

Quality improvement in the NICU: increasing the use of own mother’s milk
Human milk (HM), particularly own mother’s milk (OMM), is one of the highest impact, low cost interventions in the medical field with research constantly finding new and more impressive data to support this. OMM should be considered a medical intervention and an institutional priority, especially for those babies in the neonatal intensive care unit (NICU). However, no other medicine is administered, tracked or reported on as haphazardly as HM in the NICU.
Katie James
RM, MMid, IBCLC
Global Education Manager
Paul Bolla
BAppSc Global NICU QI Manager
paul.bolla@medela.ch
Vanessa Sakalidis
PhD
Global Education Manager
Nania G. Schärer-Hernández
PhD
Director Global Education
Medela AG, Switzerland
Impact of OMM in the NICU
Globally an estimated 15-20% of infants are born of low birth weight (<2500g)1 and approximately 10% are born premature (<37 weeks’ gestation).2 Many of these infants will require a NICU admission and may be unable to feed directly at the breast.
Providing milk is the most helpful thing mothers can do for their infant in the NICU.3 Preterm, sick and low birthweight infants are the most vulnerable of newborn populations and the ones who benefit the most from the life-saving properties of HM. Data indicate that these infants are, however, the least likely to receive OMM as early, often and for as long as is optimal.4

Preterm and sick infants in the NICU benefit most from their own mother’s milk.
OMM protects infants in a positive dose-response manner. Early doses (from birth to day 28) of OMM compared to formula feeding significantly reduce the risk of necrotising enterocolitis (NEC), bronchopulmonary dysplasia, retinopathy of prematurity, sepsis, nosocomial infection, cognitive and neurological impairments and rehospitalisation in infants born too early or small.5-11 Any amount of OMM can have an impact on the vulnerable infant’s health but research has shown a greater reduction in morbidities when a higher daily dose is available. For example, every additional 10mL/kg/day of OMM reduces the odds of sepsis by 19%.7 On the other hand, any formula in the first weeks is strongly associated with NEC:
- Infants have a 3.5x increased risk of NEC when they are fed any formula in the first 14 days9
- Infants have a 6-10x increased risk of NEC when they are exclusively formula-fed12
- Infants born at <30 weeks’ gestation have a 20x increased risk of NEC when they are exclusively formula-fed.13
In addition, investment into HM in the NICU, where it has the strongest effect at preventing morbidity and mortality, will result in considerable cost savings.9,14 For instance, the total lifetime cost savings in just one country (England) due to improved health outcomes if all preterm infants were fed HM instead of formula is estimated to be £46.7 million.15 Likewise, reductions in disease-specific costs in the NICU are significant; NEC treatment alone can account for up to one fifth of the total NICU expenditure.9
Simply increasing NICU doses of OMM from low (<25mL/kg/day) to high (>50mL/kg/day) results, on average, around US$31,000 being saved per infant, based on the reduction of a single late onset sepsis case alone.7 In this regard it is clear that there are significant health and economic gains to be made, with one health economist, Professor Tricia Johnson, Associate Chairperson of Education and Research in the Department of Health Systems Management at Rush University, stating that from a health economist’s perspective, the value of OMM is tremendous. Economically, we see a return of thousands of dollars in savings and substantially better health outcomes among our very low birthweight populations. The investment in a comprehensive lactation programme in the NICU is minimal relative to the potential cost savings (T. Johnson, 2019, personal communication).
Lack of NICU-specific feeding data
Globally, there is a paucity of standardised data outlining best practices for how HM and breastfeeding are supported in the NICU.16 Currently the only standard metrics for HM and breastfeeding outcomes assess the early initiation of breastfeeding (within one hour of birth) and exclusive breastfeeding at six months of life for all infants. These statistics, however, fail to target the unique situation of the preterm infant in the NICU. It is therefore not surprising that in Europe the rates of any breast milk feeding after preterm birth range dramatically from 36-80% and at discharge between 16 and 93% were breastfeeding.17
Comprehensive HM feeding data are not collected in a standardised manner for the preterm and sick infant populations. As such, the most vulnerable infants in our society are still not being routinely assessed on the dose of OMM received in the NICU. This is, in part, due to a lack of know-how and knowledge on what metrics to assess and how to measure them, making it increasingly difficult for NICUs to know whether their current practices are sufficient or not, or if any interventions implemented are of value.
In this regard, evidence-based improve-ments for lactation and feeding practices in the NICU have been consistently shown to increase infant health outcomes and long-term exclusive breastfeeding rates as well as providing economic benefits for NICUs. Although such practices are often employed individually and rarely in combination, they include:11,18-20
- parents being informed about the
benefits of HM
- early and frequent milk expression
- tracking the dose of OMM fed to the infant
- kangaroo mother care
- non-nutritive sucking
- oral immune care.
In order to effectively support lactation of the mother and the use of OMM for the vulnerable infant, NICUs should be highlighting and reporting upon the following important areas:
- number of infants receiving exclusive OMM for the first 14 days of life
- number of infants receiving high dose (>50mL/kg/day) OMM for the first 28 days of life
- volumes of OMM expressed daily
- number of mothers ‘coming to volume’ (defined as three consecutive days of >500mL total volume) by day 14.
Official bodies are clearly highlighting the need for more effective monitoring of how and what these vulnerable infants are fed. There have been some positive steps already taken by leading authorities to prioritise the assessment of the use of OMM for the preterm and small babies. The World Health Organization standards of care guidelines21 emphasise the importance of measuring the number of low birthweight infants fed exclusively OMM for the duration of their NICU stay.21 In addition, the Unicef UK Baby Friendly Initiative Guidance for Neonatal Units also clearly states the significance of standardising practice and metrics. This would ensure families have frequent and prolonged access to their infants, ideally in skin-to-skin contact. Furthermore, the guidance recommends that mothers are supported to express early and often, and have good access to breast pumps that can effectively establish and sustain their milk supply.22
Quality improvement to optimise OMM usage in the NICU
Quality improvement (QI) initiatives follow a plan-do-study-act (PDSA) cycle in order to monitor, compare and assess current and future performance. In order to optimise the use of OMM in the NICU, it is essential to not only improve the mother’s lactation outcomes but also the feeding and care practices for the most vulnerable infants. QI starts with a baseline assessment of current practices to identify gaps and prioritise evidence-based interventions according to the available resources.23,24
In order to assist the development of a QI programme, a NICU scorecard has been developed (FIGURE 1). It draws from the health economics and OMM dose research of Meier and colleagues5-11 as well as the 10 steps to promoting and protecting breastfeeding for vulnerable infants from Spatz et al.18,19,23,25,26 The scorecard indicators summarise evidence-based best practices that lead to increased availability and sustainability of OMM for vulnerable infants and aim to help the self-assessment of a NICU’s current HM and lactation care practices (FIGURE 2). The complete NICU QI toolkit provides neonatal units with education modules and data collection tools that help improve specific lactation practices in identified areas of need.
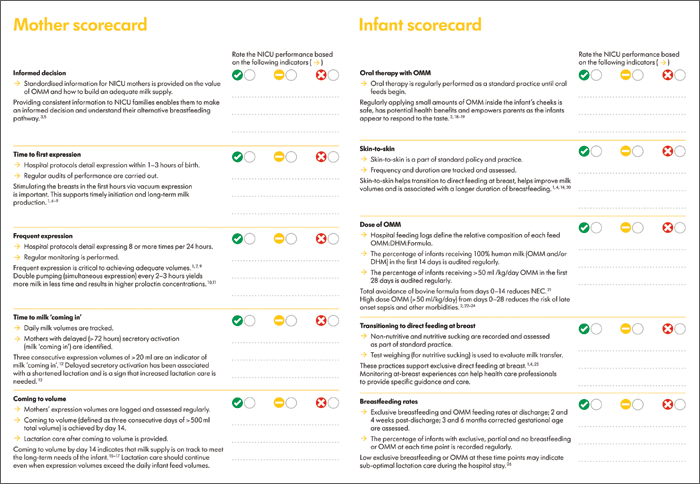
FIGURE 1 The NICU scorecard, which aims to improve the use of human milk in the NICU by allowing the self-assessment of a NICU’s current HM and lactation care practices.
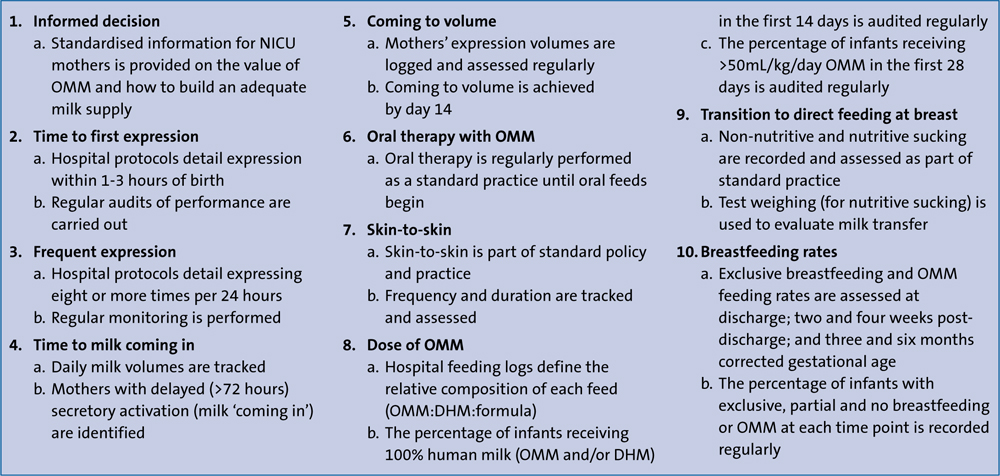
FIGURE 2 The 10 performance indicators. Healthcare professionals can evaluate their current policies and practices and, by identifying potential gaps, undertake QI initiatives to ensure that infants receive human milk through their hospital stay and beyond. Key: OMM = own mother's milk, DHM = donor human milk.
The main aims of introducing the scorecard in the NICU:
- awareness of current lactation practices
- improvement in practice to achieve:
- higher dose of OMM for infants
- reduction in morbidities
- reduction in length of stay
- increase in breastfeeding rates post-discharge
- reduction in costs.
Case study: QI improvements in a Japanese NICU
Acknowledging that there was room for improvement, one of the largest NICUs in Japan employed the NICU QI scorecard initiative over a five-month period from April to August 2018 (FIGURE 3).27 During this period this NICU saw increases to their exclusive HM feeding rates at one month post-discharge from 15 to 43%. Although the staff had prior knowledge of the importance of HM for the vulnerable infant, standardised data collection exposed areas for improvement within current practice. Through the implementation of three of the scorecard’s 10 indicators (FIGURE 3), vast increases were seen in the percentage of women enabled to make informed decisions, the rates of early first expression and the total number of expression sessions within 24 hours.
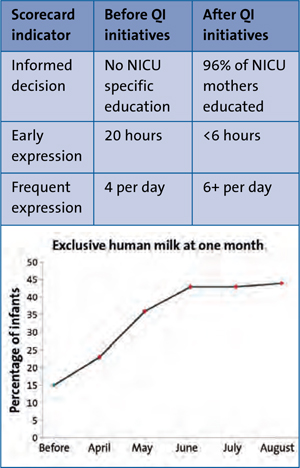
FIGURE 3 QI improvements in a Japanese NICU through implementation of three of the scorecard’s 10 indicators.
Standardising future feeding practices
It is clear from the literature that vulnerable infants in the NICU benefit most from the health-giving effects of high doses of OMM. However, there continues to be a dearth of available data on the number of infants receiving sufficient doses of HM in NICUs globally.
From a health economics perspective, NICUs cannot afford to remain uninformed about the OMM dose and the costs (health outcomes and spending) associated with not accessing the full potential of OMM.
By broadening the conversation about current care practices within the NICU environment and how they support mothers to get optimum milk supply, the challenge is elevated to centre stage; thus ensuring all neonatal units work towards making access to OMM a priority. There is a clear call to action to standardise evidence-based practices. QI initiatives that focus on the specific evidence-based indicators outlined in the NICU scorecard are a starting point for NICUs to better support vulnerable infants and their mothers.
For more information and to access the NICU QI scorecard visit: www.medela.com/education-materials
Declaration
Medela AG manufactures and supplies breastfeeding products and medical vacuum technology for hospitals and individual applications worldwide.
Or read this article in our
Tablet/iPad edition
- NICU infants benefit the most from the health-giving effects of high doses of OMM but they are the least likely to receive it.
- Globally there is a paucity of data on NICU lactation care and feeding.
- QI initiatives that focus on the evidence-based indicators outlined in the NICU scorecard are a starting point for assessment and improvement of practices
Also published in Infant:
