

Improving educational outcomes for children born preterm: a new approach
Children born preterm are at higher risk of special educational needs than their term-born peers, and have poorer attainment at school. As intervention efforts to date have had little success in improving long-term outcomes, a new approach to intervention is needed. The Premature Infants’ Skills in Mathematics (PRISM) team has developed a novel e-learning resource to improve educational support for children born preterm. The resource is freely available for use by parents, healthcare and education professionals worldwide and has been shown to improve teachers’ knowledge of preterm birth and their confidence in supporting children in the classroom. Here we describe the development and evaluation of the e-learning resource.
Deborah Bamber1Camilla Gilmore2
Samantha Johnson1
sjj19@leicester.ac.uk
On behalf of the PRISM Study Team (TABLE 1)
1Department of Health Sciences,University of Leicester, 2Mathematics Education Centre, Loughborough University

TABLE 1 The PRISM Study Team.
The need for an increasing focus on educational outcomes
Clinical outcome studies have, for many years, shown that children born very preterm (before 32 weeks of gestation) are at increased risk for neurodevelopmental disorders including cerebral palsy and vision and hearing impairments. However, cognitive problems such as deficits in IQ, attention, processing speed, working memory, visuospatial skills and executive functions, as well as social and emotional problems are the most common adverse outcomes.1 While most research has focused on children born very preterm, recent studies have shown that even those born a few weeks early, at 32-36 weeks of gestation, are at small but significantly increased risk for these problems compared with children born at term.
These kinds of difficulties can have a major impact on a child’s learning and wellbeing at school, and it is therefore unsurprising that children born preterm have poorer academic attainment than their term-born peers. By age five, at the end of the school reception year, preterm children already have poorer attainment across all six areas of learning in the Early Years Foundation Stage compared with children born at full term.2 Research in primary school also shows that, of all the subjects studied at school, preterm children have particular difficulties with mathematics. Children born preterm are also at increased risk for special educat-ional needs (SEN) and there is a clear association between increasing risk for SEN and decreasing gestational age at birth.3
As yet there is no robust evidence that children born preterm will catch up with their peers and preterm born adolescents continue to have poorer attainment than their term-born counterparts at the end of secondary schooling.4 In the longer-term, preterm born adults are also less likely to go on to higher education and are more likely to be unemployed, in receipt of social benefits and have lower wealth than adults who were born at term.5
Poor educational outcomes have significant economic consequences. After discharge from hospital, the greatest costs associated with extremely preterm birth lie not in health care, but in education.6 Moreover, the impact of preterm birth on education systems worldwide is likely to increase, as increasing preterm birth rates and survival rates will result in greater numbers of preterm children entering schools in the coming years. Recent reports also suggest that educational outcomes for children born extremely preterm may even be deteriorating despite ongoing advances in neonatal care.7 Thus it is imperative to focus our efforts on improving educational outcomes for children born preterm to maximise their life chances and to reduce the individual, societal and economic consequences of preterm birth.
Does early intervention improve long-term outcomes?
To date, efforts to improve neuro-developmental outcomes have focused predominantly on studying the efficacy of early preventive interventions delivered during the neonatal period and/or the first few years of life for improving cognitive and motor outcomes. However, despite reports of improved short-term outcomes, meta-analyses have shown that the long-term benefits of such programmes are limited and the short-term beneficial effects of intervention are no longer evident at school age.
Cognitive abilities, particularly executive functions, continue to develop significantly over childhood. It is thus likely that inter-vention in the first few years of life may not be sufficient to solve the complex issue of the impact of cognitive deficits on children’s learning throughout schooling.
If we want to improve attainment at school then intervention at school age may hold the key. To this end, attention has focused on the use of cognitive training or adaptive working memory training for improving children’s cognitive and academic outcomes. However, as yet, there is no robust evidence that such training programmes improve children’s academic attainment and working memory training is not currently recommended for children born preterm.9 Therefore alternative approaches to intervention for improving children’s educational outcomes are needed.
Education professionals’ knowledge of preterm birth
Two to three children in an average sized primary school class are likely to have been born preterm, yet education professionals currently receive little to no training about preterm birth and have very limited knowledge of the consequences of preterm birth on children’s learning and development.
In a survey of 585 teachers in the UK, we found that only 16% had received any formal training about preterm birth, and only 3% as part of their initial teacher training. Over 85% reported that they would like more information in this area. We also found that their poorest areas of knowledge related to the high risk for mathematics difficulties, inattention and poor social skills following preterm birth, suggesting that preterm children may not be receiving support in the areas they need it most.10 As teachers have primary responsibility for supporting preterm children in the long-term, this represents a significant public health concern.
Development of the preterm birth e-learning resource
Given that early intervention has met with limited success in improving long-term outcomes and that teachers have poor knowledge of how to support preterm born children in the classroom, we decided to take a new approach to intervention. Our aim was to develop a novel, multimedia e-learning resource to improve education professionals’ knowledge of the impact of preterm birth on children’s development and learning and to provide strategies they can use to support preterm children’s learning in the classroom. Thanks to funding from Action Medical Research, we are delighted to report that we have completed this work.
The e-learning resource was developed using a participatory design methodology in which 26 stakeholders including teachers, teaching assistants, educational psychologists, parents of children born preterm, and young adults who were born preterm themselves, attended a workshop to co-design the content and format of the resource. Storyboards produced during the workshop were developed into written specifications that were then reviewed by experts in neonatology, developmental psychology and education, and were revised where necessary. These were then used to develop prototype versions of the resource, which were reviewed by two teachers who provided feedback from the viewpoint of end users.
The final resource is freely available for use online and can be accessed at www.pretermbirth.info. It consists of five sections (TABLE 2), each of which comprises a mixture of audio, video, animation, text, images, case studies and quizzes to engage users in active learning. The final section of the resource provides strategies that education professionals can use to support learning for children with the cognitive, mathematics and social-emotional difficulties most commonly associated with preterm birth. In total, the resource represents approximately one hour of learning but is designed with stand-alone sections that users can access in smaller chunks and as many times as needed.
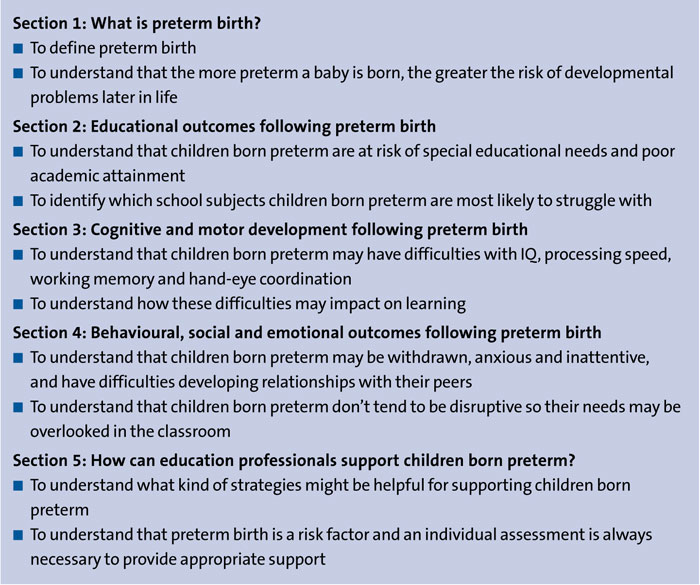
TABLE 2 Preterm birth e-learning resource: sections and learning objectives.
Evaluation of the e-learning resource
Before releasing the e-learning resource, we wanted to take the opportunity to assess whether it was effective in improving education professionals’ knowledge of preterm birth and in increasing their confidence in supporting preterm children in the classroom.
In October 2018, we carried out an evaluation study in which 61 teachers, teaching assistants, special educational needs and disabilities coordinators (SENDCO) and head teachers from eight primary, infant or junior schools in Nottinghamshire and Derbyshire participated. Participants were given up to 30 days access to the e-learning resource and completed questionnaires before and after using it. To assess whether there was any improvement in their knowledge, participants completed the Preterm Birth Knowledge Scale (PB-KS),10 a validated questionnaire that measures an individual’s knowledge of the long-term consequences of preterm birth. PB-KS scores range from zero to 33 and higher scores indicate greater knowledge. The detailed findings of the evaluation study have been published and so are summarised briefly here.11
We found that the median PB-KS score increased by 15 points, from 13 (95% CI 11 to 14; range 0-25) before using the resource to 29 (95% CI 28 to 30; range 18-33) after using it (p<0.0001; figure 1). This shows that the e-learning resource significantly improved teachers’ knowledge of the impact of preterm birth on children’s development and learning. Importantly, the greatest improvement in knowledge related to being aware of the risk for mathematics difficulties, poor social skills, inattention and deficits in visuospatial skills following preterm birth, which are among the most common areas of difficulty for children born preterm.
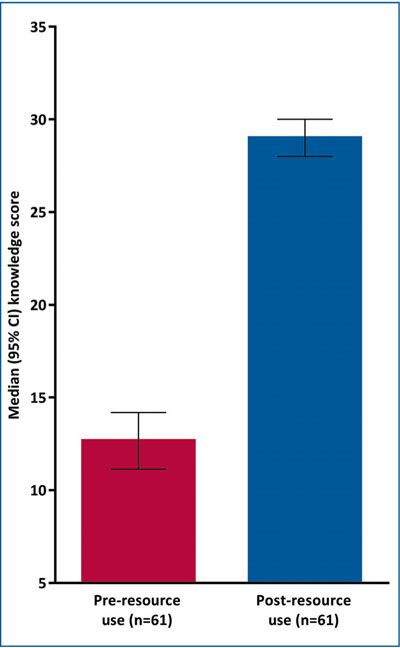
FIGURE 1 Median (95% confidence interval) Preterm Birth Knowledge Scale scores before and after using the e-learning resource.
To assess confidence in supporting the learning of children born preterm, participants also indicated the extent to which they agreed with the following four statements both before and after using the resource:
- I feel adequately equipped to support the learning of children born preterm.
- I feel confident in supporting the learning of children born preterm.
- I have received sufficient training about the effects of preterm birth.
- When I encounter a child who struggles at school, I consider whether or not they were born preterm.
We found that after using the e-learning resource, participant’s confidence in supporting children born preterm improved significantly. After using the resource there was a significant increase in the proportion of participants who felt adequately equipped (13% to 89%; p<0.0001) and confident (23% to 93%; p<0.0001) in supporting preterm children, and significantly more participants felt they had received sufficient training about preterm birth (0% to 69%) and would consider prematurity when encountering a child who struggles at school (23% to 82%; p<0.0001).
When asked if they would use information from the e-learning resource in their work, 82% said they would and 97% said they would recommend the resource to others.
Assessing the impact of the resource
In May 2019, we recontacted the 61 education professionals who participated in the evaluation study to find out if their increased confidence in supporting the learning of children born preterm was maintained six months after using the resource. To do this, we asked them to indicate, once again, the extent to which they agreed with the four statements about their confidence in supporting preterm children.
Overall, 38 (63%) participants responded, among whom confidence remained significantly higher than before they had used the resource (FIGURE 2): 84% (95% CI 73 to 96) still felt adequately equipped and confident to support the learning of children born preterm, and 63% (95% CI 48 to 78) still felt that they had received sufficient training about the effects of preterm birth since using the resource six months earlier. In total, 92% (95% CI 84 to 100) reported that they now considered prematurity when encountering a child who was struggling at school.
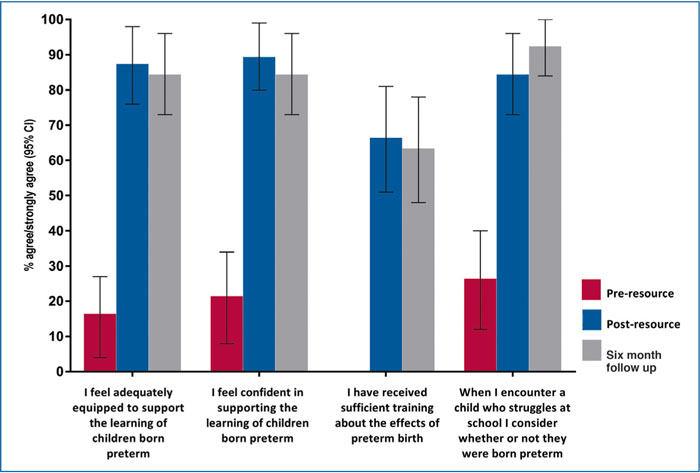
FIGURE 2 Proportion of teachers who agreed with statements about confidence in supporting the learning of children born preterm, before and after using the e-learning resource and at follow up six months later (n=38 at each assessment point).
Participants were also asked whether use of the e-learning resource had changed their thinking and the way they worked, or planned to work. Overall, 34 (90% of the respondents) reported that they now thought differently and 23 (61%) had changed the way they work, or planned to work since using the resource six months earlier. TABLE 3 gives examples of how use of the resource had changed participants’ thinking and teaching practice.
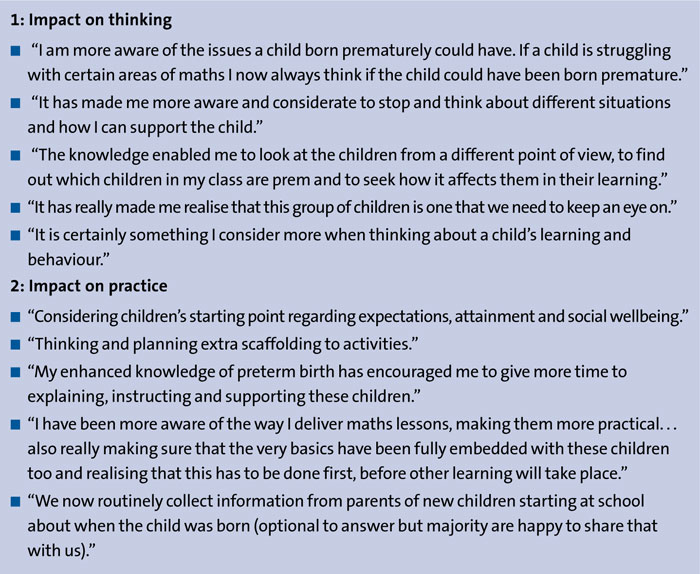
TABLE 3 Examples of ways in which the e-learning resource had changed participants’ thinking or teaching practice six months after use.

The e-learning resource gave increased awareness of prematurity among education professionals and consequent changes to teaching practice.
The results are very encouraging and show not only sustained knowledge and confidence, but also a significant impact on teachers’ practice six months after using the resource. As only two thirds of the initial evaluation study participants responded to the follow-up, this may have resulted in a biased sample; for example, teachers with a greater personal or professional interest in the subject area may have been more likely to respond, leading to an overestimation of the impact of the resource. However, this is unlikely to be the case as there was no significant difference in the median knowledge scale score between those who completed the six month follow up (median 13; 95% CI 11 to 14) and those who did not (median 12; 95% CI 9 to 18). Similarly, there was no significant difference in the proportion of participants who felt adequately equipped or confident to support preterm born children between those who completed the six month follow up and those who did not.
Thus we have demonstrated that evena short period of access to the resource produced real impact in terms of increased awareness of prematurity among education professionals with consequent changes to teaching practice.
Launch of the resource
Thanks to the funding from Action Medical Research, we were able to make the resource available non-commercially to minimise any potential barriers to its use. Since its release in May 2019, more than 3,600 people have accessed the resource in 41 countries worldwide. Although the resource was developed primarily for use by education professionals, we believe it may also be of benefit to healthcare professionals as a source of evidence-based information for their own professional development and as a valuable addition to neonatal follow-up or ongoing community care, providing parents of preterm born children with information about potential long-term difficulties and easing the child’s transition to school. The resource may benefit parents, in particular, who often report that they find it hard to raise the issue and importance of their child’s premature birth with teachers and to secure the support they feel their child needs in school. Indeed, there has been wide variation in the ‘roles’ of those recorded as accessing the resource to date, from parents, grandparents and family members of children born preterm to academics/researchers, teachers, educaional psychologists, other educational practitioners and healthcare professionals. We hope that raising education professionals’ awareness of preterm birth and their competence in supporting children in the classroom will help to bridge the gap between health and education services and improve educational support for children born preterm. Ultimately we hope that use of the resource will contribute to improving educational outcomes for this vulnerable group of children.
Acknowledgement
The authors would like to thank Dr Stephen Wardle of Nottingham University Hospitals NHS Trust and Dr Jonathan Cusack of University Hospitals of Leicester NHS Trust for their assistance with the PRISM Studies and in reviewing the content of the preterm birth e-learning resource.
Preterm Birth Information for Education Professionals is freely available at www.pretermbirth.info
Or read this article in our
Tablet/iPad edition
- Teachers have poor knowledge of the long-term consequences of preterm birth and how to support preterm born children in the classroom.
- We developed an e-learning resource for education professionals about how to support these children at school.
- Use of the e-learning resource improves teachers’ knowledge of the long-term consequences of preterm birth and their confidence in supporting these children in the classroom.
- Use of the resource may improve educational support and academic outcomes for children born preterm.
Also published in Infant:
