

Stoma associated morbidity in the preterm infant
Babies born prematurely are at risk of developing gastrointestinal complications that may require small bowel resection with or without stoma formation. The evidence base regarding the optimal initial surgical intervention and the subsequent timing of stoma closure is limited. To help inform the design of future randomised controlled trials investigating the optimal timing of stoma closure, we describe current practice and outcomes including stoma-related complications in a cohort of preterm infants who underwent stoma formation at the Royal Hospital for Children, Glasgow.
Claire Granger1
Neonatal Higher Specialist Trainee
claire.granger@nhs.net
Natalie Smee2
Neonatal Higher Specialist Trainee
Eilidh Duncan3
Senior House Officer
Timothy Bradnock2
Consultant Paediatric Surgeon
Judith Simpson2
Consultant Neonatologist
1Royal Victoria Infirmary, Newcastle
2Royal Hospital for Children, Glasgow
3NHS Greater Glasgow and Clyde
Work attributed to the NICU, Royal Hospital for Children, Glasgow
It is not uncommon for preterm infants to require emergency small bowel surgery for a variety of acquired gastrointestinal pathologies, including necrotising enterocolitis (NEC), spontaneous intestinal perforation (SIP), volvulus and obstruction.1 There is a relative dearth of evidence with which to guide management in this situation and decision making is often based on centre-specific surgical expertise and experience. As such practice varies not only in terms of the initial operation (primary anastomosis versus stoma formation), but also in the timing of subsequent stoma closure.2,3
In recognition of this uncertainty the National Institute for Health Research (NIHR) recently funded a feasibility study (Timing of Stoma Closure in Neonates; TOSCiN), which aims to explore current practice and use this to inform future study design. With this in mind, and in order to more closely examine management in our own centre, a regional surgical unit, we reviewed stoma-related complications and timing of closure in a cohort of preterm infants with acquired small bowel disease.
Methods
We retrospectively identified infants born at <32 weeks’ gestation who underwent stoma formation ± small bowel resection between January 2012 and December 2018 in the neonatal intensive care unit at the Royal Hospital for Children, Glasgow.
We recorded stoma, vascular access and parenteral nutrition (PN) related complications, enteral feed tolerance and timing of stoma closure. We compared infants who had an underlying diagnosis of NEC (Group 1) with the other combined diagnoses (Group 2). Approval for the review was obtained from our local Caldicott Guardian.
Results
Fifty-six babies were identified, 35 male and 21 female. Indications for stoma formation were:
- NEC (n=29)
- SIP (n=15)
- congenital bowel anomalies (n=4)
- meconium ileus (n=4)
- volvulus (n=3)
- milk curd obstruction (n=1).
We excluded eight from further analysis: four with congenital rather than acquired bowel pathology, two with co-existing complex genetic diagnoses and two who had incomplete clinical information available.
Of the remaining 48 infants, over half (56%) had an underlying diagnosis of NEC. Forty-seven had ileostomies created and one a jejunostomy.
The two groups were similar in gestational age, birth weight, age and weight at stoma closure, but those with NEC were older at stoma formation (TABLE 1). In both groups less than half were successfully established on full enteral feeds prior to stoma closure and almost three quarters required adjuvant PN at some point to achieve adequate growth (TABLE 1). The median duration of PN was shorter in those with NEC than those without (56 versus 92 days).
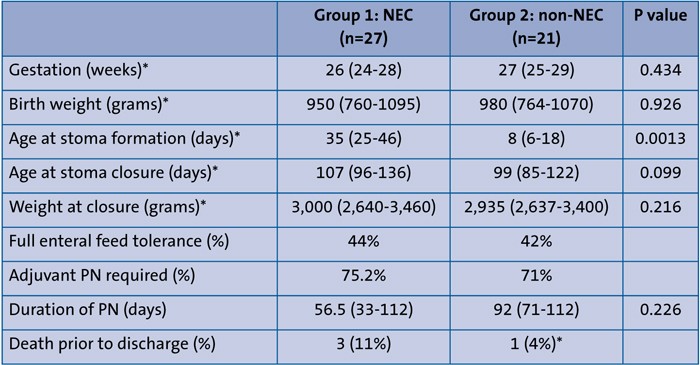
Table 1 Characteristics of NEC (Group 1 ) versus non-NEC stoma groups (Group 2). Data are median (IQR)
Stoma complications occurred in five (18%) of those with NEC and eight (38%) of those with non-NEC diagnoses. The most common problems were prolapsed stoma (n=4) and parastomal hernia (n=3). Complications related to the need for ongoing vascular access occurred in 16 (59%) of those with NEC and 19 (90%) of those without. The most common problems were infection (n=22) and extravasation (n=7).
Four babies died prior to discharge from the neonatal unit, three with an underlying diagnosis of NEC and one with SIP.
Discussion
A significant minority of preterm infants require gastrointestinal surgery, with a recent English network-based study identifying that over an eight-year period nearly one in six infants born at <26 weeks’ gestation required an emergency laparotomy.1
The extent and heterogeneity of the underlying disease processes combined with the clinical condition of the baby at the time of surgery will always make a direct comparison of the initial operation challenging (primary anastomosis versus stoma formation), and the operation performed will be at the discretion of the surgical team involved. This probably explains why it is difficult to draw any meaningful conclusions from the existing literature.2 Even attempts to combine studies and strengthen the data have had limited success. A systematic review and meta-analysis of 12 studies, none of which were randomised trials, compared outcomes for primary anastomosis versus stoma formation in NEC, concluding that mortality was less following primary anastomosis.2 However, the authors hypothesised that this was probably related to underlying disease severity influencing the choice of operation rather than the operation influencing the outcome. In cases of severe NEC the same study identified no significant difference in complication rate between primary anastomosis and stoma formation.
In our centre, stoma formation is the most commonly performed operation in a preterm infant requiring small bowel resection. In situations where there is uncertainty about the viability of extensive portions of the bowel or where the distribution of ischaemia is patchy or discontinuous, a ‘clip and drop’ procedure is usually performed with plans for a second-look laparotomy, with or without further bowel resection, stoma formation or primary anastomoses. However, even within our centre there is variable practice with regard to both the initial surgical approach and the timing of subsequent stoma closure, a situation that is replicated across most other tertiary neonatal surgical centres,1 again reflecting the limited evidence base to guide contemporary practice.
Once a stoma has been created, its closure is often viewed as an elective rather than a time critical procedure, although there can be exceptions including high small bowel stomas with large outputs that compromise fluid and electrolyte balance or growth. Even though surgeons refer to ‘early’ and ‘late’ stoma closure, there is no real consensus about how these are defined. Is it by corrected gestational age or weight at the time of closure or time from the original surgery? In a systematic review and meta-analysis of six studies comprising 280 infants with NEC, Zani et al described early as <8 weeks from stoma formation and late as ≥8 weeks. They identified no significant difference in duration of PN, total length of hospital stay or post-closure complication rates.3 Many surgeons, including those in our centre, adopt a weight-based approach to stoma closure. Interestingly although some of our surgeons state that they aim to close a stoma when the infant reaches a weight of approximately 2,500g, our data indicate that the median weight at stoma closure in this cohort, irrespective of underlying diagnosis, was around 3,000g.
The argument for delaying closure is to allow the infant to grow and recover from comorbidities such as lung disease before they undergo further surgery, but these have to be balanced against the complications of having a stoma. In a single centre review of 58 infants with stomas, complications were described in 41%; low birth weight infants and preterm infants were more likely to remain PN-dependent prior to closure with an increased incidence of PN-associated complications.4 In a systematic review of gastrointestinal sequelae after surgery for NEC, Hau et al identified a stoma complication rate ranging from 4% to 71%.5 Complications fall into two main categories: those directly related to the stoma itself (eg prolapse, retraction, parastomal hernia and skin problems) and those as a result of a requirement for prolonged PN. These in turn can be divided into PN-related complications (eg cholestasis and associated liver disease) or vascular access related (eg sepsis and extravasation injury).6 Our data reflect what previous authors have described, with between 75% and 80% of our cohort experiencing complications that fall broadly into one of these categories. FIGURES 1, 2 and 3 are representative images of some of these complications from our centre.

Figure 1 Widespread skin breakdown and full thickness wound dehiscence (liver in base).

Figure 2 Skin breakdown and superficial wound dehiscence.

Figure 3 Prolapsed stoma.
Weight gain in the presence of a stoma can be challenging and significant growth failure is not uncommon in this cohort of patients. The aetiology of this is multifactorial: reduced small bowel surface area, enterocyte damage with resultant malabsorption, high stoma output with associated fluid and essential salt loss, and in addition enteral feeds are often paused due to concerns about sepsis or poor feed tolerance. As a consequence of this, a significant proportion of infants receive long term PN. The likelihood of requiring adjuvant PN has been shown to be greater in low birth weight and premature infants and our data support these findings.4 In both our groups there was a requirement for adjuvant PN in over 70% of patients with a median duration of use of 56 days (NEC) and 92 days (non-NEC), respectively.
It should be acknowledged that the approach to feeding and growing babies with stomas may vary from centre to centre, with some like us, adopting strategies such as distal lumen re-feeding or tolerating higher stoma outputs if weight gain is preserved to reduce the need for PN. In this context it is important to recognise the limitations of single centre data and their applicability to a wider neonatal population.
Conclusions
Our data identify a significant complication rate, a high need for adjuvant PN and poor progression to full enteral feeds associated with stoma formation in the preterm population. This burden of stoma-associated morbidity should prompt further consideration of the primary operation of choice following small bowel resection and inform discussion regarding the optimal timing of stoma closure. In this context, the NIHR TOSCiN feasibility study of stoma closure is timely.
Parental consent and acknowledgement
The authors obtained written consent from the children’s parents for publication of the images contained in this article. We are grateful to Margaret Reeves (Specialist Nurse) for providing the images.
Or read this article in our
Tablet/iPad edition
- Optimal timing of stoma closure in preterm infants is unknown.
- Complications following stoma formation are common and associated with significant morbidity.
- Complications can be related to poor growth, vascular access or the stoma itself.
Also published in Infant:
