

Prevention is indeed better than cure: the successful management of neonatal haemochromatosis
In this case report, we present a growth-restricted preterm infant with a family history of neonatal haemochromatosis who presented with deranged liver function at birth. Aggressive in utero treatment along with exchange transfusion and immunoglobulins in the first few days of life prevented worsening of liver failure and resulted in rapid improvement in liver function.
Audrienne Sammut1MD, MRCPCH
Paediatric Specialty Registrar
a.sammut@nhs.net Jogesh Kapadia1
MBBS, DCH, DNB(Paed), MRCPCH, DipClinRiskClaimsManag, MMedEd, FHEA
Neonatal Consultant Shyam Das2
MBBS, MD, FRCOG
Consultant Obstetrician and Gynaecologist Bharat Vakharia1
MBBS, MD(Paed), MRCPCH
Neonatal Consultant 1Neonatal Intensive Care Unit, 2Department of Obstetrics and Gynaecology, Luton and Dunstable Hospital NHS Trust, Luton
The case
A liveborn baby boy weighing 1,880g was born to non-consanguineous parents at 34+2 weeks’ gestation following emergency caesarean section for reduced fetal movements, intrauterine growth restriction (IUGR) and abnormal cardiotocograph (CTG). He has a nine-year-old brother who was diagnosed with neonatal haemochromatosis (NH) a few days after birth and required a life-saving liver transplant at one month of age.
The mother had a miscarriage a year previously; therefore, during this pregnancy she received intravenous immunoglobulin (IVIG) at 14 and 16 weeks’ gestation, and then weekly from 18 weeks of pregnancy until delivery. She had growth scans every two weeks from 20 weeks. The pregnancy progressed well until 30 weeks, after which the fetus was diagnosed to have growth restriction.
From 30 weeks, the pregnancy was managed with weekly fetal surveillance on scan. Progressive coarse echogenicity was identified in the fetal liver along with progressive splenomegaly (FIGURES 1 and 2).

FIGURE 1 Coarse echogenicity in the fetal liver at 32 weeks’ gestation indicating nodularity/calcification, possibly secondary to injured hepatocytes.
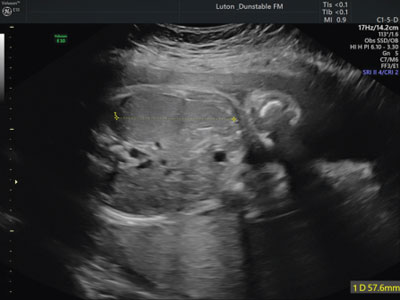
FIGURE 2 Antenatal splenomegaly at 32 weeks’ gestation.
At 34 weeks, the mother was admitted for steroid administration with a view to deliver the baby. Suspicious CTG precipitated an urgent caesarean section the next morning. The infant required admission to the neonatal intensive care unit (NICU) for continuous positive airway pressure in view of initial respiratory distress. The baby was visibly jaundiced and had hepatosplenomegaly on examination. An initial low blood glucose level (0.1mmol/L) at 40 minutes of age was treated with a dextrose bolus followed by intravenous maintenance fluids. Umbilical lines were sited, and phototherapy was commenced in view of a high serum total bilirubin. Admission blood tests (TABLE 1) suggested acute liver failure with markedly raised gamma-glutamyl transferase, aspartate aminotransferase (AST), alpha-fetoprotein (AFP) and ferritin as well as abnormal clotting. An abdominal ultrasound scan revealed mild hepato-megaly and splenomegaly. The liver had coarse heterogeneous echotexture, but no focal lesions. Both kidneys were normal and there was no evidence of ascites. Following discussion with the paediatric liver unit on day 1 of life, the infant was treated with a second dose of 1mg intramuscular vitamin K, a double-volume exchange transfusion, and an IVIG infusion of 1g/kg (10mL/kg)/dose as a single dose at a rate of 0.3mL/kg/hr for the first 30 mins, 0.6mL/kg/hr for the next 30 mins, then 1.2mL/kg/hr for the remainder of the infusion.
On day 2 of life, the infant was started on antioxidant therapy in the form of intravenous N-acetylcysteine 100mg/kg/day, selenium 3µg/kg/day and oral vitamin E 50mg daily, which were given until day 10. Vitamin K 1mg daily, ursodeoxycholic acid 10mg/kg three times a day and multivitamins 0.6mL daily were also added. He also had hypocalcaemia on day 2, for which he received four boluses of calcium gluconate, followed by oral calcium supplements in the form of calcium carbonate 0.25mmol/kg four times a day and cholecalciferol 1,500 units daily.
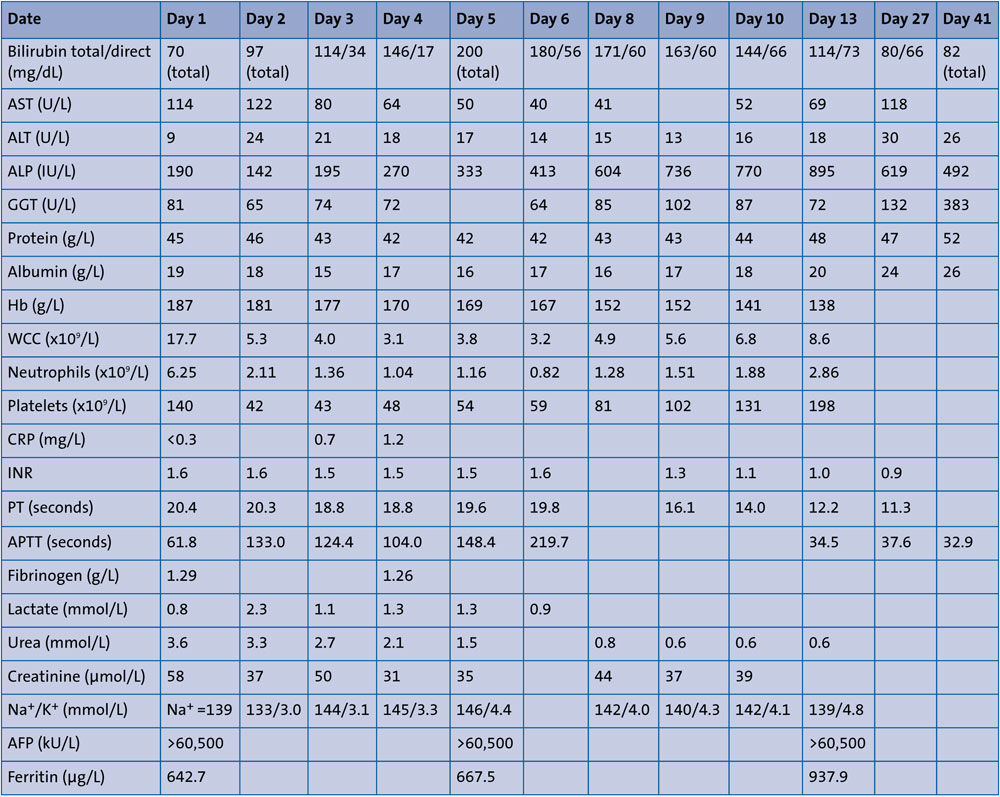
TABLE 1 Results of serum investigations performed during the infant’s hospital stay. Key: AST = aspartate aminotransferase, ALT = alanine aminotransferase, ALP = alkaline phosphatase, GGT = gamma-glutamyl transferase, Hb = haemoglobin, WCC = white cell count, CRP = C-reactive protein, INR = international normalised ratio, PT = prothrombin time, APTT = activated partial thromboplastin time, Na/K = sodium/potassium, AFP = alpha-fetoprotein.
He received cautious total parenteral nutrition (TPN) at a maximum volume of 95mL/kg/day of aqueous solution (3.1g/kg/day of amino acids) and 5mL/kg/day of SMOFlipid for two days while nasogastric feeds of expressed breast milk and/or term formula were gradually increased. He reached full feeds by day 6. Infection markers remained low and blood cultures were negative. Antiviral therapy was discontinued after serum polymerase chain reaction (PCR) tests for herpes simplex virus, Epstein-Barr virus and urine PCR for cytomegalovirus (CMV) were reported negative.
Liver function tests showed a marked improvement by day 3; however, he developed persistent conjugated jaundice. His stool and urine were normal in colour. Urine CMV PCR was negative on retesting. Both parents and the infant tested negative for galactosaemia and alpha-1 antitrypsin deficiency. He remained clinically stable and was discharged home on day 18. On follow-up with the paediatric liver unit at the age of three weeks, he had a liver MRI scan that showed a heterogenous nodular liver indicative of mild liver disease. The second follow-up at six weeks of age showed an improvement in conjugated jaundice and normal clotting function. The specialist team did not feel the need for a liver biopsy.
The child is thriving well at six months of age with a current weight of 7kg and reaching all of his developmental milestones. He continues to have hepatosplenomegaly but his jaundice is improving. He will continue to have regular follow-up with the paediatric liver unit.
Discussion
NH was first reported in 1957 by Hans Cottier who described a rare, fatal multi-organ disease characterised by iron deposition in sibling newborns with advanced liver disease, similar to that seen in hereditary haemochromatosis.1 Its aetiology and pathogenesis, however, was uncertain. Due to its occurrence in siblings, it was believed to be a genetic disease. It was not until 2010, that NH was found to be caused by a complement-mediated cascade of hepatocyte injury with maternal IgG antibody directed against fetal hepatocytes. It is thus a gestational alloimmune liver disease (GALD) that causes in utero liver injury leading to the NH phenotype.2
The injured fetal hepatocytes in GALD are unable to produce hepcidin, a regulatory feedback molecule produced in states of iron sufficiency to regulate placental iron transport. This results in excess iron crossing the placenta and depositing in the fetal liver. In addition, the transferrin production is decreased resulting in a surplus of circulating non-transferrin bound iron (NTBI). Various organs that cannot regulate this NTBI are more susceptible to siderosis than others, including the exocrine pancreas, myocardium, thyroid and salivary glands.2
NH is hereditary, not genetic. After having an affected infant, there is a 90% chance that each subsequent baby is affected. It is not surprising that after having had a child with confirmed NH nine years ago, our maternal index case had an affected fetus. The miscarriage she suffered a year ago may well have been due to fatal NH. Unfortunately, there was no post mortem performed. Following the discovery of GALD as the underlying disease mechanism, Whitington et al first recommended high dose IVIG in 2004 to reduce the severity of recurrent NH in expectant mothers.3 To date, various studies have reported success in reducing fetal mortality and morbidity with this approach. Feldman et al recorded a good outcome in 99% of their 140 pregnancies treated with IVIG. Only one infant demised at 22 weeks due to late initiation of treatment. The recommended dose is 1g/kg body weight (maximum 60g) of IVIG at 14 weeks, 16 weeks, and then weekly from the 18th week of pregnancy until the end of gestation.2 We used the same regime in our maternal index case.
GALD-NH can present as a spectrum of disease severity ranging from fulminant, life-threatening liver failure to no clinical signs of illness. Infants who have GALD-NH are likely to have IUGR, as did our patient. This is mainly as a result of ongoing liver disease in utero, the liver being a critical organ in fetal nutrition and metabolism. He also presented typically with liver failure within hours of birth showing hypoglycaemia, coagulopathy, hypoalbuminaemia and jaundice. There was no renal involvement. Laboratory results were characteristic of the disease with marked conjugated and unconjugated hyperbilirubinaemia, very high AFP levels (100,000-600,000ng/mL) and high serum ferritin levels (>800ng/mL). In view of the marginally raised AST of 114IU/L, he was started on antiviral therapy as this was thought not to be typical of GALD-NH, however, PCR testing excluded a viral infection and aciclovir was stopped. The serum lactate level was normal, which excludes some but not all, underlying metabolic disorders.2 The gold standard method of diagnosis for NH remains a liver biopsy, but this can only be performed in specialist centres and should not delay life-saving treatment.
Perinatal medicine has seen groundbreaking advances over the years. Many conditions previously known to be universally fatal during fetal or neonatal life, are now either preventable or have significantly less disease burden. The prognosis for severe NH without intervention remains poor. Ever since the discovery of GALD as a cause of the acute liver injury in NH, treatment strategies have been aimed at reducing the immune-mediated attack on the fetal hepatocytes rather than iron chelation therapy. This includes antenatal IVIG, a double-volume exchange transfusion immediately after birth to remove existing reactive antibodies, followed immediately with an IVIG infusion in order to block antibody induced complement activation.2 This novel form of aggressive medical treatment has been shown to improve survival rates to about 75% without the need for a liver transplant.4 This is a significant positive change compared to the historical success rate of 10-20% survival offered by iron chelation and antioxidant therapy alone.5 In our patient, antioxidant therapy was recommended as an adjunct to the mainstay of treatment to reduce oxidative injury caused by iron overload, if any.
While we aggressively targeted this immune-mediated liver injury both antenatally and postnatally, this baby’s prognosis remains guarded. Medical treatment can dampen the ongoing inflammatory cascade but cannot reverse the liver injury that may have already occurred. It can take up to 2-4 years for full recovery. In the event liver function deteriorates, liver transplant might still be warranted as definitive therapy.2 Although advancements have been made in the medical treatment of NH, there is still scope for further research.
Parental consent
The authors received permission from the patient’s mother to publish this case report.
Or read this article in our
Tablet/iPad edition
- Neonatal haemochromatosis can cause in utero liver injury resulting in life threatening liver failure at birth.
- Antenatal intravenous immunoglobulin reduces immune-mediated fetal hepatocyte injury and improves survival rates by 75%.
Also published in Infant:
