

Waving goodbye to the baby train: reducing mother-infant separation and drug errors by collaborative working
This article describes a quality improvement initiative to decrease maternal and newborn separation and to reduce drug errors by stopping the ‘baby train’ of well infants attending the neonatal unit for administration of empirical intravenous antibiotics (IVABs). Utilising bite-sized teaching boxes, midwives were trained to act as a second checker of IVABs alongside a neonatal nurse, keeping mother and babies together on the postnatal ward. The initiative also saw an improvement in patient safety through greater understanding of antibiotic regimen and collaborative working between midwives and neonatal nurses.
Sarah Quinton-Shapcott
BSc Hons, PGDip with Merit in Advanced Clinical Practice
Advanced Neonatal Nurse Practitioner
sarah.shapcott@nhs.net
Shelley Knights
BScHons, MSc Advanced Clinical Practice
Advanced Neonatal Nurse Practitioner
Colchester Hospital Neonatal Unit, East Suffolk and North Essex NHS Foundation Trust
Background
Neonatal sepsis is a common cause of morbidity and mortality but due to its non-specific presentation, infants are often commenced on empirical antibiotics even if clinically well.1,2 The challenge facing many neonatal units (NNU) is deciding upon the most appropriate place to nurse these infants and where their antibiotics are administered.
In 2012, the National Institute for Health and Care Excellence (NICE) developed a guideline for the management of neonatal sepsis and delineated the assessment of risk factors and appropriate commencement on empirical antibiotics.3 However when considering the location of care, the guidelines are vague but suggest: ‘when deciding on the appropriate care setting for a baby, take into account the baby’s clinical needs and the competencies necessary to ensure safe and effective care’.
Some hospitals have a transitional care service but this facility and its definition varies greatly from hospital to hospital.4 Transitional care is not uniform and is often the ‘grey zone’ between the postnatal ward (PNW) and the NNU.5 Historically at Colchester Hospital, infants with suspected sepsis who are clinically well but require IVABs due to risk factors were cared for at the mother’s bedside on the PNW in ‘virtual’ transitional care. They would be transferred by a member of the midwifery team to the NNU twice a day for the administration of IVABs by two neonatal nurses. On most days, this could be three or four infants, on some days a train of up to nine babies would travel to NNU. This process was fraught with issues, many of which were the drivers for changing practice, including:
- separation of mother and infant – this can disrupt bonding and breastfeeding and have harmful effects on the mother-baby relationship
- drug errors – mostly missed and delayed doses
- patient safety – transferring infants though the hospital results in infection control issues
- workload – the increased presence of infants on the NNU distracted staff from caring for their infants. Midwifery staff ‘missing in action’ as they accompanied infants to the NNU.
Collecting data
A time in motion study was performed of the infants’ journey while on a course of IVABs. This offered tangible quantitative data to highlight the issues around maternal and newborn separation (FIGURE 1). To summarise, this demonstrated that an infant on a five-day course of IVABs would be transferred 22 times, totalling eight hours. This represents eight hours of mother-baby separation and eight hours of staff time as the midwifery team member had to remain with the infant while they received their antibiotics.
Datix incident reports were reviewed; TABLE 1 shows some of the themes that were identified with this practice.
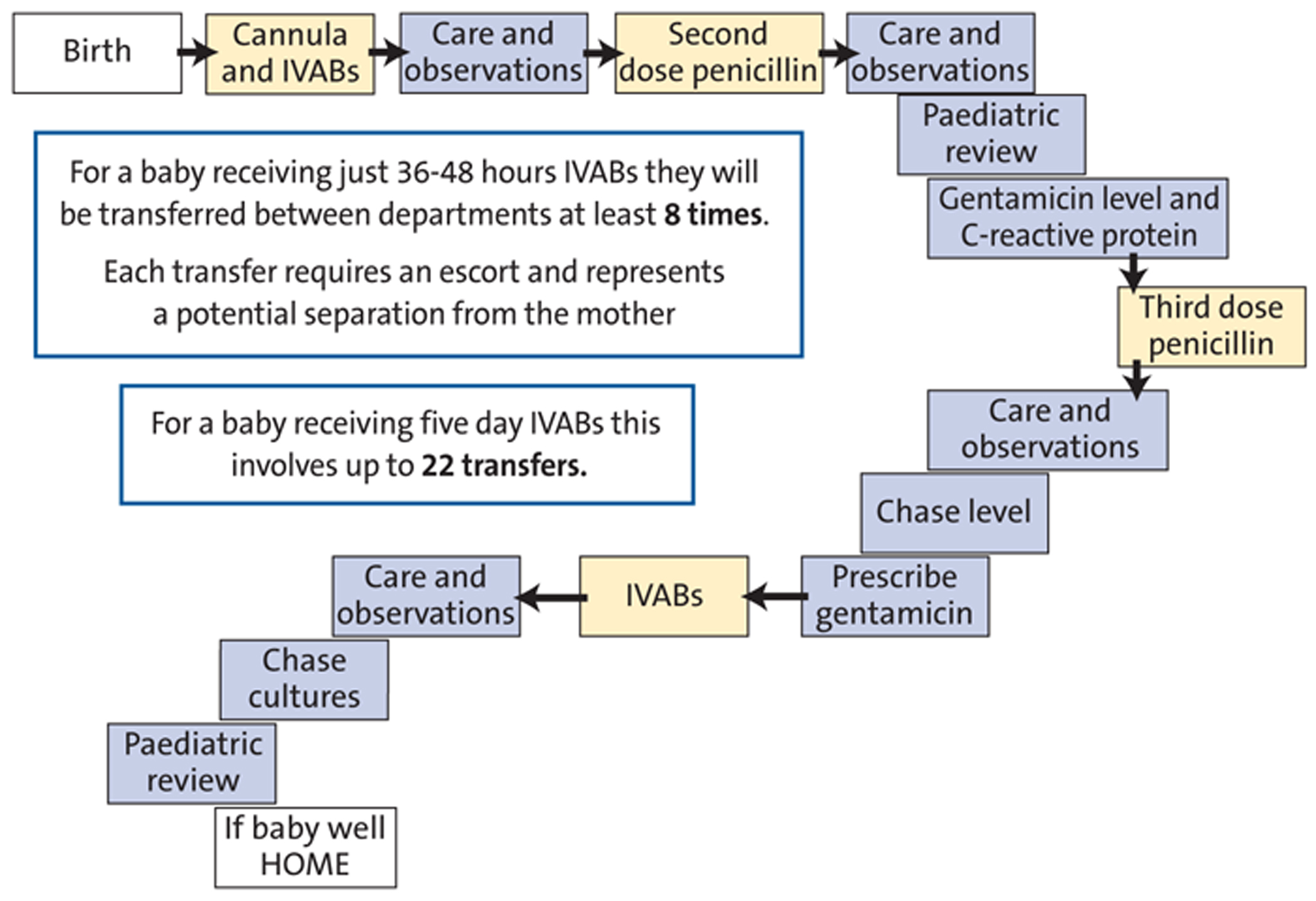
FIGURE 1 An infant’s journey while on a course of IVABs.
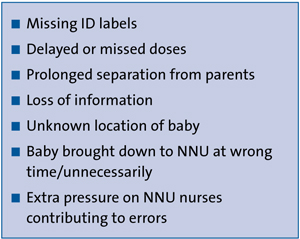
Table 1 Themes identified in a review of the Datix incident reports.
An impact analysis was conducted to examine how the original practice affected those involved (FIGURE 2). This was presented, along with the above data to key stakeholders, the heads of midwifery and lead nurse for children’s nursing, and it was agreed that a change in practice was required to improve the care of these infants.
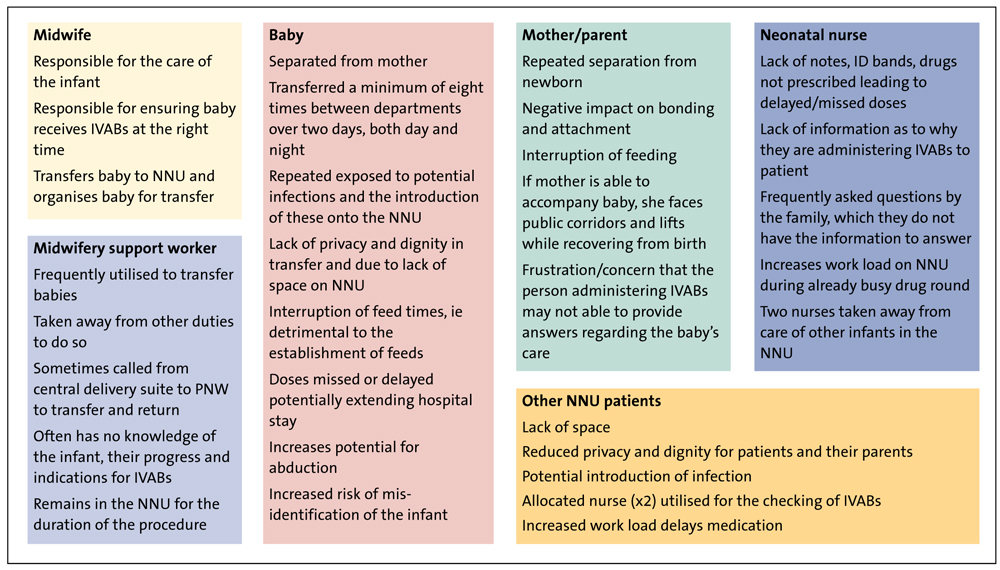
Figure 2 An impact analysis to examine the effects of the original practice.
Aims and objectives
In light of the concerns a new practice was designed whereby midwives would become the second checkers and would administer the antibiotics alongside the neonatal nurse, at the mother’s bedside on the PNW. The SMART (specific, measurable, attainable, relevant, time-limited) objectives can be seen in TABLE 2.
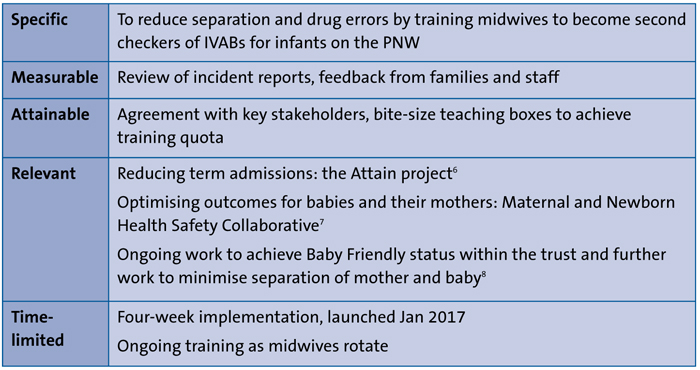
TABLE 2 SMART objectives.
Setting
Colchester Hospital NNU is a level two local NNU with 3,700 births per year, 464 admissions to NNU and 260 infants treated for suspected sepsis; an average of three infants per day. The PNW is located on the floor above the NNU and is accessed via one of two lifts used to transfer patients as well as staff and visitors.
To gain context at a regional level, we performed a benchmarking exercise across the East of England neonatal network (FIGURE 3). We found our issues were echoed across the network. The feedback from many units was that they had similar problems with missed and delayed doses of antibiotics. In a large proportion of units, the neonatal nurses administered antibiotics and, of those units where transitional care was available, there was still a majority of neonatal nurses administering IVABs.
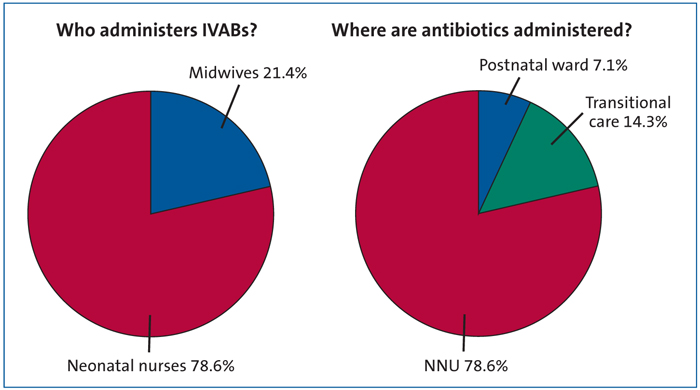
FIGURE 3 Regional benchmarking across the East of England neonatal network, 2017.
Methods
It was acknowledged early on that traditional teaching methods (ie study days) would not be possible, nor would we be able to train midwives en mass because of workload and staffing shortages. We had to think outside the box and came up with a solution inside a box – a training package of bite-size teaching boxes was developed to facilitate ad hoc teaching on the ward. The bite-size boxes had all the necessary resources to teach each topic, with each session lasting around 15-20 minutes. There are four topics that are worked through in order:
- Understanding neonatal sepsis
- Checking the drug chart
- Drawing up drugs
- Administration and cannula assessment.
Each of the four teaching boxes contains a training manual detailing what is required of the key trainer to run the session, and background information on the specific theory. There is a flip chart of theory and simulation/training materials for each session.
All of the boxes take a family integrated care approach to facilitate empowering the parents to care for their infant. As the infant's main carer, the parents are best positioned to notice any change or deterioration in their child and, if adequately supported, they will take care of the cannula and will remember antibiotic times.9 Each teaching session describes what to tell parents and gives examples of the type of language to use to make difficult medical jargon more accessible.
Upon completion of the teaching package the midwives were given a competency booklet which explained their roles and responsibilities and entailed a short numeracy quiz. To become competent as second checkers they needed to complete this booklet and have their first two episodes of checking IVABs observed and signed off. The project was launched in January 2017 and in the four weeks leading up to that we rolled out the bite-sized boxes and training package. We also displayed posters and sent out emails informing staff of the upcoming change in practice. Training was undertaken by the authors and 80% of staff were trained before the launch; after we launched we were able to provide ad hoc teaching for those staff that had not yet been trained.
Mechanisms
FIGURE 4 shows the mechanisms of working and the implications for practice.
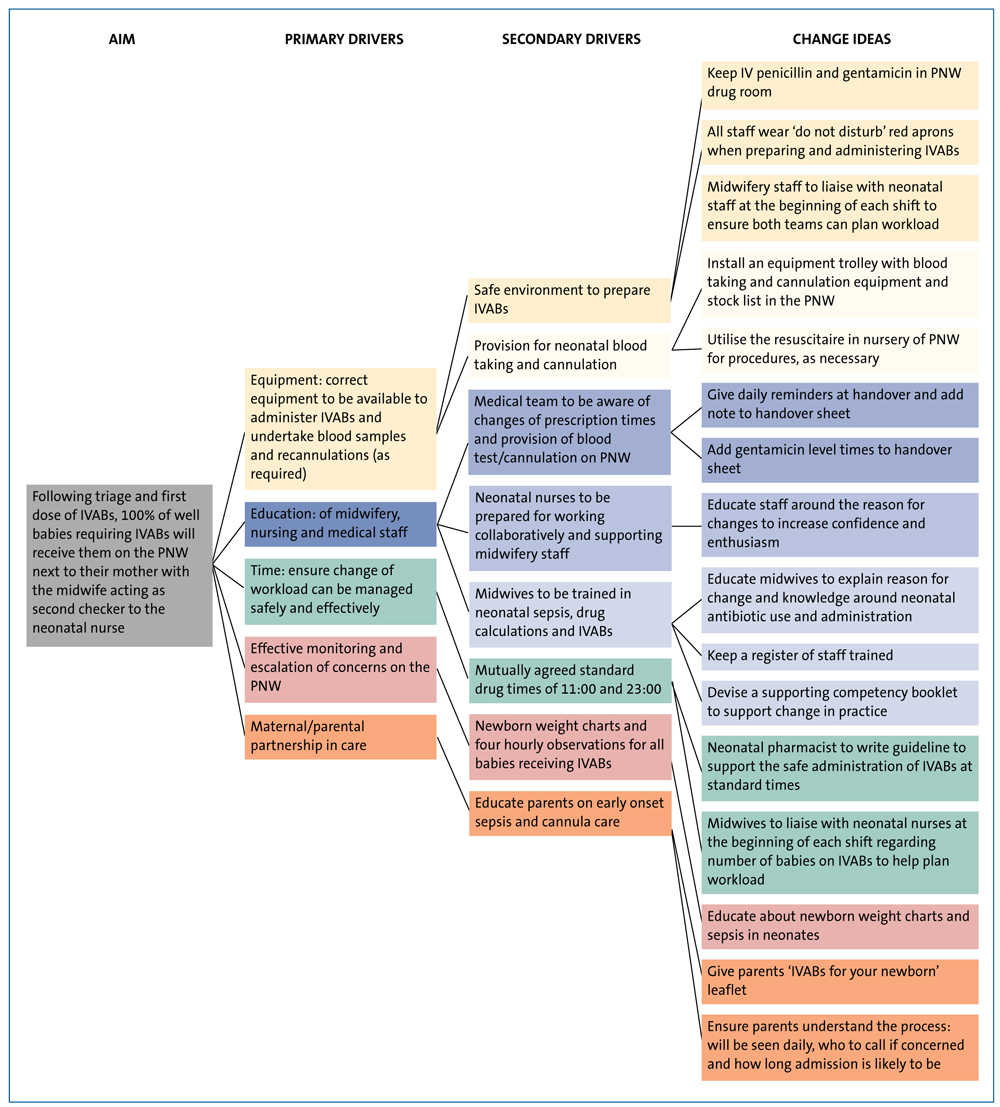
FIGURE 4 The mechanisms of working and the implications for practice.
Measures
Following training and implementation of the new way of working, there was only one drug error – a prescribing error of gentamicin at the wrong time. A root cause analysis was performed by the ward manager and this was attributed to human error.
There were some practical difficulties encountered during implementation that required alternative measures:
Lighting – it was found that the low lighting at night sometimes made safe administration at the bedside difficult. If this cannot be rectified, the baby can be moved to a well lit nursery for its IVABs (with the mother’s consent).
IV trolley and equipment – the PNW now has to stock new items. In the transition period the trolley was stocked from the NNU. Now the full stock list is being implemented on the PNW.
Baby receiving IVABs while mother in the central delivery suite (CDS) – one baby had a delayed dose as it was neither on the NNU nor PNW. It was agreed that babies on CDS would have their IVABs on the NNU until the mother and baby are transferred to the PNW.
Isolated mothers – a potential issue with neonatal nurses entering rooms where mothers have been isolated due to possible infection. With these cases, there is a need for improved communication. The babies are administered last and strict infection control procedures are adhered to.
Delayed blood culture reporting – 36-hour blood culture reports are often not available due to a delay in plating and/or microbiology staff not available out of hours.
Recannulation– babies were brought to NNU for recannulation. Where appropriate, the registrar now attends the PNW.
Data and results
Feedback was collected anonymously from staff by way of semi-structured surveys. These were reviewed by the authors and a thematic analysis conducted.
Workload concerns were raised with both maternity and neonatal nurse teams commenting on how they initially felt it had increased their workload although they understood the importance of not separating mother and baby. One midwife commented: “It was great that a baby could have its antibiotic while breastfeeding.”
Feedback from the midwifery support workers was the most positive as they felt glad they no longer had to take the baby train to NNU for antibiotics: “I can be much more use on the postnatal ward. No more baby trains!”
The neonatal nurses felt it impacted their workload by taking them off NNU for up to an hour sometimes. However, it was acknowledged that it felt safer as they were no longer being pulled in different directions while trying to check drugs on the NNU.
The overwhelming response from all teams was that collaborative working had improved communication, with one neonatal nurse reporting: “I actually get to put faces to names of some of the midwives who I’ve been talking on the phone to for years.”
Maternal feedback was sought by informal interview although the feedback is of limited value because the mothers had only experienced the new way of working. One mother who was post-caesarian section expressed concern that had antibiotics been administered to her baby in the original way, she would have found it very difficult.
Discussion
The project so far has been met with a positive response. There was an initial reticence by midwives to increase their workload and many expressed an understandable anxiety about drug calculations in newborn infants; smaller patients than they were used to.
An improved working relationship between the PNW and NNU has been a consistent response from both teams. Going forward, this will foster a better culture of collaborative working.
A reduction in drug errors is evident from the reduction in incident reports, although this process always relies upon an openness to report errors. One of the drivers for change was a reduction in drug errors, something that is high in the neonatal population. Gentamicin accounts for 15% of drug errors so taking measures to improve this statistic was paramount for increasing safety of our newborns.10
The project was presented at the East of England Neonatal Operational Delivery Network clinical oversight group and received lots of support and positive feedback. There was encouragement from the lead nurse for others to consider such projects in their own trusts and subsequently the authors have been contacted to share their resources. The bite-size boxes have been key to the successful implementation; being able to train midwives on an ad hoc basis has facilitated training for a greater number of staff.
Most importantly, we have waved goodbye to the baby train and kept babies and their mothers together during a time when they are bonding and establishing breastfeeding. Our next step is to try and reduce antibiotic use.
Acknowledgement
The authors are grateful for the help of Liaison Midwife Linda Humphries and Practice Development Nurse Lindsay Harding-Payne.
Or read this article in our
Tablet/iPad edition
- Previously at Colchester Hospital, a ‘train’ of babies would travel from the PNW to receive IVABs on the NNU.
- A QI initiative set out to reduce maternal and newborn separation and drug error incidents by administering IVABs on the PNW.
- The project improved safety and collaborative working between maternity and neonatal services.
Also published in Infant:
