

Getting it right – the critical window to effectively establish lactation
Globally, only 41% of infants are exclusively fed human milk for the first six months of life. Healthcare providers need to change the practice paradigm and initiate a pro-active approach for the establishment of milk supply.
Diane L. Spatz
PhD, RN-BC, FAAN
Professor of Perinatal Nursing and the Helen M. Shearer Professor of Nutrition, University of Pennsylvania School of Nursing, and Nurse Scientist for the Lactation Program, Children’s Hospital of Philadelphia, USA
spatz@nursing.upenn.edu
Human milk and breastfeeding are the preferred form of nutrition for all infants, yet in the USA and elsewhere in the world breastfeeding rates continue to be suboptimal. The Centers for Disease Control and Prevention (CDC) report that in the USA 83% of women initiate breast-feeding but only 25% of infants receive exclusive human milk for the first six months.1 In 2018, the United Nations Children’s Fund (UNICEF) and the World Health Organization (WHO) released two significant reports which underscore that suboptimal breastfeeding rates are a major public health concern.2,3
Only 42% of infants are breastfed within one hour of birth.3 The lack of exclusive breastfeeding under six months is alarming, with only 41% of infants globally receiving exclusive human milk.3 Breast-feeding is one of the most effective ways to protect both child and maternal health and provide for optimal child development and health.2
It is important to note the global focus on human milk and breastfeeding is, and has always been, on the presumed healthy mother-infant dyad. There exists no international database on human milk and breastfeeding rates for vulnerable infants (preterm infants, infants with birth defects, term infants with complications, or other infants separated from their mothers at birth). These are infants who could most benefit from human milk but are at high risk for not receiving it.4
WHO released a significant report in 2017 stating that the Baby Friendly Hospital Initiative (BFHI) has not been effective in improving human milk rates globally.5 Based on this landmark report, WHO released new guidelines for the BFHI that expand the scope to address the needs of preterm infants and also remove the restriction on the use of bottle teats and pacifiers.6 While the new BFHI guidelines are improved they do not address the needs of other vulnerable infants, there is no clear definition of the need for technology when mother and infants are separated and there is not specific language about human milk as a medical intervention. I would recommend that healthcare providers consider using the model I developed to protect and promote human milk and breastfeeding for vulnerable infants, which has published research outcomes.4,7-11
Given the above introductory information, there is great opportunity to improve the landscape of breastfeeding worldwide. I believe that a paradigm shift is essential to effectively increase human milk rates not just for the short-term (initiation) but for the long-term (exclusivity and duration rates). Healthcare providers need to change the current practice paradigm. The two most essential paradigm shifts that must occur are:
- appropriate prenatal anticipatory risk assessment with appropriate education and guidance to the mother and her family about how to get the best possible start to lactation
- creating a sense of urgency about the establishment of milk supply.
Anticipatory risk assessment, education and guidance
During prenatal care it is essential that the healthcare provider conducts a thorough assessment to determine potential risk factors that could impact the mother’s breastfeeding experience and her ability to develop a copious milk supply. There are multiple risk factors that can be assessed antenatally (TABLE 1). In the USA and around the world more women are delaying childbirth so it is likely that many healthcare providers will be caring for women who are over the age of 30 and a primipara.12 Obesity rates are also growing globally and women with a body mass index (BMI) over 30 are at risk for delay of lactogenesis II and breastfeeding cessation.13 If risk factors are identified, the more the risk, the more the sense of urgency healthcare providers should have about the establishment of milk supply.
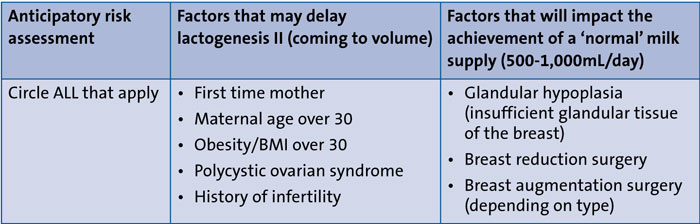
TABLE 1 Prenatal lactation risk assessment.
As healthcare providers, we should be having open and transparent conversations with the mother and her family members about potential risk factors that can have negative impact on the establishment of milk supply. This should not be viewed as a ‘scare tactic’ for the family to think they will not be able to provide milk for their child. It is helping families make informed decisions so that they are aware of risk and can proactively manage that risk in order to come to full volume.
If mothers have conditions such as prior breast surgery (especially breast reduction) or glandular hypoplasia (insufficient glandular tissue), healthcare providers must provide appropriate anticipatory guidance. These mothers should not expect to be able to achieve a ‘normal’ milk supply. Strategies should be employed from birth to help these mothers maximise their personal milk making capacity.14 For these mothers, the use of technology is essential. They should be encouraged to rent the hospital grade pump at the time of birth and to utilise a baby weighing scale in order to measure milk transfer.15 In such cases, mothers should be counselled that any amount of milk is a lifesaving medical intervention. There are components in human milk that will never be present in infant formula.12 Every drop of milk that they can produce for their child should be valued and celebrated.
Pro-active management to ensure coming to volume
Following delivery of the placenta, the levels of oestrogen, progesterone and human placental lactogen rapidly decline and this allows the mother to convert from lactogenesis I (secretory activation) to lactogenesis II (secretory differentiation).
If a mother presents with prenatal risk factors, it is essential for us to have a sense of urgency about milk supply. Even if the infant can latch on and suckle, these mothers should be advised to initiate milk expression with a hospital grade pump with ‘initiation technology’ (eg Symphony, Medela) in order to facilitate the establishment of milk supply and increase access to colostrum. Research on this technology demonstrates that:16,17
- the colostrum can be removed more effectively
- more colostrum is available for the infant
- the mother comes to full volume faster.
If the mother has a presumed healthy infant but presents with antenatal risk, the number one priority has to be the establishment of milk supply. In addition to breastfeeding, she should also be instructed to pump after breastfeeding as many times per day as feasible using the pump’s initiation setting. For the first week, the mother’s only focus should be to eat, sleep and breastfeed/pump for her infant. Family support should be mobilised.
It is essential to pump as soon as possible following delivery in order to ensure coming to volume.15,18,19 The goal is to pump within the first hour after birth. If this is not feasible, milk expression should commence before six hours post-delivery. If the mother has a presumed healthy infant, she should be holding her infant skin-to-skin immediately after birth and for as many hours a day as feasible. She should breastfeed within that first hour and pump afterwards to facilitate coming to full volume. For infants that are unable to effectively latch on and suckle, the priority must be pumping early and often.
The mother should be instructed to always pump both breasts simultaneously – double pumping (FIGURE 1). Double pumping leads to higher prolactin levels, better release of oxytocin, and improved breast emptying which means we also will have richer, creamier milk for the infant once the mother comes to full volume.20

FIGURE 1 Double pumping.
It is also important to remember that there are intrapartum and postpartum factors that can negatively impact development of milk supply. Mothers who received magnesium sulfate during labour and delivery for pregnancy-induced hypertension, and/or had interventional deliveries (eg induction, intravenous fluids, operative delivery) have been reported to experience problems with milk supply and delay in lactogenesis II.12
If the mother and infant are separated for any reason post-delivery, milk expression with the hospital grade pump with initiation technology has to be prioritised. Mothers need to pump early and pump often.15 Research demonstrates that pumping within the first hours is critical for coming to volume. The earlier the mother pumps the more likely she will have more milk in the first week and in subsequent weeks. When working with healthcare providers in many countries to implement my 10-step model, I have focused on pumping initiation immediately after birth – the critical first four days and first 14 days of pumping (TABLE 2). This focus of early frequent pumping has led to substantial improvements in human milk rates at discharge and beyond.4,7-11,21
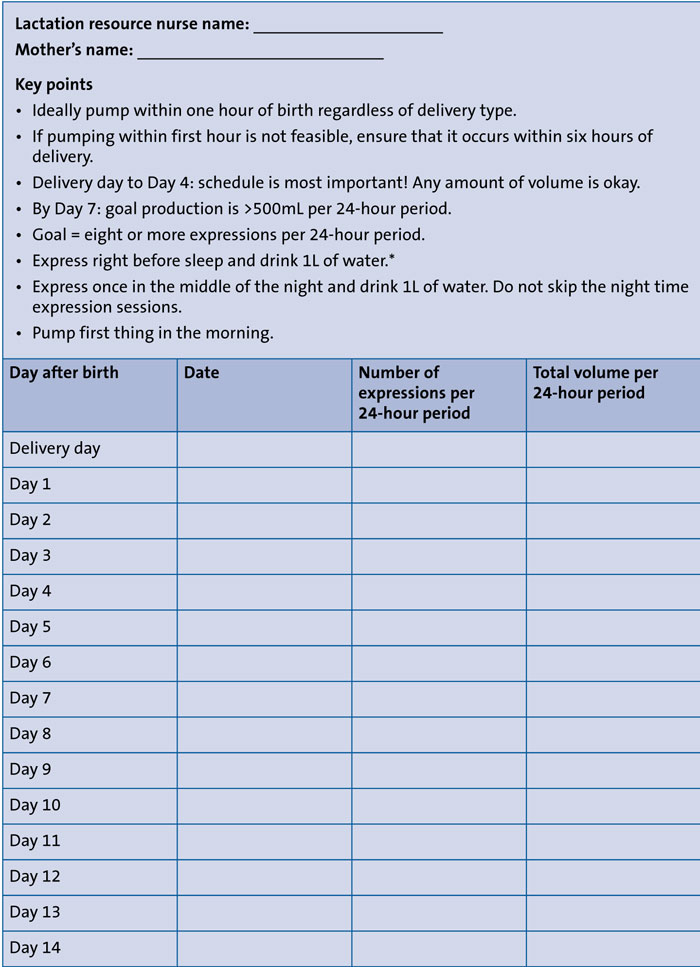
TABLE 2 Coming to volume data collection tool. *Drinking 1L of water before sleep and in the middle of the night ensures the mother wakes up to urinate and express. It also keeps her hydrated.
Summary
Healthcare providers need to change the current practice paradigm. Routine antenatal assessment for risk factors related to lactation is essential. Healthcare providers should have open and honest conversations with families prior to delivery. We must adopt a proactive management style to ensure that mothers come to full volume.
Or read this article in our
Tablet/iPad edition
- Both mothers and infants can have risk factors that may impact the ability for a copious milk supply to be achieved.
- Healthcare providers should conduct an antenatal risk assessment for maternal lactation risk factors that could impact milk supply.
- Healthcare providers should employ a pro-active management style to ensure that a mother comes to full volume (500-1,000mL/day) by Day 7 post-delivery.
Also published in Infant:
