

Anxiety: an invisible complication of pregnancy
Depression is commonly diagnosed during pregnancy and in the postpartum period. While it is largely recognised as a problem, anxiety is often misdiagnosed as depression. Anxiety during pregnancy and in the postpartum period can hinder maternal-infant bonding and manifest as an inability to cope. Pregnant and postpartum women should be screened for anxiety disorders frequently to engage in proper treatment.
Catherine A. Pankonien
Assistant Professor
catherine.pankonien@msutexas.edu
Sandra M. Groth
Assistant Professor
Cesar Alvarado
Assistant Professor
Midwestern State University, Wilson School of Nursing, Wichita Falls, Texas, USA
During pregnancy and beyond, women feel a vast number of emotions. Some of these emotional changes are due to hormones, while others are a response to the pregnancy itself.
Initially women may feel disbelief at being pregnant, hesitation, happiness, fear, elation, excitement, and worry. Throughout the pregnancy feelings can vary, depending on hormonal changes and other events happening in the woman’s life. For instance, when a woman is offered genetic testing to see if there are any anomalies, fear and uncertainty may become prevalent; pregnancy complications may cause anxiety and a sense of loss. Following the birth of a baby, anxiety can result from some of the new stressors a woman faces, such as finances or balancing the new role of motherhood. For all of these reasons, anxiety associated with pregnancy should be evaluated to help each woman reach her optimal wellbeing.
Background and significance of the problem
Along with the typical postpartum issues, for example lack of sleep, hormonal changes, stress of healing from pregnancy and delivery, caring for a new baby and worries about the wellbeing of the new baby, symptoms of postpartum depression (PPD) can be exacerbated during the first month following delivery.1 PPD is a debilitating mood disorder. Symptoms include persistent sadness, loss of interest, feelings of emptiness, low energy, changes in appetite and sleeping patterns, feelings of hopelessness, worthlessness and guilt with suicidal ideation that can occur during pregnancy or up to four weeks after birth.2
Peripartum and postpartum anxiety, however, can manifest as the inability to relax, a constant sense of worry that something bad may happen, interrupted sleep, irritability, muscle tension, forgetfulness, decreased appetite, nausea, dizziness, or a form of obsessive-compulsive disorder (OCD), including constant cleaning, counting, reordering things and a strong desire to protect the infant. Some women experiencing postpartum anxiety may try to avoid certain situations, activities, places or people. They may also need constant reassurance and may consistently be imagining the worst-case scenario, making them extra careful and vigilant of danger (TABLE 1).4
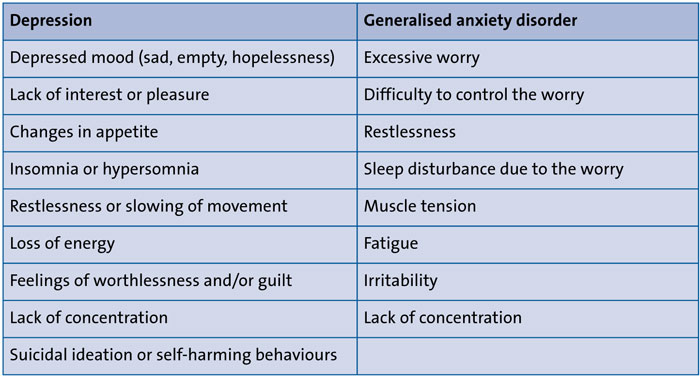
TABLE 1 Depression versus anxiety symptoms.
Anxiety is a natural process of human experience that serves as a warning system to alert danger that is known or vague. Fear, an additional warning system that responds to known threats, can manifest positive or negative decision-making and can become maladaptive and trigger unwanted physical and mental symptoms. Approximately 18% of the American population suffers from an anxiety disorder.5,6 Worldwide, anxiety affects 2.5-7% or 284 million people.7 While these numbers are significant, the number is even higher in pregnant and postpartum women. Postpartum anxiety reportedly affects 15-40% of new mothers worldwide,8 Anxiety, similar to depression, can manifest prior to pregnancy, during pregnancy, or in the postpartum period. Having a baby can be both exciting and scary. The anticipation and planning for a new baby prepares a women for motherhood, but may also come with unanticipated mental health consequences. During this time in a woman’s life, anxiety and worry about the future can often be dismissed and ignored. It must be recognised that mental illness is one of the most common maladies among new mothers. Typically, postpartum anxiety occurs within the first 12 months after delivery.9-11 The impact of anxiety on the pregnancy and postnatal period is long-lasting, leading to negative outcomes for both mother and baby. Maternal anxiety impacts the developing baby as well as the maternal-child bond. Anxiety also negatively impacts infant growth, breastfeeding, attachment, bonding, and the child’s cognitive, emotional, and behavioural development. Therefore, to promote optimal growth and development of the newborn, the mother’s mental health should be regularly assessed.
Depression has been extensively studied and a significant number of those afflicted with postpartum depression also suffer from anxiety disorder.9 However, mothers can have anxiety apart from depression. Treatment for depression may not work if the real problem is anxiety.13 Unfortunately, while postpartum depression screening is an integral part of identifying mental illness; anxiety is often not part of the screening process in postpartum mothers.10 Upon discharge, mothers are taught about ‘the baby blues’ and signs of postpartum depression, but rarely is anything mentioned about anxiety.
There is significant literature to support screening tools for detecting PPD but assessment scales to detect postpartum anxiety remain scarce. The limitation with detecting postpartum anxiety increases the probability of complications during pregnancy and may directly harm the wellbeing of the newborn infant.14 The need to have a reliable assessment tool to assist in detecting postpartum anxiety should be a part of the mental health screening process since the evidence shows a direct link between maternal wellbeing and child outcomes.14
A review of screening tools
Edinburgh Postnatal Depression Scale (EPDS)
Most commonly, the EPDS is used to screen antepartum and postpartum women for depression and comorbid anxiety. The EPDS items ask women to rate how they have felt in the previous seven days. The items include:15
- ability to laugh
- anhedonia (the inability to feel pleasure)
- guilt
- anxiety
- panic attacks
- overwhelmed
- sleep disorders
- tearfulness
- suicidal ideas.
Response categories are scored 0, 1, 2 and 3 for each item according to increased severity of the symptoms. Individual items are totaled to give an overall score ranging from 0 to 30.15 The higher the score, the more likely depression is present and the woman should be treated and/or referred for treatment as soon as possible. According to Sinesi,16 there is strong evidence to support the EPDS, which is also able to reliably detect antenatal and postnatal anxiety through a separate subscale, including items 3, 4 and 5.
Hospital Anxiety and Depression Scale (HADS)
HADS is an alternative screening tool with a ten-point scale used to determine depression and anxiety in antenatal women.17 On this scale, a total score equal to or greater than 8 is indicative of depression or anxiety. However, neither EPDS or HADS expressly screen for anxiety. The HADS scale has been found to be reliable, however, it is not specific to any one population, such as antenatal or postnatal women who are facing unique challenges.
Generalised Anxiety Disorder scale (GAD-7)
GAD-7 is used in the general population to screen for generalised anxiety. It is a seven-item, self-administered questionnaire that enquires about the degree to which the person is bothered by nervousness, irritability, feeling on edge, or worrying.18 Scores of 5, 10, and 15 represent mild, moderate or severe anxiety, respectively. The GAD-7 correctly identifies about 74% of the cases screened; it has good reliability, validity and sensitivity. Women who screen positive should be further evaluated for anxiety and possible treatment options. However, evidence indicates the GAD-2 is more effective with a sensitivity of 86%.19,20
Perinatal Anxiety Screening Scale (PASS)
PASS is a screening tool specific to antepartum and postpartum women, which takes into account the gestational or postnatal age. It consists of 31 statements that the woman ranks as feeling ‘not at all’, ‘sometimes’, ‘often’, or ‘almost always’.12 The scale has a four-factor structure, namely:21
- acute anxiety and adjustment
- general worry and specific fears
- perfectionism, control and trauma
- social anxiety.
Using this screening tool aids in identifying women with mild, moderate or severe anxiety symptoms, helping to guide treatment and increase referrals of women to the appropriate level of care.22
Postpartum Specific Anxiety Scale (PSAS)
PSAS is a scale that specifically targets anxiety in postpartum women and the types of worry from which they suffer. Due to the vulnerability of pregnant women, this screening tool was tested during the COVID-19 pandemic and assessed the frequency of maternal and infant-focused anxiety.23 This scale measures four factors:22
- competence and attachment anxieties
- infant safety and welfare anxieties
- practical baby care anxieties
- psychosocial adjustment to motherhood.
The scale comprises 51 items that measure maternal and infant focused anxiety over one week in the first year after the birth of a baby.24 To measure competence and attachment anxieties, items address anxiety related to maternal self-efficacy, parenting and the mother-baby relationship. Infant safety and welfare is measured with items related to fears about baby illness, accidents, and cot death. Practical infant care anxiety is measured with items addressing feeding, sleeping and the baby’s general routine. Psychosocial adjustment to motherhood is determined by looking at adjustments concerns related to personal appearance, relationships, support, work, finances and sleep.24 The PSAS appears to be a reliable measure of maternal mental health in the postpartum period.
Recommendation and conclusion
Postpartum anxiety and depression are recognised as common and increasing problems worldwide. According to Koukopoulos, “Assessing anxiety in prepartum and postpartum with specific scales is crucial for new mothers' mental health and newborn babies' upbringing”.21 In 2018, the American College of Obstetrics and Gynecology25 confirmed its recommendation that all obstetrician-gynaecologists and other obstetric providers complete a full mental health assessment, including screening for depression and anxiety, during each post-partum visit, for each patient. Thus, it is essential to utilise a valid screening tool to identify women in need, so that treatment and referrals for mental health care are offered and recommended. Furthermore, the National Institute for Health and Care Excellence (NICE) recommends the GAD-2 screening tool, because it is effective in the general population.16,26
In conclusion, all women should be screened for anxiety and depression in the antepartum and postpartum periods. The screening tools must be specific to the ante- and postpartum periods, not generalised tools for any population. The EPDS is specific to depression and the postpartum period. The PSAS and the PASS are both specific to anxiety and are useful in differentiating anxiety from depression. When appropriate scales are employed, proper diagnosis and treatment can begin quickly. When a woman is suffering from an anxiety disorder, treatment for depression is not effective.13
Or read this article in our
Tablet/iPad edition
- Anxiety is often misdiagnosed as depression and treatments may not work effectively.
- Postpartum anxiety can negatively affect the maternal-infant bond and subsequently breastfeeding.
- Healthcare professionals can support pregnant and postpartum women by recognising the difference between anxiety and depression and providing education and support for women to seek help.
Also published in Infant:
