

Dysphonia following preterm birth
Dysphonia – vocal abnormality – in children that were born preterm is relatively common but it is not screened for and behavioural or surgical interventions may be difficult for parents to access. Childhood dysphonia often persists into adulthood and can result in significant adverse social, academic and emotional outcomes that may add to other pre-existing problems of prematurity (eg hearing, developmental and cognitive challenges). Infants born extremely preterm/low birth weight or those that have had patent ductus arteriosus ligation might benefit from early referral for expert assessment. This article includes a personal story to better appreciate the ‘lived experience’.
Lauren Dhugga1
Specialty Trainee in Paediatrics
Sophie Proud2
Neonatal Junior Sister
Salema King1
Specialty Trainee in Paediatrics
Claire McLarnon3
Consultant Otolaryngologist
Nicholas Embleton1,4
Consultant Neonatologist and Professor of Neonatal Medicine
nicholas.embleton@ncl.ac.uk
2Neonatal Unit, Belfast Health and Social Care Trust, Belfast
3Great North Children’s Hospital, RVI and ENT Dept, Freeman Hospital, Newcastle Hospitals NHSFT
4Population Health Sciences Institute, Newcastle University, Newcastle upon Tyne Dhugga L., Proud S., King S., McLarnon C., Embleton N. Dysphonia following preterm birth. Infant 2023;19(5):164-68.
The dramatic improvement in survival rates for very premature infants over the last 20-30 years has led to an increased focus on longer term neurodevelopmental sequelae and health-related quality of life (HRQoL). Early-life brain injury, especially haemorrhagic infarction and white matter damage, may result in life-long impairments affecting cognitive and socio-behavioural outcomes. While motor or physical impairments are frequently detected in the first 2-3 years of life, cognitive, language and socio-behavioural outcomes may not be apparent until school age or later in childhood.
Hearing impairment is relatively common in children born prematurely and can affect speech and language development; however, most cases are diagnosed in early infancy through routine screening and enhanced assessments for those with additional risk factors. Hearing aids can be highly effective and prevent the impairment from resulting in a disability.
In contrast, vocal disorders in premature-born children may be relatively common, but are not screened for and behavioural or surgical interventions may be difficult to access. The prevalence of vocal disorders in extremely preterm-born children is not known, but some studies suggest it might be >50% and there are data to show significant adverse impacts on HRQoL over the life-course.1
Dysphonia and speech production
Generation of vocal sounds is termed ‘phonation’ while the action of producing words is called ‘speech’. Phonation not only involves the vocal cords but also the oral and nasal cavities, pharynx, larynx, large airways (trachea and bronchi), lungs, thorax and diaphragm.2 Phonation/speech involves coordinated action to integrate complex movements and it is, perhaps, not surprising that speech problems are common in extremely preterm born children and adults over the life-course. Cortical nerve signals result in expiratory flow of gas from the lungs upwards through vocal cords that are adducted due to innervation via the recurrent laryngeal nerves (RLN) and which then vibrate to produce sound. Pathology in any of these component parts may result in a vocal disorder.2
The anatomy of the larynx is different in neonates compared to adults, which may increase the risk of injury when receiving care on a neonatal intensive care unit (NICU). Vocal disorders following preterm birth are often, either not recognised in infancy or early childhood, or not brought to medical attention, despite their co-existence with speech and language problems. In typical neonatal follow-up clinics, preterm-born children with a ‘normal’ Bayley score at two years of age are discharged from further paediatric follow-up, although the National Institute for Health and Care Excellence (NICE) has more recently recommended follow-up until four years of age.3
Typically, developing children at two years will have a vocabulary of up to 200 words or more; many will put 2-3 words together. However, routine neonatal follow-up may fail to recognise that the speech is indistinct or abnormal or parents may not report it. Dysphonia is therefore easily missed and even when parents recognise voice abnormalities, they might be unsure how to seek help or if intervention is necessary or even likely to be successful.
Average age at presentation to a voice clinic was just over five years in one case series,4 but there are likely to be many more children who never receive adequate multidisciplinary assessment. Follow-up studies show that while there is individual variation, childhood dysphonia often persists into adulthood.5-9
In comparison to language, speech and vocal problems are less studied in preterm children and many of the studies yield inconsistent results. When preterm children are compared to those born at term with speech problems, some studies show that the differences are largely accounted for by differences in rates of chronic lung disease and neurological problems.10 Preterm children also demonstrate higher rates of dysarthria (difficulty speaking because of weak speech muscles), which may be associated with other motor disorders such as cerebral palsy. Voice disorders are also more prevalent in preterm-born children and are strongly associated with common neonatal morbidities such as intubation and thoracic surgery. There is, therefore, a complex interplay of aetiological factors and pathological outcomes including feeding, speech, language, cognition, hearing loss and voice production. These are further complicated by social inequalities that may increase the chance of a delayed diagnosis or limit access to therapeutic interventions.11
Risk factors for dysphonia in preterm born children
Risk factors for dysphonia include extreme prematurity (birth at <28 weeks’ gestation) and extreme low birth weight (<1,000g), as well as being more likely in infants who required thoracic surgery, most commonly patent ductus arteriosus (PDA) closure (TABLE 1). Dysphonia is also more common in infants who experienced emergency or complicated intubations when direct trauma may have occurred. Prolonged intubation duration and tube size was not consistently associated with increased odds of later dysphonia in some studies,9 but in others prolonged intubation (>28 days) or NICU stays of >12 weeks were associated with higher rates of dysphonia.1,4 Interestingly, unlike many other neonatal morbidities, dysphonia in preterm-born children appears to be more common in females (odds ratio = 3.4).5-7,9
TABLE 1 Risk factors for dysphonia in preterm-born children.
Vocal pathology
Dysphonia can be classified according to which phonation mechanisms are affected and include:
- impairment of glottal closure
- stiffness, atrophy, nodules or scarring of the vocal cords
- vocal cord asymmetry.
These conditions alter the shape and/or movement of the cords. Occasionally, dysphonia may be due to problems with breathing, the ‘resonance chamber’ (larynx, pharynx and oral and nasal cavities) or psychological factors.2 Assessment requires specialist expertise and involves a range of techniques, such as:
Parent and child-reported voice-related quality of life scales are also useful.
Trauma due to emergency intubation may damage the fragile vocal cords and other glottic structures and result in long-term structural changes that may not be amenable to later surgery. The histopathologic laryngeal changes associated with intubation show ulcer formation proportional to the duration of intubation,12 which is especially marked in the sub-glottic and posterior glottic regions. Where intubation lasts for more than a week, these changes appear very commonly and expose the perichondrium of the cartilage, although there is also evidence that healing changes occur while the infants are still intubated.
In a case series of 20 children born at 23-29 weeks’ gestation with vocal problems, most (14 out of 20) had a posterior glottic chink with a mild degree of supraglottic hyperfunction (‘squeeze’). Several children had evidence of arytenoid prolapse or vocal cord immobility. Rarer findings included posterior scar band, vocal cord atrophy, arytenoid oedema and nodules. One child with structural laryngeal pathology had never been intubated.7,8
Nodules are bilateral lesions occurring on the anterior third of the vocal cords and maybe the commonest cause of dysphonia in normal adolescence, perhaps because of over-use or misuse of the laryngeal musculature.13 However, there are no good data to show they are more common in preterm-born adolescents. They appear more common in boys than girls in some but not all studies13,14 and are usually amenable to vocal therapy.
The RLNs are branches of the vagus nerve that run alongside the trachea and supply all intrinsic muscles of the larynx, with the exception of the cricothyroid muscles. The RLNs innervate the posterior cricoarytenoid muscles, which are the only muscles that can open the vocal cords. The left RLN loops under the aortic arch and is at risk of damage during PDA ligation. The right RLN loops under the right subclavian artery and may also be damaged during thoracic surgery. The RLNs also supply sensation below the vocal cords. In one case series of primary unilateral vocal cord paralysis in preterm children, 90% of cases involved the left RLN, in whom 92% of cases had cardiac surgery.15 Interestingly, studies also show that left RLN palsy may not present until adult life.16
Interventions: voice therapy and the role of surgery
Behavioural voice therapy can be highly effective in cases where there is no structural damage, but the effectiveness in the presence of vocal cord paralysis or traumatic injury is not well studied even in term-born children. Therapy may take several sessions and this may be challenging in children with other behavioural, developmental or cognitive impairment. Voice therapy is also useful pre- and post-surgical intervention but can be time consuming. One study showed that telehealth (virtual) therapy was feasible and effective.17
Surgical interventions for vocal cord palsy include:18,19
- injection laryngoplasty
- surgical medialisation – ‘pushing’ the paralysed vocal cord closer to the functioning cord
- laryngeal reinnervation – surgery to promote neuronal reinnervation.
Injection laryngoplasty is minimally invasive and may use hyaluronic acid, calcium hydroxyapatite, gel or other implants to obtain glottal closure. FIGURE 1 shows the glottis before and after hyaluronic acid injection augmentation of the vocal cord. Post-operative assessment of vocal cord function, voice quality and patient-reported outcomes is complex and multi-dimensional, but many studies show it is effective in some but not all patients.20 Assessment includes perceptual, acoustic and aerodynamic assessment, as well as direct endoscopic visualisation.21 In writing this review, we did not find any large case series of injection laryngoplasty in children or adults who were born preterm.
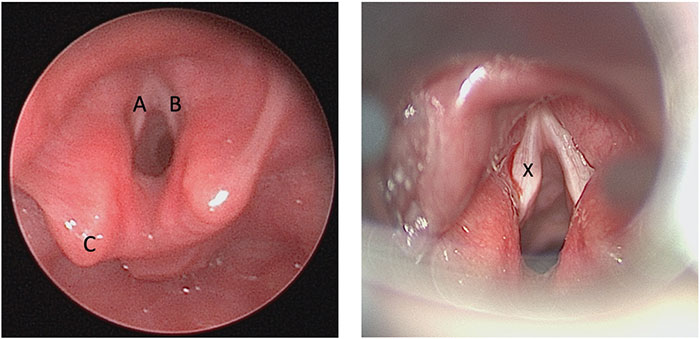
FIGURE 1 Endoscopic images of the larynx of an ex-preterm born at 26 weeks’ gestation with left vocal cord paralysis after PDA ligation. Left: Pre-operative image showing A = left vocal cord, B = right vocal cord and C = left arytenoid. Notice the prolapsed left arytenoid due to palsy. Right: Left vocal cord augmentation with hyaluronic acid, X = site of hyaluronic acid.
Impacts of dysphonia or laryngeal abnormalities over the life-course
The larynx is the narrowest part of the airway and is therefore responsible for a large proportion of total airway resistance.22 It is possible, therefore, that laryngeal disorders might be associated with exercise-related respiratory symptoms in preterm-born children. In a large Norwegian cohort of 228 preterm-born adolescents, those who had PDA surgery had an odds ratio of 3.4 for having breathing problems during exercise, and an odds ratio of 16.9 for having a hoarse voice.22 Surgery for PDA and prolonged mechanical ventilation were closely associated, meaning the independent effect of surgery was difficult to determine. Many children had previously been prescribed, but discontinued, asthma medication. This suggests that breathing problems during exercise may have previously been misdiagnosed as asthma.
HRQoL is a broad multi-dimensional concept that includes the patients’ subjective evaluation of both positive and negative aspects of life, which includes physical, mental, emotional and social domains. Voice-related QoL was assessed using qualitative analysis to identify themes in children of different ages with dysphonia. Young children expressed issues related to physical function including ‘run out of air’ or ‘sometimes voice doesn’t work’.23 90% of the children reported that they had been repeatedly asked to use a quieter voice in school, which probably had a negative impact on their education. Older children and adolescents said their dysphonic voice received undue attention and limited their participation in important events – they felt they ‘missed out’. Adolescents were sometimes afraid or hesitant to speak; they worried about ‘sounding dumb’, reported being teased by other children and many were asked to ‘speak up’. Many said they felt they were left out of activities or felt isolated.23 They also expressed anger, sadness and frustration. Dysphonia may also impact on educational performance and occupational choices,4,24 and many parents perceived poor long-term voice quality as an important ongoing issue (FIGURE 2).1
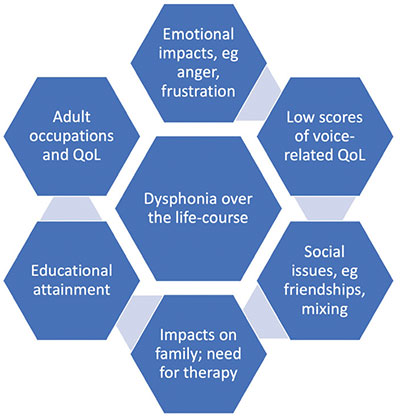
FIGURE 2 Impacts of dysphonia over the life-course.
Conclusions
Voice abnormalities in extremely preterm or low birthweight infants may be quite common in later childhood and clinical teams should have a low threshold for clinical evaluation in those with risk factors.4,5,7,9 There is no agreement on those preterm infants that should be referred for assessment but infants born at <1,000g, <28 weeks’ gestation or those who have had PDA ligation might benefit from expert assessment. Dysphonia results in significant adverse outcomes including worse HRQoL and concerns parents throughout childhood.1 The adverse social, academic and emotional outcomes may add to pre-existing problems of prematurity including hearing, developmental and cognitive challenges.4 While prevention is clearly better than cure, the increased survival of infants born at <24 weeks’ gestation means this key neonatal morbidity will remain important. It is currently uncertain if early therapy intervention will improve outcomes, but it is also likely that in the future surgical techniques may improve.
Lived experience of dysphonia
By co-author Sophie Proud
I was one of twins born at 23+6 weeks’ gestation in 1996. Sadly, my twin sister, Beth, died on the day we were born. I was ventilated for more than two months, was re-intubated several times and sometimes needed CPR. I had a large PDA ligated at three weeks of age (left thoracotomy) following which I needed high frequency oscillatory ventilation for more than a week (nitric oxide wasn’t readily available back then). I also had cryotherapy for bilateral retinopathy of prematurity, required re-ventilation for pneumonia on day 99 and was finally discharged home shortly after term on 1.5L of oxygen. Apparently, no one ever heard me cry on the NICU but since then, my chief complaints have been hoarseness, abnormal voice pitch, abnormal voice strength and a wavering voice.
I always knew I had a ‘different’ voice and as a child I was constantly asked if I had a sore throat. My voice quality was affected by many factors, the most significant being the weather; in winter/cold weather my voice would be poor, whereas abroad/in humidity it would improve. Fatigue also had a detrimental effect on my voice quality. I hated being different and this definitely affected my confidence, particularly as a teenager. In fact, it wasn’t until I had a neonatal placement during my nurse training that I began to accept it as a small price to pay for what I went through.

Sophie Proud as a preterm baby and now a neonatal junior sister.
As a child, I was referred to speech and language therapy; I attended once and it was deemed that physio/voice exercises actually made my voice worse, ie hoarser. As an adult, I accepted that nothing could be done and presumed that intervention would have been needed at a younger age. I think assuming that nothing can be done is a limiting factor and when I discussed this with a neonatal consultant colleague, we both felt that parents might think it’s a small price to pay and that other issues (eg lung function or developmental progress) would be greater priorities. Perhaps like me, many people assume that nothing can be done to improve voice quality.
The first assessment of my voice that I know of, involved laryngeal endoscopy. This showed right-sided weakness and the glottis didn’t fully close (ie a glottal closure disorder) but no paralysis and perhaps a better assessment than was expected given my history. Following this diagnosis, I had my first injection of hyaluronic acid in November 2020 as a short-term, temporary measure to assess possible effectiveness before injection with calcium hydroxyapatite in June 2021 (FIGURE 3). The calcium injections in theory may have had a longer-term effect (up to two years) and following both sets of injections, I underwent regular, targeted voice therapy. With the calcium injections I found that the recovery was quicker, less painful and with less need for throat clearance and coughing. However, there was very little effect. The gap has closed and the muscles surrounding the vocal cords are much less strained but this does not translate to the sound of my voice – unfortunately it is the same as it was before treatment.
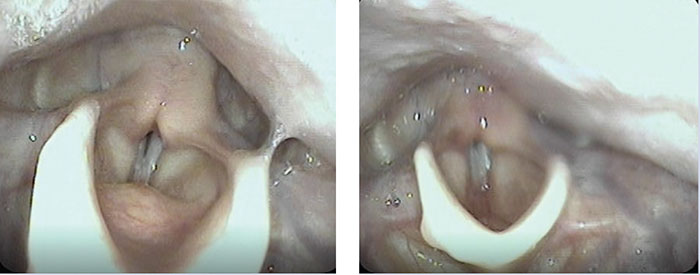
FIGURE 3 Sophie’s glottal closure disorder before (left) and after (right) hyaluronic acid treatment. The gap has closed but the quality of her voice did not improve.
I now work as a neonatal junior sister on a large NICU and I am able to share my experience with others, including parents. I feel lucky that I have done so well after being born so premature, but it is important to acknowledge that my voice quality has had a huge impact on many aspects of my life. I’m looking forward to being part of research to help understand the condition better and work towards improving interventions for future children and families.
Or read this article in our
Tablet/iPad edition
- Dysphonia is common in children who were born preterm. It may result from damage to the larynx, laryngeal nerves or other structures.
- It is often under-recognised or not referred for expert assessment.
- Dysphonia can have significant adverse impacts over the life-course.
Also published in Infant:
