

The development and impact of the ENNP role in the NICU
The impetus for change in neonatal staffing structure remains constant and, as in all areas of nursing today, roles are evolving to meet the changing needs of our workforce and service users. This article will discuss the challenges and impact of developing an enhanced neonatal nurse practitioner (ENNP) tier within a busy neonatal intensive care unit. It will highlight issues that other neonatal services may relate to and offer solutions to achieve this goal.
Jessica TalbertRN(Child), BSc(Hons) Health Studies, PGCE, MSc Health Care and Educational Practice Neonatal Module Lead
Diane Keeling
RN(Child), BSc(Hons) Health Studies, PGCE, MSc Neonatal Studies
Advanced Neonatal Nursing Practitioner/ Neonatal Module Lead
University Hospitals Plymouth NHS Trust
neonatalmoduleteam@plymouth.ac.uk
The 1990s saw the emergence of the ENNP and advanced neonatal nurse practitioner (ANNP) roles in the UK. However, while the ANNP role became widely established and recognised in national documents as part of quality neonatal services, the ENNP role is arguable less well-defined and has only more recently been highlighted within national standards as part of the neonatal workforce.1 Nevertheless, there are some areas, such as the north west of England, where the role of the ENNP has thrived.2
University Hospitals Plymouth NHS Trust strives towards having ‘the right staff with the right skills, in the right place at the right time’3,4 to provide high quality neonatal service provision. Over the last 20 years Plymouth neonatal unit has nurtured a robust ANNP team, a development further supported by the Department of Health’s Toolkit for High Quality Neonatal Services in 2009.5 The ANNP team contributes towards the tier 1 and tier 2 medical rotas to maintain consistent high quality care, supporting both the medical and nursing team. However 20 years on and despite having a team of ANNPs, the Plymouth NICU faces similar challenges to other neonatal units in that there is a persistent lack of junior medical staff and the subsequent use of locum doctors results in inconsistent care delivery. The situation was further challenged by the actual and impending retirement within the current senior nurse and ANNP workforce. To address the issue there was an unsuccessful attempt to recruit more qualified ANNPs and therefore, trainee ANNP posts were advertised to once again ‘grow our own’.6
There were, however, challenges to internal recruitment as there was a largely junior neonatal nurse workforce. The tier of very experienced senior neonatal nurses, which had previously been available, had either moved into other roles or retired, leaving a noticeable gap in experience within the team. This reduced the number of staff ready to undertake ANNP training. There was also a reluctance of experienced qualified in specialty (QIS) staff to undertake the leap to ANNP training due to the desire to remain in nursing care roles, the fear of academia and increased clinical responsibility. In addition the ward manager was understandably reluctant to release the most experienced QIS staff due to a perceived loss to the nursing workforce. Hindering potential ANNP trainees further was the limited national availability of training courses. The geographical location of Plymouth to the nearest ANNP training centre was unappealing to many of the nursing staff who had commitments within the south west. As a result, despite having an established ANNP team, there still remained challenges in delivering high quality neonatal services due to:
- the persistent lack of medical staff
- retirement within the senior nurse and ANNP teams
- a reluctance of QIS staff to undertake ANNP training and of nurse managers to release experienced nurses.
A review of staff numbers and workload identified that even with a full complement of staffing, at times there were insufficient staff numbers to meet clinical demand. During the day the medical team consists of a tier 1, tier 2 and consultant solely covering the neonatal unit. However out of hours, in addition to the busy NICU, the tier 1 and tier 2 cover postnatal wards, a large transitional care ward (TCW), delivery suite and community referrals, with a consultant on call. On busy shifts this staffing is insufficient to maintain timely care to the neonatal population. However, it became evident that NICU nursing staff at the bedside were consistent in number, both day and night with approximately 10 staff per shift.
The workforce plan was therefore reviewed for possible solutions and the consistent nursing staff numbers meant there was a potential for the nursing team to support the medical staff. Identified within the Toolkit5 is the role of the critical care nurse (CCN). Although this role is not clearly defined it refers to nurses with enhanced skills, which was identified as a possible solution to maintain safe and efficient care. The initial interpretation of this role was that the CCN should attain additional clinical skills to support the medical team as required, acquiring non-accredited, in-house training. Their workload would remain at the cotside of allocated infants and they would be included in the QIS numbers, thus remaining within the nursing workforce and budget.
The unit developed a small cohort of experienced nurses with enhanced skills. Unfortunately, due to insufficient numbers and the influence of the nursing rota, which dictated the number of QIS staff per shift, it was not possible to have a CCN on every shift. Additionally, due to their intensive care workload they were unable to utilise their enhanced skills across the unit and thus were unable to perform and maintain their skills as anticipated. Consequently, the role did not have the desired impact on wider service delivery and service provision remained inconsistent.
In hindsight the additional clinical skills had been bolted onto an established neonatal nurse job description. Although there was some financial remuneration for this, the CCNs were restricted in their ability to perform and maintain their skills due to their allocated patient workload and the lack of a defined role within the workforce. This highlighted the need for an entirely new tier of nurses within the nursing structure with a clearly defined role. There needed to be a significant enough number to be available on every shift and for them to be additional to the current nurse workforce and QIS numbers. These nurses needed the enhanced clinical knowledge and skills to be able to work effectively and flexibly across the neonatal service. This created the opportunity to provide an appealing career pathway for QIS nurses to develop enhanced skills in the role of an ENNP.
Financial support was secured from within the local trust to develop a new tier of ENNPs. With the support of the lead ANNP and service line director (also an ANNP) the opportunity arose to create an ENNP role to address identified workforce needs. In a truly serendipitous moment, this coincided with the development of an ANNP MSc pathway in partnership with Plymouth University. This was a significant opportunity to develop ENNP training in synergy with an ANNP pathway (FIGURE 1). This ensured ENNP training as an incremental component of the ANNP MSc pathway to facilitate an efficient and seamless route for those ENNPs wishing to pursue an ANNP career.
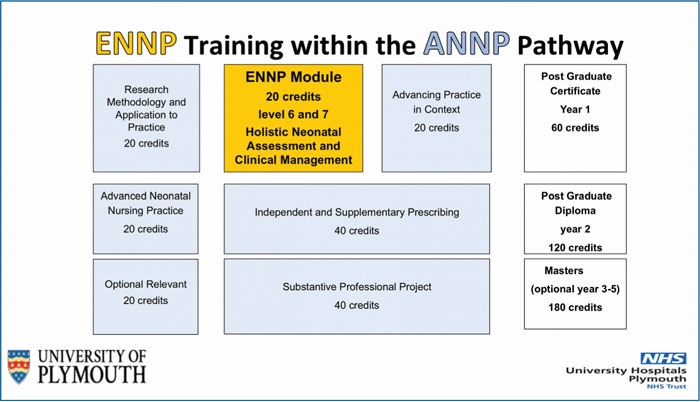
FIGURE 1 At the University of Plymouth the ENNP module sits within the ANNP MSc pathway.
This validated training provides a breadth of underpinning knowledge and ensures competency in a broader range of clinical skills, in comparison to the CCN. The clearly defined role offers a development opportunity for experienced QIS nurses who wish to pursue a clinically focused career, with the training offered at academic level 6 and 7 to increase accessibility. In addition, this stepping stone approach has increased the appeal to those who may not have previously considered an ANNP career, improving recruitment and retention potential. Currently, there are only three institutions in the UK that offer ENNP courses (TABLE 1).
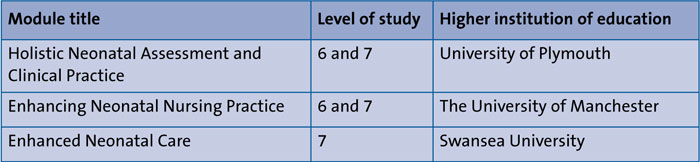
TABLE 1 Currently there are just three institutions that run ENNP courses in the UK.
This was a new role for the unit with a new job description and a clearly defined scope of practice, including extended skills and newborn and infant physical examination (NIPE) screening. In addition, ENNPs have an increased responsibility equivalent to that of the tier 1 in high dependency, special care and transitional care, where they review community admissions. They also attend low-risk deliveries to initiate resuscitation if required. Included in the ENNP job description is the provision of nursing and/or transport shifts to facilitate staff to maintain their skills, minimising the initial impact on the nursing rota until the skill void is back filled. This provides a clear career development opportunity for experienced QIS nurses.
In September 2017 six ENNP trainees were appointed and successfully completed training in June 2018. Subsequently six ENNPs are in post working alongside the nursing staff, ANNP and medical teams supporting clinical service delivery. The ultimate objective is to have an ENNP on every shift.
In a local audit of all clinical and non-clinical staff the impact of the role on service delivery was positively evaluated, relative to the delivery of safe and timely neonatal care. The success of this role has subsequently inspired other staff and created interest in the ENNP role within the unit.
Several ENNPs are now in the process of accessing ANNP training via the flexible modular pathway, which impacts positively on the future ANNP workforce. While it had previously been challenging to recruit ANNPs there is now an evolving future ANNP team. In a stepping stone approach, the ENNP role has provided the additional benefit of increasing the confidence of nurses who had been apprehensive of the academic component of ANNP training, allowing them to pursue their goals. As a consequence the unit is now working towards the recruitment and training of more ENNPs to maintain consistent care delivery.
The development of the ENNP role within our neonatal team has taken several years. However, there is a firm belief that this pursuit is in the right direction to deliver the right staff, with the right skills, in the right place, at the right time.3
Or read this article in our
Tablet/iPad edition
- The ENNP role provides an alternative career pathway beyond qualification in specialty.
- The success of the ENNP role is dependent upon a clearly defined scope of practice within a specific job description.
- When ENNP training is in synergy with an ANNP MSc programme it facilitates a seamless incremental transition into the ANNP role, improving recruitment and retention.
Also published in Infant:
