospital environment. However, there has not been an increase in local admissions with worsening weight loss or jaundice in the short term.
There are several factors that may have played a role in increased breastfeeding. Women may have been more aware of the benefits of breastfeeding. They may have read or been informed that breastfeeding may help support immunity from COVID-19, and this may have affected maternal decision regarding feeding choice. As suggested by one of the midwifery team, women may be concerned regarding lack of ‘drop-in’ support in the community and may have ensured they felt more confident regarding feeding prior to being discharged.
Due to the hospital visiting policy, women have undoubtedly had less interruption by visitors while on the postnatal ward. Furthermore, as a result of Public Health England advice restricting movement and encouraging social distancing at this time, it is likely that this will have continued within the home environment. As a result, some women may have been able to spend a larger amount of time with their closest family circle, which could offer more time and space to establish breastfeeding. With less conflicting advice or judgment from family members, mothers may feel more relaxed and less embarrassed while feeding.
Clearly there are also disadvantages of reduced visiting. Some women may have experienced less family support, such as not having partners or their own mothers present who may usually help in the immediate peripartum period. However, the increased presence of partners at home, in some cases through furlough or work-from-home arrangements may have increased support for women.
It is also important to note that several aspects of breastfeeding support that would usually be in place locally are not, for example breastfeeding peer support in the community. This could have affected some women’s feeding journey.
There may of course be other influencing factors on referrals and breastfeeding rates that have not yet been explored. More research would be highly valuable to understand this phenomenon further and to explore women’s experiences of feeding their infant in these unusual times. It would be particularly important to know how long breastfeeding is being sustained and whether or not this continues in the longer term. Ultimately, if contributing factors to increased successful breastfeeding rates could be understood in more depth, there is a greater chance of it being sustained in the future.
Conclusions
In our maternity unit we have demon-strated that during March and April 2020, there was an increase in women breast-feeding at discharge from hospital. Referrals to our RAC for jaundice and weight loss dropped significantly.
Informal discussions with the midwifery team suggest that this may be due to women having more uninterrupted time with their babies.
These findings suggest that providing women with the time and space to spend time with their new baby, while being supported by their close support circle, facilitates the establishment of successful breastfeeding, while also reducing early referrals back to hospital with feeding-related problems.
Acknowledgement
The authors would like to thank the midwifery team at the Jessop Wing for providing their comments, in particular Consultant Midwife Helen Baston and Head of Midwifery Paula Schofield.
Or read this article in our
Tablet/iPad edition
- Providing women with the time and space to be with their new baby, while being supported by their close support circle, facilitates the establishment of successful breastfeeding.
- A reduction in referrals to our Rapid Access Clinic, particularly for jaundice and weight loss, may be attributable to increases in successful breastfeeding.
Also published in Infant:
