

Sepsis and central line-associated neonatal infection: a care bundle QI project
Neonatal late-onset sepsis (LOS) is a significant cause of mortality and morbidity within neonatal units. These infections are often associated with the insertion and use of central lines. Data from 2017 identified the local neonatal unit at Gloucestershire Hospitals NHS Foundation Trust as an outlier with above average rates of LOS. A quality improvement (QI) project was therefore created with the aim of reducing rates of central line-associated sepsis.
Rowena Craig
MB BChir, MRCPCH
ST6 Registrar
Simon Pirie
MBBS, MRCPCH
Neonatal Consultant
simon.pirie1@nhs.net
Michellee Grant
MSc ACP
Senior Advanced Neonatal Nurse Practitioner
Neonatal Unit, Gloucestershire Hospitals NHS Foundation Trust
Neonatal LOS is a significant cause of morbidity and mortality with neonates developing signs of septicaemia, pneumonia or meningitis.1,2 For patients in a neonatal unit setting, this may represent nosocomial infection and lead to prolonged hospital stays and increased financial costs.2,3
Studies show that the causative organisms in 50% of neonatal LOS cases within the neonatal unit are coagulase negative staphylococci (CoNS). Other organisms implicated include Staphylococcus aureus, Enterococcus, Streptococcus, Escherichia coli, Klebsiella and Pseudomonas.4,5
Premature and low birthweight neonates are at increased risk of LOS because of immunological immaturity and a hospital environment that includes frequent invasive medical procedures and the routine use of central lines to administer medication and parenteral nutrition.4-10
In 2017 routine data collected via the BadgerNet system identified our unit as an outlier, with an above average number of cases of culture-positive neonatal LOS. In view of this, a QI project was designed and implemented with the aim to reduce LOS and positive culture rates.
This project has been multidisciplinary with particular focus on developing sound aseptic technique and care bundles to improve the process of central line insertion.
Evidence
Key steps in reducing rates of neonatal LOS and central line related bloodstream infections include meticulous attention to hygiene, minimising invasive procedures and improving the insertion and care of central lines.3,4
Care bundles are one method of achieving this and are defined as a limited number of specified practices implemented simultaneously.11 Bundles have been shown in multiple settings to reduce rates of central line related bloodstream infections and even subsequent rates of neuro-disability.11-16 The overall aim in these settings has been to ameliorate the impact that neonatal care has on the neonatal microbiome, which is influenced by the clinical environment, use of antibiotics and altered feeding patterns.17-22
Various interventions have been included in care bundles relevant to neonatal LOS. These include but are not limited to:
- targeting hand hygiene
- improving and standardising barrier precautions for central line insertion
- improving skin and hub decontamination
- using the aseptic non-touch technique (ANTT)
- frequent staff training and feedback
- improved documentation of procedures
- early introduction of breast milk
- stringent antibiotic use.18-23
Aim and methods
The aim of the QI project was to reduce the incidence of sepsis in the neonatal unit at Gloucestershire Hospitals NHS Foundation Trust.
Central line sepsis bundle
Our local tertiary centre had recently published its experience of reduction in sepsis episodes, having incorporated a care bundle into practice12 and so we adapted its template to one that would suit our unit.
Changes implemented as a result of this included the choice of cleaning solution used prior to central line insertion. Previously we used 0.02% chlorhexidine for peripheral and central catheter insertion; in the care bundle we used:
- 0.05% chlorhexidine gluconate (Unisept) for babies born at <28 weeks’ gestation.
- 2% chlorhexidine gluconate with 70% isopropyl alcohol (ChloraPrep) for babies born at ≥28 weeks’ gestation.
We found that use of appropriate hand-wash was variable among practitioners; this was felt to be partly because the correct solution was difficult to find and not always readily available. We therefore purchased wall-mounted dispensers and ensured that the appropriate solution – 4% chlorhexidine gluconate (Hibiscrub) – was available at several sinks throughout the unit and near to the intensive care beds where staff are more likely to scrub prior to inserting central lines.
Using the template from the tertiary centre, a local checklist was created (FIGURE 1). This would act as a prompt to ensure that the person inserting the central line was assisted and observed in maintaining aseptic technique throughout. The presence of a checklist, which would then be filed in the patients notes alongside the existing proforma (FIGURE 2) would, we hoped, work to standardise practice and improve aseptic technique.
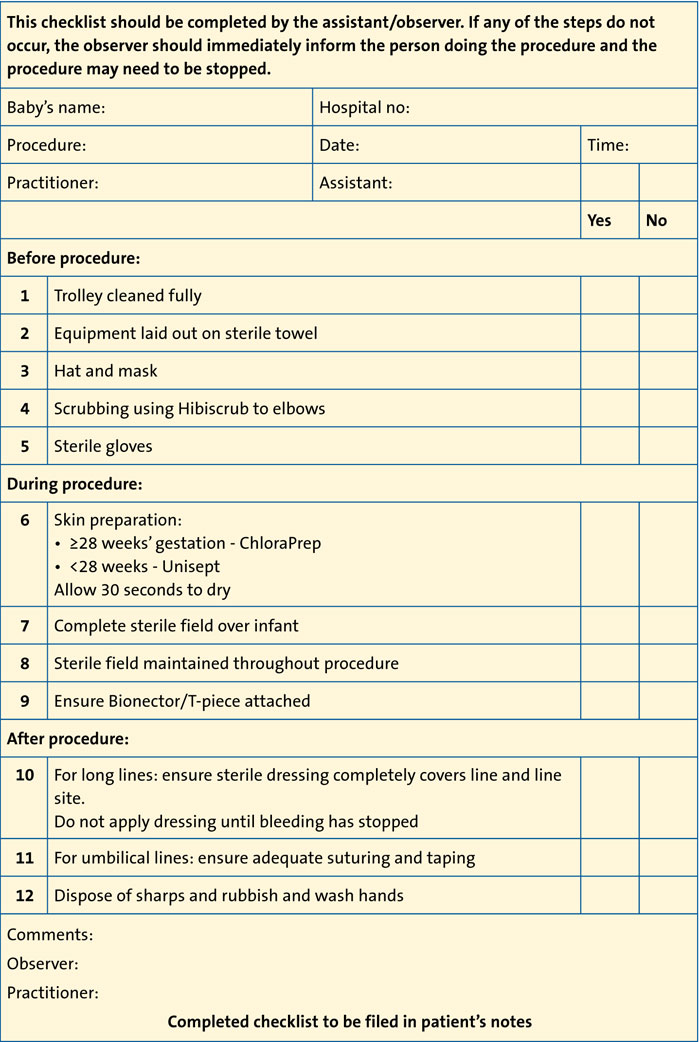
FIGURE 1 The neonatal central line insertion checklist.
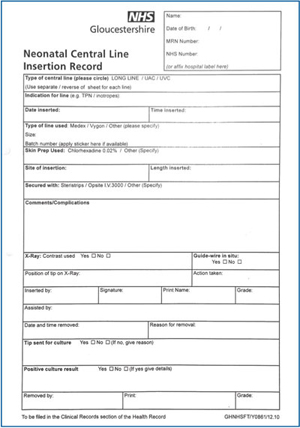
FIGURE 2 The existing proforma.
Aseptic technique
One high-risk area identified locally and in the literature was the frequent accessing of central lines for the administration of fluids and drugs.10 We therefore worked to improve care of central lines and devel-oped a teaching package. This was formulated using an adapted standard operating procedure from the ANTT direct observation of procedural skills competency assessment documents. This teaching package was then delivered to new members of the team (both medical and nursing) as part of induction and implemented regularly as a part of a continuing professional development programme.
Reviewing use of central lines
We surveyed hospitals in the network to try to understand whether units were minimising peripheral cannulation by giving antibiotics and drugs via central lines. None of the respondents were using central lines for medications on a routine basis because of the risks associated with such frequent access to central lines.
Audit and results
In order to examine the efficacy of the interventions, an audit examined positive blood cultures from babies with central lines in situ. Data from quarter one (January to March) of 2017 (pre-intervention) were compared to data from quarter one of 2018 (post-intervention).
BadgerNet was used to create a list of eligible babies who had a central line inserted in the neonatal unit within the relevant time period. This included the majority of babies less than 32 weeks’ gestation or with a birth weight below 1,500g. In addition any babies who had been recorded as having an umbilical line or peripherally inserted central line (PICC) were included. As a result of these para-meters a few term babies were included.
In 2017, 25 babies were audited and in 2018 34 babies were included. Features of the two groups are shown in TABLE 1.
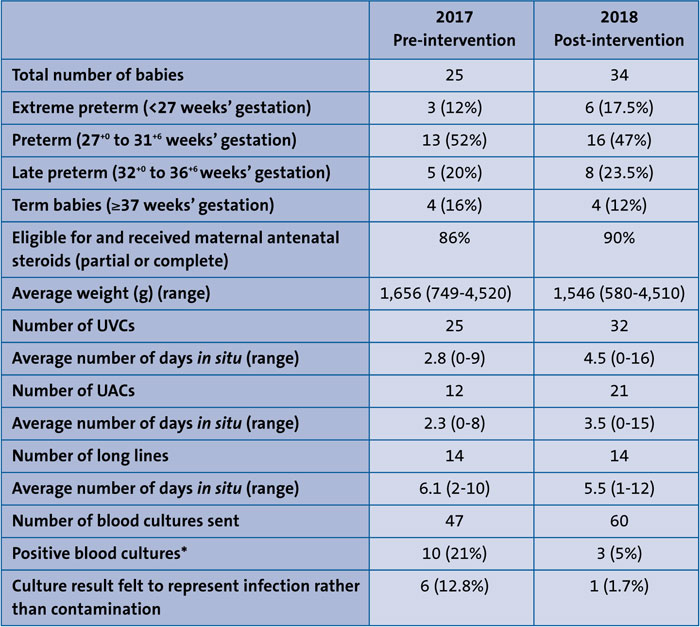
TABLE 1 Features of the two audited groups. *The total of 13 positive cultures were from 10 different babies. Three babies had two positive cultures each. Key, UVC = umbilical venous catheter, UAC = umbilical arterial catheter.
Positive blood cultures
The organisms grown from the positive blood cultures were:
- Staphylococcus haemolyticus (two occasions)
- S. epidermidis (four occasions)
- non-specified CoNS (three occasions)
- Klebsiella (two occasions)
- E. coli (one occasion)
- Enterococcus faecalis (one occasion).
Not all of these positive cultures occurred in the context of infection. On six occasions it was decided by the clinicians at the time that the culture represented a contaminated sample. For the purposes of the audit this was analysed based on the documentation made in the notes, the C-reactive protein peak and trend, and the length of antibiotic course given. Therefore on seven occasions the positive culture was felt to represent a definite episode of sepsis. Of note, six of these occurred in 2017 and one in 2018. The cases are described in TABLE 2 and the organisms in these cases reflect descriptions in the literature.5
TABLE 2 shows that in four cases positive cultures were associated with the presence of central lines. These occurred only in 2017. Six babies (five in 2017) underwent a lumbar puncture during their stay. Three of these had positive blood culture results. No cases of bacterial meningitis were detected.
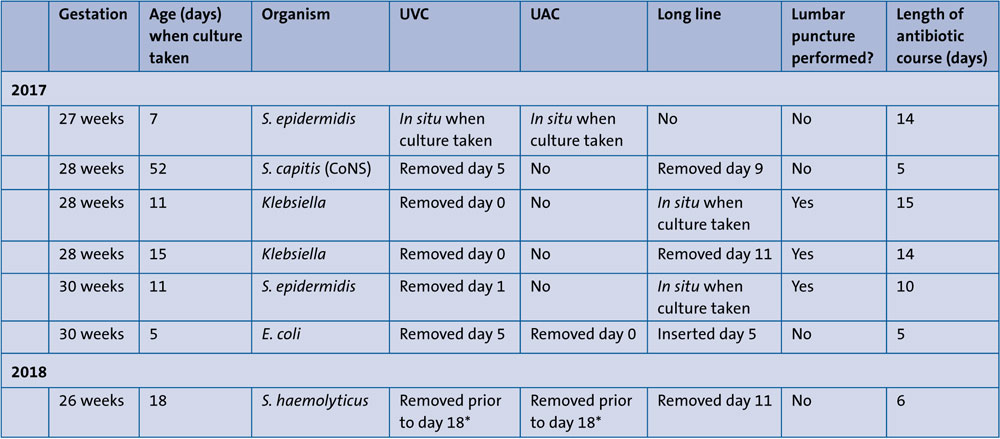
TABLE 2 Features of the seven babies with culture-positive sepsis. *The line was removed in another unit so the exact date is unknown.
Discussion
A checklist was implemented as part of a training package and QI project and was available on the unit for practitioners to use. However, it was not always found in the medical notes when practice was subsequently audited and was sometimes only partially completed, eg the assistant's name was not documented. Despite the introduction and promotion of a checklist, paperwork was completed more thoroughly in 2017 compared to 2018 (TABLE 3) yet the rates of positive blood cultures fell in this time. The improvement in positive blood culture results is not reflected in more accurate documentation of line insertion, including details of use of an assistant or use of the checklist. This might suggest that the decrease in infection rates was not related to the need to complete a form, rather that staff are taking the required actions but simply not documenting their new improved practice. Further audit work is required.
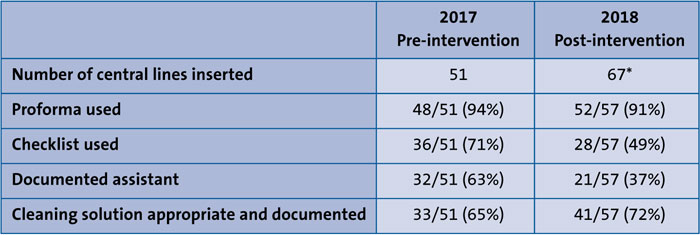
TABLE 3 Documentation of practice. *Ten sets of notes were unavailable.
Conclusions
This QI project has resulted in a reduction in the number of positive blood cultures within our neonatal unit within a year. This is encouraging and has occurred despite caring for a greater number of babies, taking more blood cultures, and siting and accessing more central lines. This suggests that working to care bundles and improving aseptic technique is, in our setting, effective.
The adoption of a care bundle related to central line care can be effective in reducing morbidity and mortality of the vulnerable preterm neonatal population.
Or read this article in our
Tablet/iPad edition
- The introduction of a care bundle and a multidisciplinary approach resulted in reduced rates of central line-associated sepsis.
- Key changes included a focus on meticulous asepsis when accessing lines and observation of central line insertion.
- These changes, among others, resulted in a reduction in the number of positive blood cultures on our unit within a year.
Also published in Infant:
