

Bone health of extremely preterm infants: screening, monitoring and management of metabolic bone disease of prematurity
In this review article we summarise the pathogenesis of metabolic bone disease (MBD, also called osteopenia of prematurity). We consider the screening tools and the recommendations of professional bodies on management of MBD. We also present two case studies of long bone fractures in extremely premature infants following MBD. Based on the literature and our two cases, we propose a screening, monitoring and management algorithm for MBD of prematurity.
Asma Yasmeen
Neonatal Consultant, Victoria Hospital, Kirkcaldy
Previously Princess Royal Maternity, Glasgow
asmayasmeen@nhs.net
Allan Jackson
Consultant Neonatologist and ScotSTAR Lead (Neonatal) for Scotland
Princess Royal Maternity, Glasgow and ScotSTAR
Work attributed to Neonatal Unit, Princess Royal Maternity, Glasgow
Extremely preterm infants are at significant risk of MBD of prematurity. The aetiology is multifactorial including:
- failure of calcium and phosphorus accretion during the third trimester
- prolonged parenteral nutrition
- intestinal immaturity leading to poor absorption
- prolonged immobilisation
- some medications that alter the level of bone minerals in the body.
The condition is silent and leads to poor bone mineralisation until severe osteopenia occurs. Other features are poor growth, rickets and pathological fractures. The best strategy is to aim for prevention of symptomatic disease but there is lack of consensus on the choice of screening tests and thresholds to follow due to gaps in evidence-based research. Screening and monitoring are performed using various biochemical tests and radiological studies. X-ray findings usually come late and signify advanced MBD. Fortification of human milk, phosphate and vitamin D supplements are the mainstay of prevention of symptomatic disease. Treatment of pathological fractures requires multidisciplinary team involvement including orthopaedic and endocrine specialties. There is a need for nationally agreed guidelines on screening, monitoring and management of MBD to promote bone health and prevent complications in infants at high risk. Also, further research is required to establish investigations to diagnose early MBD to enable clinicians to commence prompt treatment to prevent complications.
A review of the literature: definition and prevalence
There is no consensus on the definition of MBD. It is characterised by reduced mineralisation of bones in preterm infants. In more severe cases, it can lead to radiological features of rickets, which can be seen in 10-20% of extremely low birth weight (ELBW, <1,000g) infants. In its most severe form it can lead to poor growth, poor lung function and pathological fractures.1 The exact prevalence is unknown due to the silent nature of the condition in most cases. It is estimated to affect 23-60% of very low birth weight (VLBW, <1,500g) and ELBW infants.2
Pathogenesis
Antenatal conditions that are associated with placental insufficiency (eg pre-eclampsia, intrauterine growth restriction and chorioamnionitis) lead to an increased risk of MBD, likely due to decreased phosphate transport to the fetal circulation.3
Most bony development occurs during the third trimester in utero making prematurity an important risk factor. Calcium and phosphorus are the main minerals involved and are transferred from mother to fetus (FIGURE 1). After preterm birth, changes occur in mineral homeostasis (FIGURE 2). Calcium transport is mainly regulated by parathyroid hormone-related peptide (PTHrP) and also by parathyroid hormone (PTH) and vitamin D (active form 1,25-dihydroxyvitamin D [1,25(OH)2D]). The mechanism of transport of phosphorus is not very well known but PTH has a role in the process.4
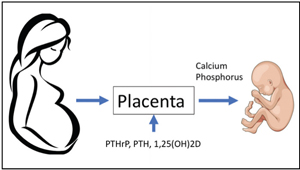
FIGURE 1 Fetal accretion of bone minerals. Key: PTHrP= parathyroid hormone-related peptide; PTH=parathyroid hormone; 1,25(OH)2D= 1,25-dihydroxyvitamin D.
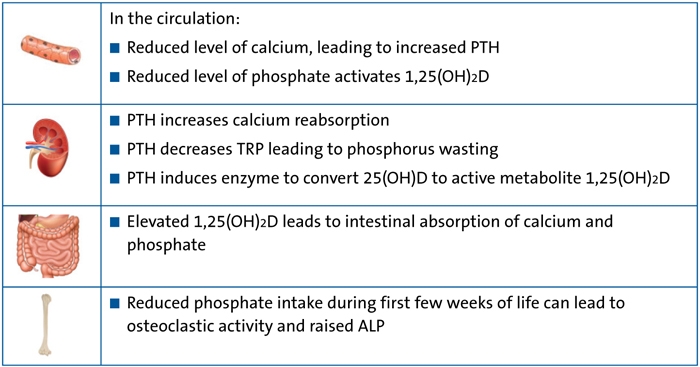
FIGURE 2 Bone minerals and homeostasis after birth. Key: PTH=parathyroid hormone; 1,25(OH)2D=1,25-dihydroxyvitamin D; TRP=tubular reabsorption of phosphate; 25(OH)D=25-hydroxyvitamin D; ALP= alkaline phosphatase.
Even with fortification of breast milk and use of preterm formula, intestinal immaturity can play a role in suboptimal absorption of calcium and phosphorus. Also, certain medications such as corticosteroids, methylxanthines (caffeine) and diuretics (especially loop diuretics) can further contribute to the risk of MBD.1
Screening and monitoring of MBD
Primary screening
Routine screening and monitoring includes checking levels of calcium, phosphorus and alkaline phosphatase (ALP). The calcium level (corrected for albumin) is considered normal if between 2.12-2.62 mmol/L. PTH acts on bone to increase osteoclastic activity, which leads to bone resorption and release of calcium thus maintaining calcium level within the normal range. A low value could be due to either low intake or increased losses. High levels are likely to be due to over treatment.5
For phosphorus, the aim is to keep the level at 1.8mmol/L or above. Low values are indicative of MBD.6,7
High ALP (hyperphosphatasia) in preterm neonates is usually indicative of MBD. ALP levels are the sum of bone, liver and intestinal isoforms, with the bone isoform contributing about 90% of the total. It is considered a marker of bone mineralisation.2 The ALP level in preterm infants increases after birth over the first few weeks and plateaus at around 5-6 weeks. If the ALP level is high after six weeks, it shows inadequate intake of calcium and phosphate and is highly indicative of MBD. However, the degree of osteopenia or rachitic changes does not correlate very well with ALP levels. Rachitic changes are more commonly associated with greater ALP levels (>800IU/L) but can also be seen at lower levels (<600IU/L).8 ALP levels may be deceivingly low in the setting of glucocorticoid exposure and should not be the only factor used in screening for MBD.9 Likewise, low levels of ALP may be due to a zinc deficiency, however in rickets, the ALP level is raised alongside the serum zinc concentration because of high bone turnover and zinc release.10
ALP can be elevated due to other reasons too, eg liver disease. In cases of any uncer-tainty, bone specific ALP can be requested.
Secondary screening
PTH and 1,25(OH)2D are measured when calcium, phosphorus or ALP levels are deranged. PTH is raised in subclinical hypocalcaemia. There is no reference range for preterm infants. The normal adult reference range is 50-88pg/mL. A level of >100pg/mL is taken as significantly high.11,12
The role of vitamin D in screening of MBD is not clear. 1,25(OH)2D can be normal in cases of MBD and rickets in preterm infants. There is emphasis on vitamin D supplementation. Vitamin deficiency can occur in cases of maternal vitamin D deficiency, short gut syndrome, malabsorptive disorders and anti-convulsant therapies (eg phenobarbital) and can lead to MBD. These patients require monitoring of their vitamin D levels.13
Rustico et al consider 1,25(OH)2D to be insufficient when <30ng/mL and deficient when <20ng/mL.9 Different thresholds are followed by different institutions and there is no consensus.
It is interesting to note that serum 1,25(OH)2D levels have been shown to be in the same range in preterm infants with rachitic changes and those without any rachitic changes. Hypervitaminosis can occur in infants on vitamin D supplementation and levels can be checked for monitoring purposes. Further studies to assess weight-based dosing are required.14
A study performed in 2007 on British adults aged 45 years showed that the prevalence of low vitamin D was alarmingly high during winter and spring, and much worse in Scotland compared to the rest of the UK.15 The results from Scottish health surveys conducted in 2010 and 2011 showed that 47% of the population living in the most deprived areas and 25% living in the least deprived areas have a suboptimal vitamin D level (<25nmol/L).16 This is why vitamin D levels are usually checked in extremely preterm infants in the UK who, despite having phosphorus prophylaxis, continue to have low phosphate and rising ALP levels. The threshold level of ALP varies across different neonatal units.
Tubular reabsorption of phosphate (TRP) is a measure of the fraction of filtered phosphate that is reabsorbed back into the circulation. The normal range is 78-91%. TRP is considered high if above 95%, which indicates insufficient phosphorus supplementation.3 A low TRP suggests urinary phosphate wasting, usually in infants with high PTH, resulting in low phosphate level. Paired urine and serum samples should be sent for testing.6
Urine calcium to creatinine spot ratio (urine Ca:Cr spot) is a screening test for hypercalciuria and a value of 3.8 (mmol/mmol) is considered significant. It could be due to excess calcium intake or side effects of certain medications, such as loop diuretics and methylxanthines.6
Imaging studies
X-rays of the long bones can show a range of changes (including osteopenia, rachitic changes, fraying and cupping of the metaphyses, and fractures) although these changes usually appear later. A long bone film of wrist or knee is performed in infants with suspected rickets. X-ray changes of rickets are only seen when bone mineralisation is reduced byby 20%.17 Osteopenia and rachitic changes are more common in infants with lower birth weight (ie <600-800g).8 If findings of rickets are evident, the American Academy of Paediatrics recommends repeating the film every 5-6 weeks until improvement is seen.1
A dual energy X-ray absorptiometry (DXA) scan is considered gold standard for determining the mineral density of the whole body in older children and adults but its utility in preterm infants as a screening tool is still restricted to research projects due to issues regarding availability, ionising radiations and artefacts.3,18
A screening algorithm
There is no consensus on a screening algorithm for premature infants. We recommend that all preterm infants should be tested using primary screening tests (calcium, phosphorus and ALP) every 1-2 weeks. If ALP is ≥450IU/L and trending up, along with a low phosphorus level (<1.8mmol/L), additional tests including PTH, vitamin D and TRP should be considered.
Prophylactic phosphorus supplementation should be commenced in all preterm infants who are at high risk of MBD (ie preterm <28 weeks’ gestation, birth weight <1,500g, required parenteral nutrition for 3-4 weeks, etc) once on full enteral feeds. Phosphorus can be added to parenteral nutrition too. The starting dose of oral phosphorus supplements is 0.5mmol/kg every 12 hours. The dose can be increased according to the requirement after serial weekly measurements.
If an infant requires calcium supplementation or is on calcitriol the aim is to normalise the PTH level and increase the TRP, thus reducing phosphorus wasting and normalise phosphorus. Monitoring of the vitamin D level as well as calcium, phosphorus, ALP and PTH will be required in this case. Measuring vitamin D levels is usually repeated after 12 weeks. We propose a screening algorithm based on a literature review and our two cases, as shown in FIGURE 3.
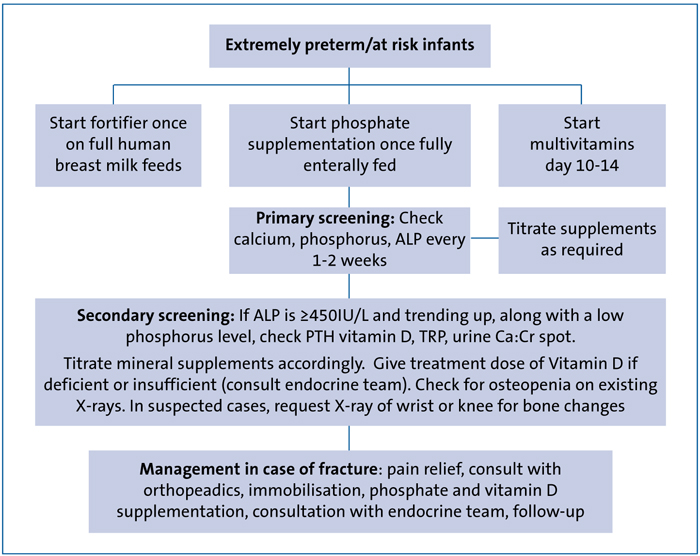
FIGURE 3 Screening, monitoring and management algorithm for MBD of prematurity.
Treatment of MBD
The aim of prevention and treatment is to maintain normal serum levels of calcium, phosphorus and ALP along with bone mineral accretion rates similar to that in utero.
Fortification of breast milk is essential for providing an adequate quantity of bone minerals. Unfortified human milk (either provided by the mother or a donor) only provides one third of the quantity of bone minerals that a fetus receives in utero.19 Banked donor breast milk may have a lower phosphorus content and care must be taken when unfortified breast milk is used.2
Many institutions routinely fortify donor breast milk. Some preterm infants will still develop MBD despite all measures and require a more personalised management of mineral intake.
All infants who are receiving calcium and/or phosphorus supplements or vitamin D at the time of discharge should be monitored with biomarker tests after discharge. TABLE 1 show the recommendations for vitamin D supplementation by different professional bodies.20
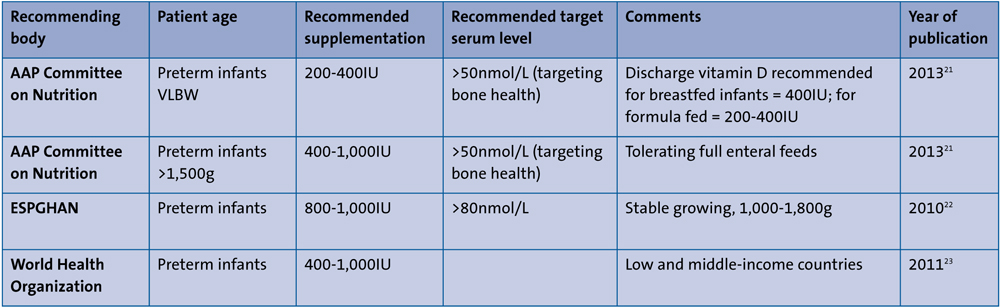
TABLE 1 Recommendations for vitamin D supplementation by different professional bodies.20 Key: AAP=American Academy of Paediatrics; ESPGHAN=European Society for Paediatric Gastroenterology, Hepatology and Nutrition.
Case studies
Case 1: A female infant born extremely premature with birth weight <1kg
The infant was fully enterally fed on day 7 of life. She received caffeine until almost 34 weeks’ corrected age, mostly at a dose of 10mg/kg. She did not require diuretics or postnatal steroids. At 37 weeks’ corrected age she was noted to have swelling and paucity of movements in the left thigh.
X-rays showed a proximal femoral metaphyseal fracture with a background of generalised osteopenia.
Case 2: A male infant born extremely premature with birth weight <1,100g
The infant had an initial rocky course due to sepsis. He was fully enterally fed at two weeks of age. He received caffeine until almost 34 weeks’ corrected age at a dose of 5mg/kg. He received topical (inhaled or nebulised) steroids from day 28 onwards for chronic lung disease. He did not receive any diuretics. He was found to be vitamin D deficient and received treatment. At 36 weeks’ corrected age he was noted to have swelling and paucity of movements in the left arm. X-rays showed a transverse displaced fracture of the distal humerus with a background of generalised osteopenia.
Both infants were fed on expressed breast milk until 34 weeks’ corrected age. The milk was fortified and oral phosphate supplementation commenced once they were fully enterally fed.
Management and outcomes
Orthopaedic surgeons and endocrinologists were involved in management of the infants, which comprised:
- immobilisation
- analgesia
- high-dose phosphate and vitamin D supplementation.
Both infants showed good healing of the fractures. Local reviews as well as Significant Case Incident enquiries were performed. Bone profile had been regularly monitored. The lowest phosphate levels for these infants were between 1.4-1.6mmol/L. X-rays showed evidence of osteopenia and signs of MBD. There was no evidence of trauma or use of excessive force. MBD/osteopenia of prematurity was concluded as the underlying cause of the fractures.
Conclusions
MBD remains a significant problem for extremely preterm neonates. Prevention of symptomatic disease is the goal to prevent complications such as rickets and pathological fractures. Neonatal units should have a screening policy for infants at risk of MBD. Screening includes monitoring of calcium, phosphorus and ALP and additional tests and radiological imaging, where required. Biochemical screening (both primary and secondary) is informative when results are analysed together as there are limitations of individual tests.
Further imaging modalities that can be routinely used for screening at the bed side are required. Development of local guidelines with multidisciplinary pathways can be helpful in management of advanced disease. Radiological evaluation is important in advanced cases and is a sign of late disease. Pathological fractures (rare) require multidisciplinary team management.
Early supplementation of phosphorus for prevention of MBD is important.
The 2013 American Academy of Paediatrics guidelines recommend daily vitamin D intake. There is need for a consensus across the UK over screening and management strategies to promote bone health in this vulnerable group.
Or read this article in our
Tablet/iPad edition
- Neonatal units should have a screening policy for infants at risk of MBD.
- Development of local guidelines with multidisciplinary pathways can be helpful in management of advanced disease.
- Development of consensus guidelines for screening and management in the UK are required.
Also published in Infant:
