

Administering the Hospital Anxiety and Depression Scale within a neonatal unit
Within recent years there has been an emphasis on developing effective psychological screening for mothers within postnatal mental health services. This study builds upon a previous pilot study that introduced psychological assessment skills training to community midwives. Following this training, a local standard was implemented, requiring the Hospital Anxiety and Depression Scale (HADS) to be administered at day two following birth, and then every ten days after this. The current study assesses the experiences of neonatal unit staff administering the HADS five years on.
Christopher James Anderton1
Psychological Wellbeing Practitioner
Bianca Thomas1
Senior Psychological Wellbeing Practitioner
Sarah Pestell2
Psychotherapist and Counsellor
Nigel North2
Consultant Clinical Psychologist and Head
of Department
2Department of Clinical Psychology, Health Salisbury NHS Foundation Trust
shc-tr.clinicalpsychology@nhs.net
Pregnancy and the postpartum period represent a period of change and adjustment in a mother’s life, especially if childbirth is complicated and the life of the mother or baby is endangered.1 An infant’s admission to the neonatal unit (NNU) is an understandably stressful experience for parents and comes with a wide range of psychological and emotional challenges. Having to face these psychological and emotional stressors can greatly impact upon a mother’s psychological wellbeing.2
Mothers on the NNU are at greater risk of psychological distress, with up to 39% meeting the criteria for postpartum depression.3 This is in contrast to rates of between 10 and 20% for the general population of mothers developing anxiety and depression following childbirth.4 Traditionally, postpartum depression is described as being under-identified, under- diagnosed and under-treated.5 In an NNU setting, this may be partially explained by the fact that the child is the patient as opposed to the parents. This could potentially lead to a mother’s psychological needs being overlooked in comparison with her critically ill child.6
The current study follows a review of the maternity service at Salisbury District Hospital (SDH) and a previous pilot study (published in 2012) aiming to equip maternity staff with skills in recognising and referring mothers exhibiting psycho-logical distress for support.7 Maternity staff from SDH underwent psychological assess-ment skills training (PAST), and were trained to administer the HADS as part of their expanding roles as healthcare profess-ionals. The training was delivered over three sessions lasting two hours each. They found this training, alongside establishing a clear referral pathway, significantly increased staff confidence in recognising psychological distress and referring mothers to the Clinical Psychology Department. This is, of course, vital in a modern healthcare system where there is an emphasis towards giving equal status to both physical and mental healthcare.8
National Institute for Health and Care Excellence (NICE) guidelines state that health professionals may consider the use of the HADS as a screening tool in perinatal populations.9 However, this has now been implemented as a standard on the NNU at SDH. The use of the patient health questionnaire-2 (PHQ-2) as an alternative screening tool for mothers has been previously reported to yield high false positive rates,10 hence the implementation of the HADS, which has been found to be more accurate.7 For mothers, inadequate or absent psychological treatment can result in a range of adverse psychological, social and employment outcomes including the risk of relapse. Postnatal depression also has profound consequences for the child
in terms of attachment and psychological development.11 One study in particular found that all cases of adolescent depression in its sample were associated with depression in the mother during pregnancy and early life.12 Moreover, evidence suggests that children whose mothers had experienced perinatal mental illness are at increased risk of prematurity, low birth weight, irritability and sleep problems in infancy alongside behavioural and academic difficulties at school.13 The importance of detecting psychological distress in mothers is therefore vital.
The purpose of the current study was to explore the experiences of NNU staff in administering the HADS with a particular emphasis on what effects they believed its use had on mothers.
Method and analysis
Interviews
Individual staff from the NNU were approached and asked to take part in the study. In total, nine members of NNU staff consented and were interviewed individually by a member of the research team. All interviews were audio recorded with the knowledge and consent of the interviewee. With the questioning style being semi-structured in nature, this allowed flexibility for both interviewer and interviewee to explore and expand upon given topics that emerged during the interview. These particularly concerned enabling the interviewee to express their own views and experience of using the HADS, alongside their perspective of how mothers found completing it. Eight primary questions that were asked during the interview can be seen in TABLE 1.
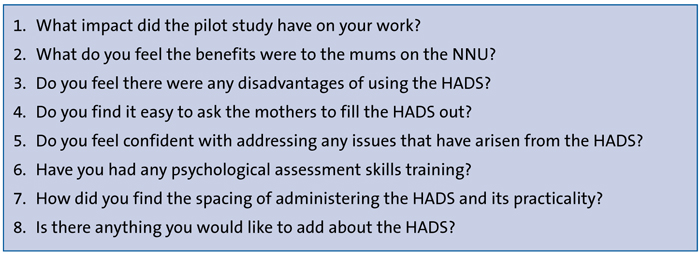
TABLE 1 The primary questions that were asked during the NNU staff interviews.
Analysis
The analysis itself was predominantly theme orientated, with the analytic process broadly following the three stages and procedures of thematic analysis outlined by Braun and Clarke.14 The COREQ guidance for qualitative research was followed.15 The first stage of analysis consisted of ensuring the transcripts accurately mirrored what was being said in the audio recordings. The second stage consisted of dividing and grouping into what became 17 sub-themes with four main over-arching themes. The third stage of analysis explored how these different themes related to one another, combining to produce the overall perspective and conclusion put forward in this article.
Findings and discussion
Four main over-arching themes were identified from the thematic analysis of interview transcripts (Figure 1).These will be discussed in turn, along with the individual sub-themes from which they are assembled.
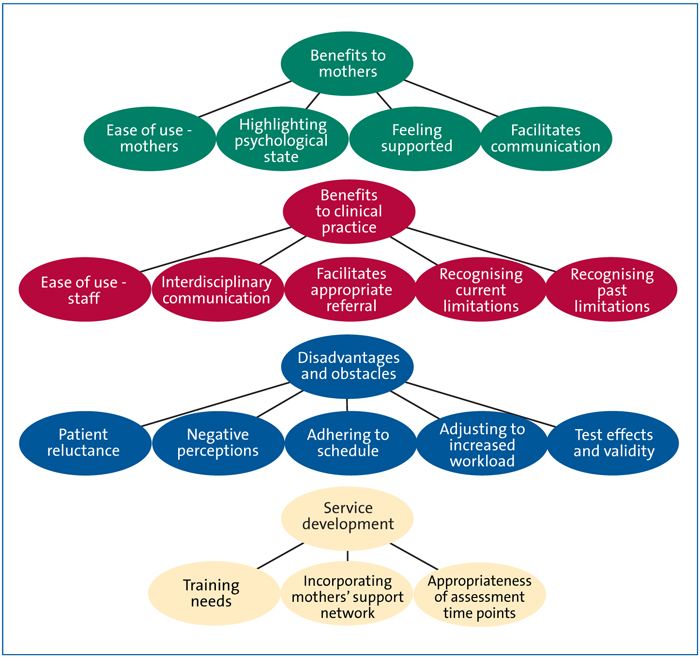
FIGURE 1 The sub and main findings from the thematic analysis.
Theme 1: benefits to mothers
This theme encompasses the views of staff regarding the effect administering the HADS has on mothers. This begins from its ease of use for mothers, with all staff interviewed identifying that on the whole, the HADS was simple to complete.
“Yeah, yeah it’s all been fine and most of the women are happy to do it as well, which is good.” Interview 1
Another benefit of the HADS to mothers was that of highlighting psychological state. Although this sub-theme also demonstrates a degree of benefit to the staff and clinical practice, it gave mothers an opportunity to express their thoughts and feelings. Staff also believed that mothers felt more supported as a result of the HADS having given them the oppor-tunity to express how they were feeling. This in turn led to mothers feeling that NNU staff were taking even more of an interest in them.
“It’s now very positive that all of the mums feel, and have actually vocalised they feel, that staff are interested in them and not just the baby and that alone is huge.” Interview 7
Both highlighting psychological state and feeling supported were found to be closely interwoven with the sub-theme of facilitating communication, which was apparent throughout the discourse. This sub-theme represented an increased awareness and willingness for mothers on the NNU to talk to maternity staff and other health professionals about any difficulties they are having.
“I think they probably feel that they’re being listened to, they’ve got extra support as well. I think sometimes they see us every day and they have to put on a brave face, and I think sometimes knowing that they can talk to somebody else outside is a good thing.” Interview 2
Theme 2: benefits to clinical practice
Benefits to clinical practice emerged across the interviews, with staff expressing various advantages of using the HADS in the NNU. It became apparent that although administering the HADS was an addition to their workload, it had generally integrated well into their routines and was now a helpful part of their general practice. These views resulted in the formation of the sub-theme ease of use for staff.
“It is extra work but it’s doable. It’s just another piece of paperwork, it doesn’t take long. It’s always documented in our handover sheet so we know when they’re due. It’s not a major thing, it doesn’t make life difficult – we just do it.” Interview 5
A further identified sub-theme improved interdisciplinary communication. Overall, staff conveyed that they were more confident in communicating with appropriate services, and that other professionals involved in the mothers’ care were aware
of the use of the HADS in the NNU. This enabled community professionals to be able to follow up with any issues that had arisen in order to continue acting accordingly.
“It is linked now, it’s not just us doing a HADS and discussing it with the woman and then sending her home. The huge benefit is the health visitors, who see the women at home, and the GPs know that we are doing it. If people are scoring, the mothers can get seen, they can have interventions early. Our women get seen within days of expressing those thoughts. Also we can document it and send it out to the GP – we feel we close the loop from our side and that’s been fab.” Interview 7
Following on from the improved interdisciplinary communication, the closely accompanying sub-theme of facilitating appropriate referral developed. NNU staff relayed that as a result of better communication and the establishment of clear referral pathways, they were now more confident in referring mothers to the Clinical Health Psychology Department.
As a result of the training that accompanied the introduction of the HADS, the sub-theme of recognising current limitations emerged. Here, several NNU staff spoke openly of the limitations of their professional role, as well as the barriers that remain in addressing the difficulties faced by some mothers. Understandably, psychological distress was not an easy subject to broach, with some mothers declining intervention. As well as recognising their current limitations, staff also highlighted past limitations and how the implementation of the HADS had made steps to address these.
“Before we didn’t really refer to anybody else, that was it – there was just a gap in the loop. Even if you knew and you could tell that this parent could just do with some help, we wouldn’t have contacted anybody.” Interview 1
Theme 3: disadvantages and obstacles
This theme fell into five sub-themes and the first was patient reluctance. This was identified in most interviews, with several staff stating that a mother declining support and intervention was a significant barrier.
“There is a group of mums who might need it but who either decline doing the test or don’t really want any kind of follow up. There are real different personalities; some want to work it out themselves or are not ready to share.” Interview 2
Another disadvantage staff identified was the negative perceptions that could surround mothers if they refused to complete the scale or if they scored high and thus were highlighted as struggling. The stigma attached to psychological distress after birth was given as a potential explanation for why some mothers may be anxious about being ‘scored’ on how they are feeling at what is undoubtedly a difficult time in their lives.
“From a personal point of view it’s another ‘big brother is watching you’ thing and I can understand why some people would be quite upset that actually you’re almost lumping them into ‘she’s a bad mother, because she’s refused her testing’ or because she has ‘done her testing and she’s quite anxious but she doesn’t want any help’.” Interview 6
The next sub-theme that emerged under disadvantages and obstacles was that of adjusting to increased workload, with the administering and scoring of the HADS inevitably increasing the already high staff workload. Although this increase was identified by all interviewees, they did however state that the extra paperwork had now become part of their daily routine and is now integrated into clinical practice.
“It’s just another thing that they do in the day and, again, that’s thanks to the support they’ve got, the training they have had to do it – it’s just been adopted into practice.” Interview 7
The last sub-theme to emerge that served as an obstacle was named test effects and validity. This involves the notion that some mothers may answer the questions on the HADS in such a way as to falsify or play down their psychological state so that they are not highlighted. Some mothers who had completed the HADS numerous times tended to stick with the answers they’d given previously, rather than completing the test as though it were for the first time and that they had to read and consider the questions and answers they gave.
“I think some of them are aware of those questions if they’ve suffered in the past from postnatal depression so I don’t think it’s a bulletproof questionnaire. I think some of them know the system and if they don’t want that help they can lie a bit.” Interview 3
Theme 4: service development
Several staff volunteered future improvements they felt would be of benefit to their clinical practice. Although the interviewees were not asked specifically about their suggestions for future development, the semi-structured nature of the questioning meant that this theme emerged from the interviewees’ ideas. Our first sub-theme was termed training needs, given that several staff identified particular areas where they felt that further training was required. This interviewee highlights how some of the less experienced staff would benefit from further training in talking about sensitive issues in particular:
“I think some of our junior members don’t like talking about feelings, opening up that can of worms. If they do it and speak to a mum who bursts into tears or scores high, I think maybe the junior or younger staff don’t know what to then do.” Interview 3
A further sub-theme that arose from the interviews was incorporating the mothers’ support network. Here several NNU staff identified the relative lack of support available to the rest of the family, particularly fathers and children.
“They come in and it’s very much about mum and the bonding and keeping that but also we do family supportive care and so often it’s the dads who go out of the building at the end of the night alone and I do feel for them sometimes.” Interview 8
The final sub-theme was the appropriateness of assessment time points. This issue was consistent across the majority of interviews whereby staff felt that administering the HADS at two days after birth was inappropriate given that the mothers are usually still recovering (emotionally and physically) from a delivery that was likely to have been a caesarean section or of a traumatic nature.
“I wonder if perhaps day two might be a bit soon for some mums that are really quite poorly after delivery. Sometimes it’s quite difficult to actually be talking that through on day two.” Interview 9
Conclusions
Five years on from the initial pilot study at SDH demonstrating the benefits of PAST for maternity staff, the current study indicates the ease with which the HADS is now incorporated into clinical practice, as well as the benefits identified for both mothers and maternity staff. While staff acknowledged that there were some difficulties in using the HADS in terms of increased workload and scheduling issues, these were often framed as somewhat minor and generally manageable. The key problems identified in administering the HADS were some mothers’ scepticism of its use and concern for the consequences for themselves and their baby should they achieve a high score. As a result, this subset of mothers held negative perceptions of the HADS and consequently avoided its use. Of course, while mothers have the right to refuse the screen, this refusal led staff to informally monitor the mother’s psychological wellbeing and use clinical judgement to assess and report any concerns.
With mothers’ reluctance having been the main concern, further considerations regarding amendments to the HADS scheduling were expressed. Throughout this study the HADS was administered routinely at two days following birth, followed by every ten days thereafter. However, multiple staff highlighted that two days following birth was not a suitable time to administer it. Assessing the mothers so early on while they remain in a potentially poor physical state, compounded by the emotional strain of having a critically ill child and hormonal changes, was not considered appropriate.
The HADS has received support from staff on the NNU at SDH who believe that it has had a significant impact on mothers. As a consequence, this will continue to be implemented on this ward as a local standard of care.
There has been significant improvement with regards to the understanding, identification, assessment and treatment of a mother’s psychological difficulties throughout pregnancy, childbirth and the postnatal period. What remains apparent is a lack of clinical support available to fathers within the healthcare approach. Several of the staff identified that fathers are of invaluable support to mothers but are sometimes overlooked. A father’s psychological wellbeing is as important as the mother’s, given that psychological distress in one or both parents can have a significant detrimental impact on the newborn baby and the family unit.16 In an era moving towards holistic family care, future research may look to expand psychological screening to fathers alongside mothers.
Acknowledgement
The authors would like to thank Zena Brit-Saunders and Hannah Gooding for their help in the interview process.
Or read this article in our
Tablet/iPad edition
- Mothers on the NNU are at greater risk of psychological distress, which can have a detrimental impact on the baby and the family unit.
- Detecting psychological distress is vital.
- Staff interviews were conducted and thematically analysed. Results showed that the HADS was beneficial to mothers and clinical practice, and helpful for identifying and enhancing access to psychological support.
Also published in Infant:
