

Optimising the delivery of parenteral nutrition in newborn care
Parenteral nutrition (PN) is a key component of newborn care, especially for preterm and growth restricted infants. Inadequate nutrition is associated with growth failure and suboptimal development. The 2016 British Association of Perinatal Medicine (BAPM) Framework for Practice provided the first UK standards for delivering PN. This articles describes a quality improvement initiative in a neonatal intensive care unit that successfully optimised PN feeding regimens resulting in higher protein and lipid intakes over the first five days of feeding, in line with BAPM recommendations.
Yasmin MilnerBSc, MSc, MBBS
Foundation (F1) Doctor
Barts NHS Trust, London
William Stagg
MEng, MBBS
Foundation (F1) Doctor
Medway Hospital, Gillingham, Kent
Helen McElroy
MBChB, MSc, FRCPCH
Consultant Neonatologist
Medway Hospital, Gillingham, Kent
hmcelroy@nhs.net
Parenteral nutrition (PN) is the administration of intravenous nutrients to support a non-functioning, inaccessible or immature gastrointestinal system, which renders oral or enteral feeding unsuitable. PN is vital for preterm infants with low nutritional reserves and an immature gut, especially during periods of critical illness.
In 2010 the National Confidential Enquiry into Patient Outcome and Death (NCEPOD) conducted an observational study of practice in UK neonatal units and revealed that more than 75% of infants requiring PN received sub-optimal nutritional care, particularly those of extremely low birth weight.1 The authors concluded there was significant room
for improvement in both clinical and organisational care, urgently recommending a UK consensus on best practice including NICE (National Institute for Health and Care Excellence) guidance. Subsequently in 2016 the British Association of Perinatal Medicine (BAPM) produced the first national framework for practice.2,3 NICE guidance is in progress with a projected publication date of early 2020, ten years after the first concerns were highlighted. Organisations interested in providing input are encouraged to register as stakeholders at www.nice.org.uk/guidance/indevelopment/gid-ng10037.
In this article we reiterate the value of PN and address the challenges of optimising PN delivery to align local practice with BAPM standards via a quality improvement (QI) initiative.
The goal of nutritional care
The goal of nutritional care in the preterm infant is to deliver adequate macro- and micro-nutrients to promote postnatal resumption of growth at a rate approx-imating intrauterine growth.4 Those born at very low birth weight (VLBW, <1,500g) or with intrauterine growth restriction (IUGR) have a limited energy reserve yet their dynamic physiological state and the stress of any additional clinical morbidities constitute a significant nutritional demand.
Growth requirements of preterm infants:
the role of PN
PN is used to achieve optimal postnatal growth in preterm and other infants who are unable to tolerate a full enteral feeding diet. Optimal PN should provide sufficient calories and protein to avoid a nutritional deficit that would otherwise result in a catabolic state. An energy supply of 90-120kcal/kg/day is needed to approximate intrauterine growth in VLBW infants with an amino acid supply on day 1 of 1.5g/kg/day and day 2 onwards of 2.5-3.5g/kg/day as advocated by the European Society for Paediatric Gastroenterology, Hepatology and Nutrition (ESPGHAN).5
Such early nutritional support, with high energy and protein intakes from PN, acts as a mediator of the relationship between critical illness in the first weeks of life and later growth, mortality, morbidities and neurodevelopmental outcomes.6-11
Postnatal growth failure
The target growth rate, ie that approximating fetal growth rate in the third trimester, was proposed by the American Academy of Pediatrics in 1977 and has been widely accepted despite a paucity of supporting data. Ehrenkranz et al demonstrated that it could be achieved after the first 2-3 weeks and once birth weight had been regained, but warned that most infants born between 24 and 29 weeks of gestation will not reach the median weight of the reference fetus at discharge and many will be less than the 10th percentile.9
The fetal growth rate is now contested as a credible target given that it is not achieved by most preterm infants. Growth patterns from a contemporaneous cohort of preterm infants in the UK show that those born at 29 weeks’ gestation and above take two weeks before they stop crossing centiles downwards, and those born at 22-28 weeks take much longer.12 These patterns, from over 5,000 infants, provide a more realistic target for judging growth once weight gain has stabilised but are equally suggestive of inadequate postnatal nutrition. This postnatal growth failure remains a common problem in preterm infants with 40-60% experiencing a fall in weight between birth and discharge despite concerted efforts by neonatologists to improve nutritional strategies.13,14
Postnatal growth failure is related in part to inadequate nutrition in the first weeks of life and has significant short-term impact including an association with an increased length of stay, increased need for ventilation and infection risk.15 Optimising energy intakes by maximising PN would seem to be the ideal strategy to prevent growth failure. Paradoxically it has been shown that the most critically ill infants receive even less energy in the first seven days of life than healthier infants, corres-ponding to even slower growth velocities and significantly higher odds for neuro-developmental impairment and death.14
There are many reasons for a failure to provide adequate PN, which can be simply summarised as started too late, given too little and increased too slowly (TABLE 1). Any delay in commencement of PN will result in protein and calorie deficits that contribute to a lack of postnatal catch-up growth.
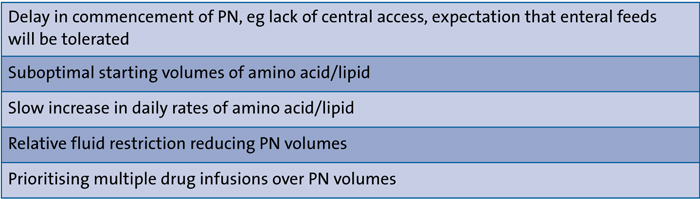
TABLE 1 Causes of inadequate PN.
Local QI initiative to optimise delivery of PN
In 2013 the neonatal unit at Medway Hospital participated in NEON (Nutritional Evaluation and Optimisation in Neonates), a randomised controlled trial that compared lean body mass at term in extremely preterm infants randomised to receive the recommended daily intake of parenteral amino acids from day 1 compared to an incremental provision of amino acids.15,16 Recruited infants received much higher volumes of both amino acid and lipid compared to our usual practice. These volumes were well tolerated by our infant population and this sparked interest in determining whether our current PN regimen was delivering optimal nutrition. In addition, junior doctors remarked that the quantities of PN prescribed for infants were lower than at other units where they had worked. The publication of the BAPM framework in 2016 provided further incentive to review our standard of care.
Methods
A simple QI initiative was designed using PDSA (plan-do-study-act) cycles to optimise delivery of PN in line with BAPM recommendations. The fluid and obser-vation charts were reviewed to measure actual volumes of amino acid and lipid delivered and compared to intended volumes (according to the current unit guidance) to quantify the PN deficit for each infant. This was conducted over a five-month period for preterm infants <30 weeks gestational age and <1,250g birth weight who had completed at least five days of PN. The duration of data collection was limited by the time allowed for the QI project conducted by final year medical students. Data collected on 14 infants demonstrated a notably lower intake than suggested by BAPM guidance (TABLE 2).
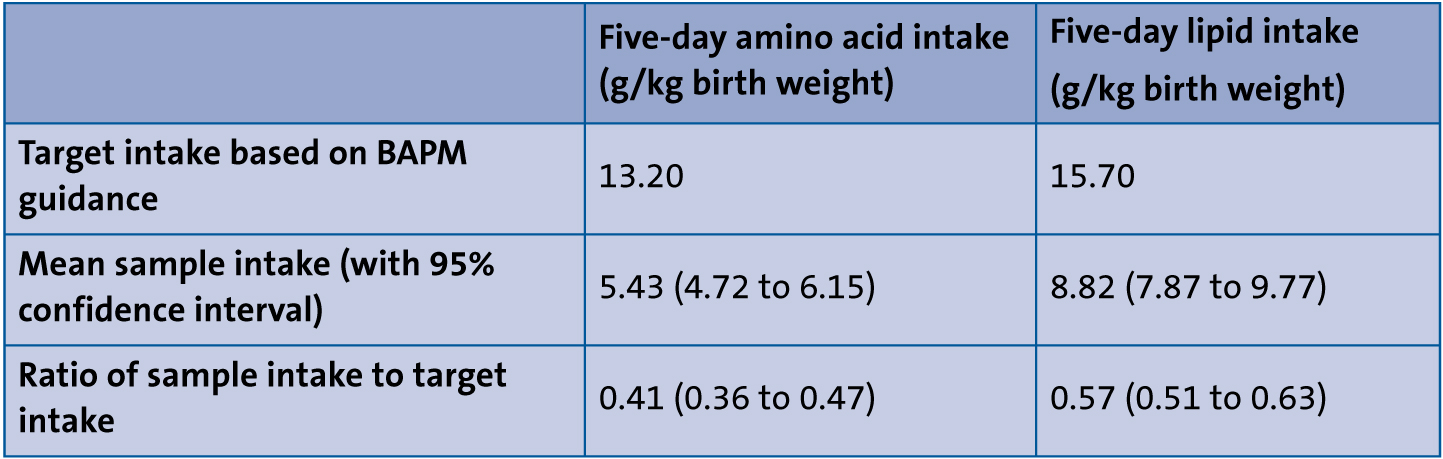
TABLE 2 Data on 14 infants before QI changes.
In response, a number of actions were implemented:
- The data was presented at a multidisciplinary unit meeting to raise awareness of the nutritional deficits and potential impact.
- New unit guidance was drawn up to incorporate BAPM recommendations. For protein, BAPM recommends starting at 2-2.5g/kg/day intake of protein, working up to 2.7-4g/kg/day by day 5, with a target set on the unit for 13.2g/kg total amino acid intake over the first 120 hours as a daily increasing regimen. For lipids, BAPM recommends starting at 2g/kg/day working up to 3.5-4g/kg/day by day 5, with the unit target therefore set at 15.7g/kg in 120 hours.
- The unit PN formulation was reviewed and amended in line with ESPGHAN and BAPM requirements resulting in a slightly higher content of amino acid per unit volume of PN.
- Fluid charts were revised to separate nutritional prescriptions (amino acid, lipid, milk) from non-nutritional prescriptions (dextrose and other drug infusions) and place emphasis on prioritising nutritional intake above a total daily fluid volume.
- PN daily volumes were changed to meet BAPM targets, giving both higher levels per day and a more rapid increase, reaching target daily PN rates in three days, as opposed to five days.
After implementation of these changes, data on 29 eligible infants were collected over the following 12 months, demonstrating a significant increase in nutritional intake with a 101% increase in protein intake, and 44% increase in lipid intake, over the first five days of feeding for preterm infants on the unit (TABLE 3). The improvement in cumulative intakes are impressive but still fall slightly short of BAPM minimum recommendations, emphasising the difficulty of achieving these national targets (FIGURES 1 and 2).
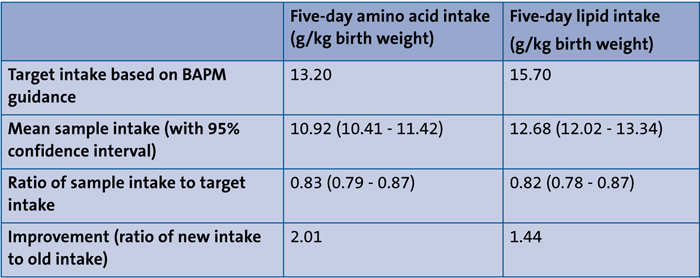
TABLE 3 Data on 29 infants after QI changes.
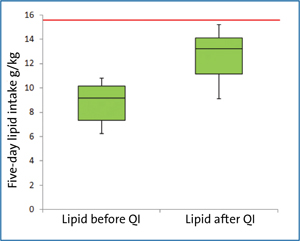
FIGURE 1 Cumulative five-day lipid intake before and after QI initiative. The red line indicates target intake.
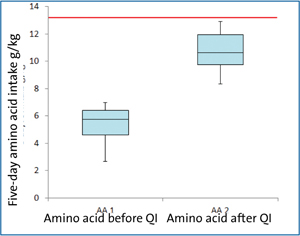
FIGURE 2 Cumulative five-day amino acid intake before and after QI initiative. The red line indicates target intake.
Challenges of implementing guidance
This QI project identified a number of challenges to delivering PN at adequate volumes to achieve BAPM targets. There remains a concern that excess fluid is detrimental and may increase the incidence of morbidity, ie chronic lung disease. However, the NEON trial demonstrated that increased volumes were tolerated and safe and many infants from our unit were recruited to this trial, indicating acceptance of the higher fluid regimens by senior medical staff.
The review of fluid prescriptions before implementation of changes indicated that there was a tendency on ward rounds to make decisions to pull back on total fluid volumes for the day to conform to a ‘historical’ practice of 60mL/kg on day 1 increasing daily by 30mL/kg up to 150mL/kg. When fluid regimens were complicated by additional infusions such as inotropes, heparinised saline, muscle relaxants, and/or morphine, these took up much of the daily allowance with the consequence that PN was sacrificed.
Prioritising nutrition on ward rounds
Recognising this concern about fluid volume and its impact on PN delivery was key to changing clinical practice on the unit. By raising awareness of the nutritional deficits faced by at-risk infants and introducing a series of small changes to the fluid prescription charts it was possible to embed the necessity of safeguarding the daily PN volume with all other fluid infusions administered additional to this. The effect was considerable on total five-day cumulative intakes for both amino acid and lipid. This practice continues on the unit as staff accommodate the change, suggesting that it represents a sustainable improvement.
Summary
PN is an essential component of optimal care for preterm infants. The successful implementation of an initiative to increase nutritional intake over the first five days of feeding for preterm infants required significant changes to the volumes of PN delivered to infants to achieve BAPM targets and equally important changes in team attitude and behaviours. We have shown an increase in both protein and lipid intake, 101% and 41% respectively, indicating an improved attainment of BAPM recommendations.
The much anticipated publication of NICE guidance on PN for this group of patients will provide further opportunity to review nutritional practices and ensure delivery of evidence-based practice.
Or read this article in our
Tablet/iPad edition
- Parenteral nutrition (PN) is an essential component of neonatal care.
- Postnatal growth restriction due to inadequate PN is common in preterm infants.
- Identification of nutritional deficits through review of practice enables optimisation of PN in high risk preterm infants.
Also published in Infant:
