

Developmental dysplasia of the hips: a three-year cross sectional study of hip screening in Leeds
This retrospective review considers the number of infants screened for developmental dysplasia of the hips (DDH) as per national guidance, and the incidence of actual pathology at Leeds Teaching Hospitals NHS Trust over a three-year period. Approximately 10% of infants required an ultrasound scan; 3% of scans showed evidence of DDH. Of those diagnosed with DDH and referred to orthopaedics, 93% were actively treated with a harness or surgery. The significance of ‘clicky’ hips in DDH is discussed.
Aoife Hurley1
MBChB, MRCPCH
ahurley@doctors.org.uk
Sabrina Bhattacharya2
MBChB
Georgia Ford2
MBChB
Hannah Shore1
MBChB, MRCPCH, MD
Kathryn Johnson1
MBChB, FRCPCH
1Leeds Teaching Hospitals NHS Trust
2University of Leeds Medical School
DDH: what is already known?
- DDH has an incidence of 1-3 per 1,000 infants.
- It is screened for in the Newborn Infant Physical Examination (NIPE).
- Positive findings on examination need an ultrasound (US) scan in two weeks and orthopaedic referral.
- US by six weeks is needed for those with breech presentation after 36 weeks or at time of delivery, multiple pregnancy where one infant is breech or positive family history.
- Clicky hips are not an indication for US, as per NIPE guidelines, and should be reviewed as per local policy.
Background
DDH, previously known as congenital dysplasia of the hip, is a spectrum ranging from mild acetabular dysplasia with a stable hip through to more severe forms of dysplasia with neonatal hip instability.1 Given the range of presentations it is a complicated definition, but it is accepted that dislocation or subluxation can lead to dysplasia of the hip.2 The incidence of infants with this needing treatment is thought to be 1-3 per 1,000 infants.3 If undetected or treatment is delayed, there can be serious long-term health implications such as walking difficulties, osteoarthritis and surgery. An estimated 9% of primary hip replacements are due to DDH. Even after surgery, patients can still develop radiological evidence of avascular necrosis in these joints.4 Early detection and intervention is key in improving health outcomes and trying to reduce the need for surgery.1
In the UK, the NIPE screening programme, led by Public Health England as part of the national screening prog-ramme, advises all newborns should be examined within 72 hours of birth and again at 6-8 weeks of age in the community. It also recommends hip US for any infant who has a first degree relative with DDH needing splint, harness or surgery.
A second risk factor is breech presentation at or after 36 weeks. In multiple births where one baby is breech, all should be scanned. These infants should have a scan at six weeks post-term. The final criterion for US is any screen-positive infants. These include palpable clunk with Ortolani or Barlow manoeuvres, difficulty abducting hips to 90 degrees and leg length discrepancies. These infants should be scanned within two weeks and seen by the orthopaedics team if the clinical findings correlate. Clicky hips with no other risk factors should be managed as per local guidelines and do not merit an automatic hip US, as per NIPE.
One method of categorising the degree of dysplasia is using Graf grading (from I-IV), which uses alpha and beta angle hip measurements as well as the age of the child. An alpha angle demonstrates the depth of the acetabular roof and the beta angle, which is more variable, demonstrates the femoral head cartilaginous cover.5 Grade 1 is normal, with an alpha angle greater than 60 degrees. Grade IIa has an alpha angle of 50-59 in infants less than three months of age and is usually an immature hip that will normalise. Grade IIb is similar to grade IIa but in a child older than three months. Grade IIb onwards is classified as an abnormal hip and Grade III and IV are increasingly severe with an alpha angle less than 43 degrees.6
At Leeds Teaching Hospitals NHS Trust, the Pavlik harness is used as first line for DDH requiring treatment, with milder cases simply being observed. The Pavlik harness is successful in treating 80-97% of cases and US is used regularly throughout treatment to monitor progress.7-11
There has been a screening programme in the UK since 1969.12 The optimum screening programme and need for screening itself for DDH is debated among clinicians. There are countries similar to the UK in their approach, such as the USA whereby infants are examined and ultra-sound used if risk factors are identified.13 Other European countries such as the Netherlands, Germany and Austria routinely ultrasound all their infants.
Objectives
The aims of this work included ascertaining how many infants were being screened locally for DDH as per national guidance, and what the evidence of actual pathology within the screened groups was.
We were also keen to establish what the rate of DDH was in infants with clicky hips to evaluate if they genuinely merited US screening or not.
Methods
A retrospective cohort study was conducted using the Leeds Teaching Hospital’s NIPE system, identifying infants born between 1 January 2014 to 31 December 2016 who required US, as per NIPE guidelines. The inclusion criteria were being born within these dates at Leeds Teaching Hospitals NHS Trust and needing a scan based on NIPE and local protocols. There were infants who had more than one reason for needing a scan, for example being breech presentation with positive examination; these were counted in both categories, which explains the discrepancies in the figures quoted in the results section. Exclusion criteria included infants with skeletal deformities or neural tube defects as we felt these added pathologies could skew the data.
We used the local IT system and radiology reports to view scan results that were classified as normal, immature which then normalised on subsequent scans (Graf grade IIa) or evidence of DDH. Electronic patient records were then used to see subsequent follow-up and plans.
Results
29,894 infants were born locally during the period 1 January 2014 to 31 December 2016 (FIGURE 1). Of these 3,095 (10.3%) required a scan with 2,704 (9.0%) subsequently having a scan. Of those that missed scans, 153 (5%) were not brought to their scan and 238 (8%) did not have a scan requested. Overall 2,288 (85%) of first scans were normal, 351 (13%) immature and 87 (3%) had evidence of DDH.
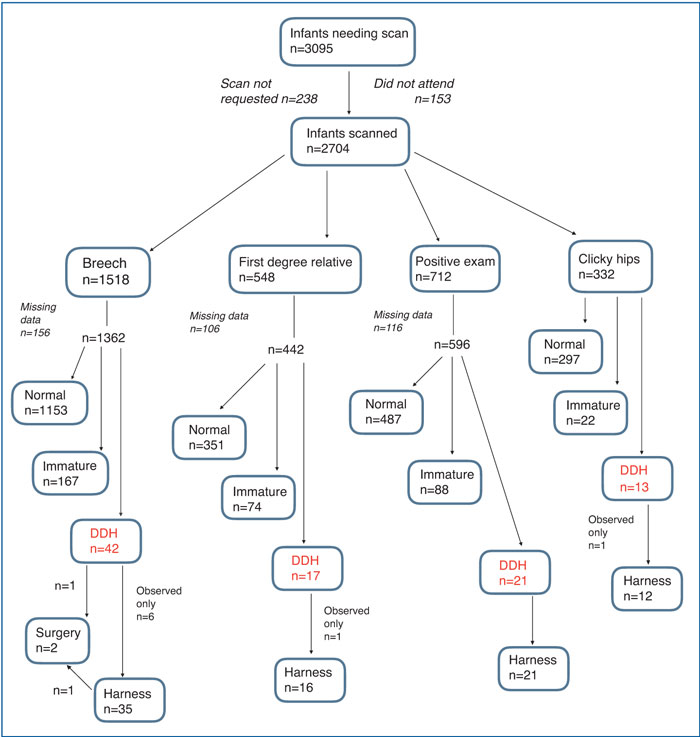
FIGURE 1 A flow chart summary of the results of the study. Note, some infants had more than one reason for a scan.
Bearing in mind that some infants had more than one reason, the reasons for a scan comprised breech infants (56%), positive examination (26%), family history (19%) and solely clicky hips (12%) (FIGURE 2). Our sonographers used alpha angle measurements only to assess dysplasia. All those with abnormal hips or immature hips that had not normalised on follow-up scans were referred to orthopaedics. Of the 87 infants with DDH referred to orthopaedics, 81 (93%) needed some form of orthopaedic intervention either harness or surgery (TABLE 1). 99% (80 out of 81) needed Pavlik harness treatment. Six cases were just observed and one case went straight for surgery as diagnosed late. In total, 2.3% of those with DDH had surgery (two out of 87).
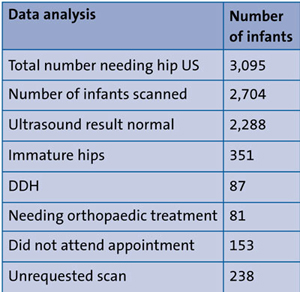
TABLE 1 A summary of the findings.
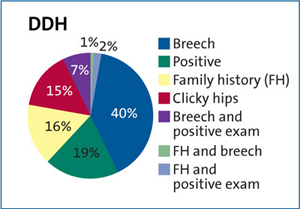
FIGURE 2 A breakdown of findings for those infants having evidence of DDH on the first scan (n=87).
The largest group scanned was breech infants; this includes those who were singleton breech or multiple pregnancy breech. They accounted for 56% of scans; of those, 3% had DDH (FIGURE 3). Positive examinations accounted for 712 (26%), 88 (15%) were immature and 21 (4%) had DDH (FIGURE 4). Those with a family history were 548 (20%), 74 (17%) were immature initially and 17 (4%) had DDH (FIGURE 5).
Some infants had several reasons for fulfilling the screening criteria, eg family history and breech, which is reflected in infants per group amounting to more than the total infants.
We were particularly keen to establish the pathology in the group with clicky hips. We found 332 (12%) infants whose sole reason for a scan was clicky hips, with 13 (4%) having DDH and 12 (92%) needing harness treatment (FIGURE 6).
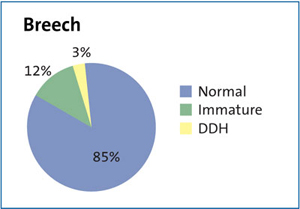
FIGURE 3 Breech infants (including those who were singleton breech or multiple pregnancy breech) accounted for 56% of scans. Of these, 3% had DDH.
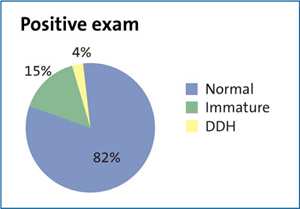
FIGURE 4 Positive examinations accounted for 712 (26%) of scanned infants. 88 (15.0%) were immature and 21 (4%) had DDH.
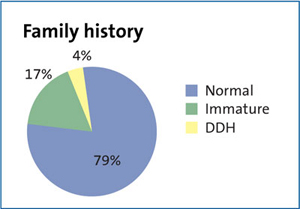
FIGURE 5 Those with a family history were 522 (19%). Of these, 74 (17%) were immature initially and 17 (4%) had DDH.
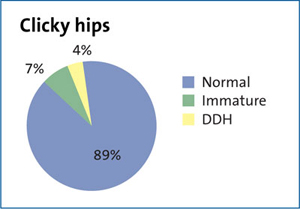
FIGURE 6 Of 332 (12%) infants whose sole reason for a scan was clicky hips, 13 (4%) had DDH and 12 (92%) needed harness treatment.
Limitations
Almost 8% of those identified as needing a scan by NIPE (238 out of 3,095) did not have a scan requested. We went through all patient notes on the list generated by NIPE to see if scans had been performed and, if not, whether we could see a request on the system. Of the missed scan requests, 49% were breech infants and 27% had a positive family history. Most worryingly, 20% had unilateral positive exam findings and 4% had bilateral findings. This could be clicky hip and not DDH, but nevertheless, this omission is a concern.
There are some missing data due to scans not being requested at the time, but these have been subsequently requested and included if available and appropriate. Some scans were not performed by the time the data were collated. This study shows the importance of being able to utilise the NIPE system to quality assure the screening programme as this cohort of infants can easily be identified. Prior to adopting NIPE it was almost impossible to identify this population of infants. Our ‘was not brought’ rate of 5% for appointments is not outside the expected rate for such a programme. While not paediatric specific, figures have been quoted at up to 8.95% ‘was not brought’ rates.14 Allowing for the missed requests as well as those not being brought to their scan appointments will affect the true rate of DDH. This review focuses on those identified on the first check that required a US scan; it does not include those found to need a scan at the 6-8 week check or indeed later on in life. Further work could be done looking at those presenting to orthopaedic clinics later and why there is a delay in presentation and potential treatment.
Conclusions
Close to 30,000 infants were included in this study with 10.3% requiring US as per NIPE guidance; 85% of scans were normal, 3% had evidence of DDH. Of those diagnosed with DDH and referred to orthopaedics, 93% were actively treated with a harness or surgery.
This study found that the risk factors laid out by NIPE for DDH, indicating a hip scan is required, were appropriate.1 The rate of DDH in our screened population (which does include mild to moderate cases) was 2.9 per 1,000 infants, which is higher than suggested by NIPE at 1-2 per 1,000.1 This suggests a higher pick up rate within our local trust, however the incidence of DDH and treatment rates may differ between trusts because of different diagnostic criteria and/or different treatment guidelines. These findings may reflect how via the NIPE programme we are better able to identify all infants needing screening, which might not have been possible before now.
The risk of DDH for an infant with clicky hips was similar to those who were scanned due to breech presentation or having a significant family history. Because of this we would recommend screening infants with clicky hips, however, the definition of clicky hips is examiner-dependent and therefore variable and this will need to be interpreted with caution as ‘clicky’ could range from a benign click through to a dislocatable clunk. This brings with it further cost implications, further pressures on existing services and a treatment that is not without risk with iatrogenic avascular necrosis affecting 1% of treated children.4
Or read this article in our
Tablet/iPad edition
- The rate of DDH cases in our population was 2.9 per 1,000 infants.
- We found the rate of DDH in infants with clicky hips is similar to those with a breech presentation or with a family history of DDH.
- This study would recommend routine scanning for those with clicky hips.
Also published in Infant:
