

Expressing parameters, maternal milk yield and discharge breastfeeding outcomes – proposing future avenues of research
This article outlines exploratory analysis of a small audit population to generate hypotheses for further research on how mothers of preterm babies can optimally express milk to maximise the volumes expressed and improve longer-term breastfeeding outcomes.
Ilana Levene
BmBCh, MRCPCH
Neonatal Trainee
Gillian Denton
Neonatal Infant Feeding Lead
Frances O’Brien
MB BS, MRCP, DRCOG, BSc
Consultant Neonatologist
frances.o’brien@ouh.nhs.uk
Newborn Care Unit, John Radcliffe Hospital, Oxford
Receiving the maximum amount of mother’s own milk (MOM) is important to reduce morbidity and mortality in premature babies. For example, very low birth weight (VLBW) babies who receive less than half their nutrition as MOM in the first 10 days of life are 60% more likely to die, develop necrotising enterocolitis (NEC) or suffer from serious infections.1 Providing exclusive MOM, in comparison to any formula, is associated with odds ratio of 0.11 for severe retinopathy of prematurity.2 Increasing human milk exposure also incrementally improves brain growth and long-term neurodevelopmental outcomes.3,4
Lack of MOM impacts on NHS costs – VLBW infants with the lowest tertile of MOM intake have 22% higher overall neonatal intensive care unit (NICU) costs (corrected for other factors) than those in the highest tertile.5 Increasing any breastfeeding in babies at NICU discharge from 50% to 75% in the UK could lead to annual savings of nearly £4 million from reduced cases of NEC during the admission period alone.6
However, mothers of preterm babies have a high risk of poor milk supply and non-exclusive breastfeeding.7,8 40% of babies born in the UK at <33 weeks’ gestation were exclusively formula fed at discharge home in 2017.9 Breast tissue may be underdeveloped at delivery when babies are born prematurely. Antenatal steroids required for lung maturation del The challenges are multiple – mothers must establish and then maintain their milk supply by mechanical expression, which they can find difficult.10,11 Breast tissue may be underdeveloped at delivery when babies are born prematurely. Antenatal steroids required for lung maturation delay lactogenesis stage II (copious milk production).12 These factors combine to contribute to high levels of insufficient milk supply, anxiety over expressed milk yield10,11 Breast tissue may be underdeveloped at delivery when babies are born prematurely. Antenatal steroids required for lung maturation del and an increasing failure to meet mothers’ goals for human milk provision as time goes on.13
A third of mothers of preterm babies report poor milk supply and the most common question put to researchers is how to express more milk. Mothers have multiple practical questions about expressing, including how often to express, what milk yield they should target over time and whether they can reduce expressing once supply is established (Levene, unpublished survey). Unless advised differently, mothers generally target their expressed milk yield to their baby’s enteral needs, which are minimal in the early period for very preterm babies, and this may be particularly important in setting up a suboptimal long-term milk supply. There are significant gaps in the literature regarding how to optimally express to maximise expressed milk volumes and longer-term breastfeeding outcomes for preterm babies. If clinical teams are to give evidence-based care to families, investment is needed in practically focused expressing research.
The Unicef Baby Friendly Initiative (BFI) makes concrete recommendations for best practice for expression of breast milk in the neonatal unit:14
- Express as soon as possible after delivery, with a target of within two hours
- Express 8-10 times per day
- Express at least 750mL per 24 hours by day 10-14 of life.
All of these recommendations are extremely demanding for mothers, with the majority even in trial settings expressing fewer than six times in 24 hours15 and obtaining mean yield far below 750mL.16 The recommendations are based on the physiology of lactation for term infants and while this is a rational approach there is relatively little data to support these specific targets in the context of prematurity. A pilot randomised controlled trial has shown that expressing within one hour of delivery improves expressed volumes for at least the first three weeks17 and initial reports of the full trial show that the effects of early expression persist at least to discharge.18 There are no other relevant randomised controlled trials, and cohort studies have reported on the correlations of less demanding targets such as expressing within six hours of delivery,19-21 expressing at least five times a day22,23 or targeting more than 500mL per day in the first 10-14 days.16,22,23
Given that preterm babies have a much more gradual increase in volume intake as they grow than term babies and are generally lighter when they start comple-mentary feeds, it is possible that the meaning of a ‘full supply’ for mothers of preterm babies is different to term babies and that the targets set by BFI could be refined, thus reducing the burden on mothers. If less rigorous recommendations are equally effective, staff may be more likely to emphasise them to mothers and help families to see them as achievable and realistic. For example, in current practice mothers are rarely informed about the BFI volume target, partly because staff worry that it will increase anxiety and demotivate mothers expressing low volumes. However, equally it may be that these rigorous recommendations are necessary to over-come the multiple physiological disadvantages that mothers of preterm babies face in establishing milk supply, in which case strong evidence will help staff put this case to families more convincingly.
This report uses data from an existing small audit to generate hypotheses, in preparation for larger scale experimental studies.
Methods
A two-centre audit was conducted in a level II (local neonatal unit, LNU) and a level III NICU in the Thames Valley neonatal network. A convenience sample of mothers who had initiated expression of breast milk was interviewed between October 2017 and January 2018. At that time, the level II unit was seeking level 3 BFI re-accreditation within its maternity unit and the level III unit was nearing assessment that resulted in level 2 BFI accreditation as a stand-alone neonatal unit. The level III unit had 2.3 full-time equivalent staff in a dedicated neonatal infant feeding team. Both units have better than average performance in national audit measurements of breastfeeding in preterm babies.9
The women were asked when they first initiated breast milk expression and asked about their 24-hour expressed milk yield at three time points: seven days, 14 days and 21 days, or at the time of interview if the baby was older than 21 days (this combined time point is referred to as ≥3 weeks). Permission was then requested to prospectively record information on feeding at discharge. Exclusive breast-feeding at discharge was defined as exclusive MOM intake (regardless of breast milk fortifier use) by any route. Mothers who had sufficient milk to exclusively breastfeed but chose for lifestyle reasons to introduce formula were excluded from analysis from that point.
Due to the small sample size, non-parametric Mann-Whitney test, Fisher’s exact test and Spearman’s correlation were used in the analysis.
Results
Descriptive
Thirty-two mothers were included (13 from the level II unit, 19 from the level III unit). Mean gestation at birth was 29+1 weeks (range 23+5 to 35+0 weeks) with a mean birth weight of 1,312g (range 570g-2,500g). Mean age at the time point classified as ≥3 weeks was 38 days (range 21 to 100 days). Discharge feeding classification was known for 26 of the mothers (81%), two of whom were excluded from discharge analysis due to death or discharge on parenteral nutrition. Three mothers chose to introduce formula with no concern over their milk supply – their mean expressed yield at ≥3 weeks was 1,050mL. Therefore, 21 mothers contributed data to the discharge feeding classification.
Average expressing behaviours are described in FIGURE 1 and TABLE 1.
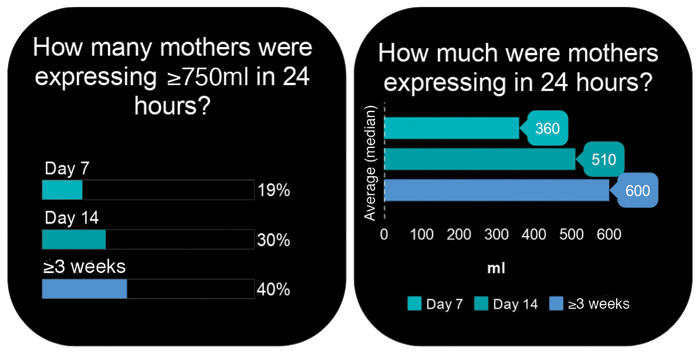
FIGURE 1 The amount of milk expressed by mothers over time.
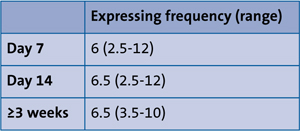
TABLE 1 The frequency of expression in 24 hours.
Time to first expression
Thirty-one per cent of mothers first expressed within two hours of delivery with median time to first expression of six hours (range 0.5-48 hours).
Expressing within two hours of delivery was significantly associated with yield at all three time points (TABLE 2).

TABLE 2 The 24-hour yield of expressed breast milk (median in mL). *p=0.03, **p=0.04
Seventy-six per cent of those expressing within two hours of delivery achieved the BFI target yield of ≥750mL at ≥3weeks whereas only 25% of those expressing more than two hours after delivery did so (p=0.03). One hundred per cent of those who had expressed within two hours of delivery were exclusively breastfed at discharge, compared to 39% of those expressing more than two hours after delivery (not significant, p=0.09).
No confounding factors were identified – expressing within two hours of delivery was not associated with frequency of expressing or gestational age at birth.
Expressing frequency
Expressing frequency on day 7 has a strong positive correlation to yield on day 7 (Spearman’s rho = 0.69, p<0.001). FIGURE 2 demonstrates that yield is highly variable within bands of expressing frequency, but there may be a linear ceiling of possible yield at each frequency.
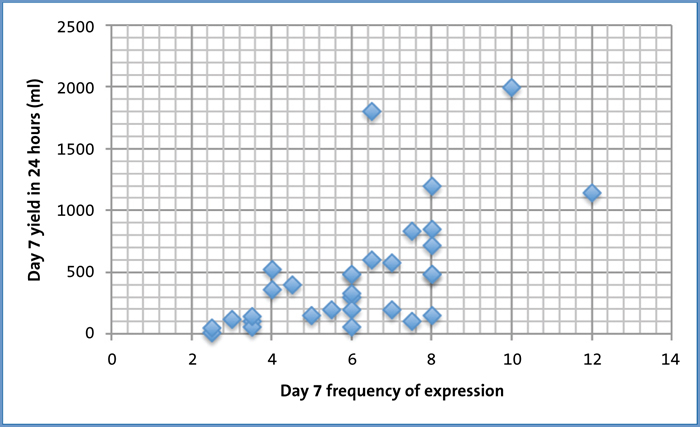
FIGURE 2 Expressing frequency and yield on day 7.
There was an interaction between expressing within two hours and express-ing frequency, so that day 7 yield was higher at a specific expressing frequency for mothers who had initiated expression within two hours of delivery (p=0.01).
Expressing eight or more times a day at day 7 was associated with significantly higher yield, as was expressing six or more times a day to a smaller extent (TABLE 3).

TABLE 3 Relationship of expressing frequency and yield on day 7. *p<0.007
There was a moderate correlation of expression frequency on day 7 with yield on day 14, and of expression frequency on day 14 with yield at day 14 (Spearman’s rho = 0.57, p<0.001 and Spearman’s rho = 0.50, p=0.005 respectively). Yield at ≥3 weeks was not correlated with expression frequency at any time point.
Target yield and breastfeeding outcomes
Achieving BFI target yield (≥750mL) at ≥3 weeks of age was associated with exclusive breastfeeding at discharge (p=0.03) as shown in TABLE 4.
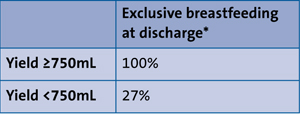
TABLE 4 Relationship of expressed milk yield in 24 hours at ≥3 weeks of age and exclusive breastfeeding at discharge. *p=0.03
Conclusion
This Thames Valley neonatal network audit shows that the majority of mothers did not achieve the BFI recommendations for milk expression, despite the units having good lactation support. This study has significant limitations due to its small size, retrospective nature and limited number of potential confounding factors measured. For example, expressing within two hours may have been associated with vaginal birth rather than caesarean, or with antenatal education about breastfeeding. Nevertheless, it suggests several interesting lines of research that should be pursued in large prospective studies or randomised controlled trials in the future.
The data support the recommendation for mothers to initiate expression within two hours of preterm delivery and suggest that early initiation may allow mothers to express less frequently. Strategies to increase the urgency of first expression are likely to significantly benefit mothers and their preterm babies, and this should be a major focus of multidisciplinary teamwork between maternity and neonatal teams.
The data support the BFI target yield of 750mL or more in 24 hours – higher than the 500mL target studied in existing literature.16,22,24 Although this target volume is much higher than the intake of a very preterm baby in the first weeks of life, the data reported here supports the idea that it is necessary to target high early volumes to enable longer-term exclusive breastfeeding, possibly because of a critical window to establish supply. However, the data clearly show that supply can be increased beyond the window of 10-14 days, with the percentage of mothers achieving target yield after day 14 increasing by a third. Therefore, a potential refinement could be moving the timeline to achieve target yield of 750mL from 10-14 days, to a later time point such as three weeks. Stepping stone targets at earlier time points would help ensure that mothers are on the right path.
The data also support the recommendation to express frequently in the early period, as expressing eight or more times a day in the first week is correlated with much higher early yield. Expressing six or more times a day (a more realistic frequency in this study and others)15 also divides mothers into higher and lower yield groups and given the uncertainty over the timing of volume targeting, it is unknown whether the difference between these two frequencies (eight times a day giving median yield of 785mL on day 7, and six times a day giving median yield of 480mL) is likely to impact on long-term breastfeeding outcomes. A recent study of expression frequency during predominantly the third week of life for mothers with good average yield showed that expressing more than five times a day did not add extra yield benefit,25 but the data reported here imply that this cannot be extrapolated to the first two weeks of life.
In summary, despite the small size of the study these data strongly support the core BFI milk expression recommendations. Some potential refinements to expressing frequency and target yield that may reduce the significant burden of expressing on mothers of very preterm babies are proposed. Further large-scale studies are needed to test these refinements, but this should not take away from the importance of investing in staff training to support mothers to express frequently and to aim for higher yield than their baby’s early needs in the first few weeks of life, in order to give themselves the best chance of fulfilling their breastfeeding goals over the long term.
Or read this article in our
Tablet/iPad edition
- Neonatal units and maternity teams should focus on encouraging and facilitating first expression of milk within two hours of preterm delivery.
- Mothers should be encouraged to express more milk than their preterm baby requires in the first few weeks of life, with a target of 750mL in 24 hours.
- Further work is necessary to analyse the optimal frequency of expression and at what time point the volume target should be applied.
