

Neonatal abstinence syndrome: a current update
There is an absence of consensus with regard to the monitoring and assessment of neonatal abstinence syndrome (NAS) symptoms and severity, and commencement of pharmacological treatment. As a result different treatment practices have evolved locally, nationally and internationally. The main goals of NAS therapy are to promote infant and maternal regulation and to minimise the signs of NAS expression in the infant by optimising the environment and using pharmacotherapy only when necessary. This article reviews current NAS understanding including antenatal approaches, community-based programmes, follow-up, knowledge gaps and potential future research ideas.
Rohit KumarMRCPCH
Consultant Neonatologist
Shalabh Garg
MD, FRCPCH, PGCertClinRes
Consultant Neonatologist
s.garg@nhs.net
James Cook University Hospital, Middlesbrough
Background
Substance misuse among pregnant women is a worldwide major public health concern. Data from the UK Advisory Council on the Misuse of Drugs suggests 6,000 babies are born to mothers who abuse drugs each year (1% of all UK deliveries).1,2 Both the incidence and the prevalence of maternal substance use, misuse, abuse and dependence is increas-ing and this is especially true among younger women. This is being reported uniformly across all communities and ethnicities, with implications for pregnancies, notably poor intrauterine growth, premature birth, stillbirth and birth defects.
Substance misuse is now common and complex, and imposes additional social, economic and healthcare costs to society. Above all, however, it poses a significant threat to the long-term health outcomes for the exposed infant.
Prolonged in utero drug exposure may result in NAS, an acute multi-systemic clinical entity that usually presents in the first few days of life. NAS is a variable and complex pattern of neonatal neurobehavioural signs in response to withdrawal symptoms, acute toxicity or lasting drug effects. These infants often endure long and costly hospital stays including prolonged separation from their mothers. The overall impact on NHS resources and local authorities is enormous and underestimated, and recently the evaluation and management of infants with NAS has received renewed attention.
Epidemiology of opioid use and NAS
A number of recently published articles highlight that the incidence of substance misuse in women and in pregnancy is gradually rising.2-8 In a recent national survey in the USA, 18.3% of pregnant teens, 9% of pregnant women aged 18-25 years, and 5.9% of all pregnant women reported some illicit drug use.3 One-third of drug users in treatment in the UK are females and 90% of these are of child-bearing age. The exact incidence is difficult to ascertain due to a number of factors leading to under-reporting, eg feelings of shame, denial, stigma experienced by the drug user, the presence of comorbid psychiatric disorders, lack of awareness among professionals in antenatal services and sociocultural barriers that may prevent a thorough assessment. Another area of significant concern is the rise in the incidence of prescription opioid misuse and resulting NAS.9
Clinical presentation
NAS is a variable, complex and incompletely understood constellation of symptoms and signs of neonatal neurobehavioural dysregulation.6,10-11 Clinical signs of neonatal drug withdrawal encompass dysfunction in four neuro-behavioural domains:
- autonomic regulation
- attention and state control capacities
- responses to sensory stimuli
- motor and tone control.
Multiple drug exposure can exacerbate the infant’s expression and/or severity of opioid-induced neurobehavioural dysregulation. Some of the common symptoms associated with NAS are listed in TABLE 1.12
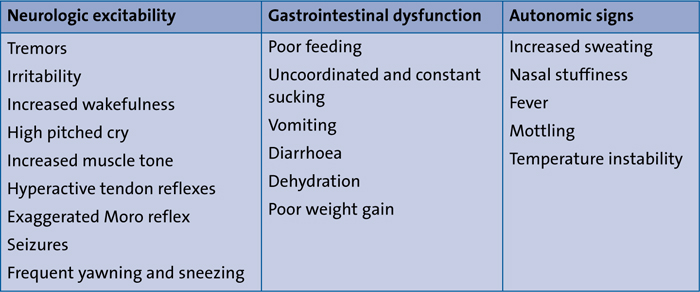
TABLE 1 Common clinical symptoms in infants with NAS.
The clinical presentation of infants with in utero drug exposure is variable and is dependent on the substance(s), timing and amount of the last maternal consumption, the presence of concomitant conditions, maternal and infant metabolism and excretion, and genetic and epigenetic factors. Genetic variations of the µ-opioid receptor (OPRM1) and the catechol-o-methyltransferase (COMT; encodes an enzyme that metabolises catecholamines) genes appear to affect the need for pharmacotherapy and length of stay in neonates with prenatal opioid exposure.13 The timing of withdrawal varies depending upon the recent history of exposure and the half-life of drug elimination.
Preterm infants have a lower incidence of NAS compared with term infants. The reasons for this difference may include:
- a shorter in utero exposure time
- decreased placental transmission
- inability to fully excrete drugs by immature kidneys and liver
- minimal fat stores leading to lower opioid deposition and activity
- a limited capacity to express classic NAS symptoms by the immature brain.1,14
Challenges with diagnosis and monitoring in NAS
The clinical diagnosis of prenatal opioid exposure is based upon history (or suspected history) of maternal opioid use, positive maternal or infant urine toxicology screening for opioids, and neonatal findings that are consistent with NAS. Specific infant tests used for the detection of substance exposure have their own limitations. Urine screening of the newborn has a low sensitivity (high false-negative rate) because, for most substances, only infants with recent exposure will have a positive test. Testing of neonatal hair is challenging due to difficulties in quantifying the small amount of drug, the slow growth of hair in the fetus/neonate and because this practice could be culturally unacceptable. Meconium analysis is sensitive and specific for drugs (including opioids) that are excreted either in the hepatobiliary system or amniotic fluid via fetal renal excretion. However, meconium must be collected before the specimen is contaminated by transitional human milk, or formula stools and, if meconium is passed in utero, this collection is not possible. In addition, analysis of meconium for substances reflects drug exposures during the second and third trimesters when meconium forms and therefore may not reflect periods of drug abstinence closer to delivery.15
There is an absence of consensus with regard to the monitoring and assessment of NAS symptoms and severity, as well as correlation to commence pharmacological treatment. The variability in NAS expression, its onset, severity and duration is currently not well described due to poorly understood pathophysiology. This is related to the difficulty in controlling possible confounding effects and, as a result, different treatment practices have evolved locally, nationally and internationally.
Scoring systems to monitor for NAS severity
Neonatal opioid withdrawal symptoms have traditionally been measured by observer-reported questionnaires that have an established cut-off score that guides decisions about the need for pharma-cological intervention. However, over the last 50 years a variety of NAS screening tools have been developed to guide prescribing decisions. The decision to score a neonate is based on observable symptoms and a positive maternal or a neonatal drug screen when no prior drug use history exists.
The Finnegan scoring tool remains one of the most comprehensive and widely used tools for monitoring the severity of opioid withdrawal symptoms.16 The Lipsitz Neonatal Drug Withdrawal Scale is much shorter and reported to be more user-friendly, although it has been criticised for providing only subjective ratings of gross individual symptoms and has not been widely validated.17 A short form scale, developed by Rivers, groups different symptoms and scores the presence of any symptom but does not take into consideration the frequency or the severity of the symptoms during the observed period.18
Inconsistencies in the use of these NAS scales include the timing, duration and frequency of administration and the degree to which observers are trained. NAS scales designed for term neonates are not validated to assess preterm neonates who may have a qualitatively different expression of abstinence symptoms.19,20
Comparisons of research findings are complicated by the use of screening tools that are different in composition and scoring. A further difficulty has been the potential for differential diagnosis with other medical conditions that may exaggerate NAS scores, eg sepsis, hypoglycaemia, hypocalcaemia and hyperthyroidism.
Management strategies for NAS
The main goals of NAS therapy are to promote infant and maternal regulation and to minimise the signs of NAS expression in the infant by optimising the environment and using pharmacotherapy only when necessary. Recent literature supports practices that keep opioid-dependent mothers and their infants together from birth. Such practices have additional benefits, such as lower neonatal unit admissions, higher breastfeeding initiation rates, less need for pharmaco-therapy and shorter hospital stays.21, 22
Some of these objectives are more effectively achieved if there is good community-based support for these families. In our neonatal unit we have adopted such a model, which is described later in this article.
Non-pharmacological management encompasses environmental control, feeding methods, soothing techniques, therapeutic modalities and social integration.23 Several interventions, including breastfeeding, swaddling, rooming-in and skin-to-skin contact, have proven to be effective in managing NAS and should be incorporated into the standard of care for this population. Non-pharmacological interventions have been shown to reduce the effects of withdrawal and should be implemented as soon as possible following birth. Examples of supportive interventions also include safe swaddling, gentle waking, quiet environment, minimal stimulation, lower lighting, developmental positioning and music or massage therapy.
Breastfeeding should be encouraged because it can delay the onset and decrease the severity of withdrawal symptoms as well as decrease the need for pharmacological treatment. Breastfeeding increases mother-infant bonding, enhances maternal confidence and encourages active maternal participation in the management of the infant.24,25
Pharmacotherapy for NAS
Initial treatment for neonatal withdrawal should be primarily supportive because medical interventions can prolong hospitalisation, disrupt mother-infant attachment and subject an infant to drugs that may not be necessary. In the literature, medical intervention necessary to control withdrawal symptoms has been variably quoted in 27% to 91% of neonates with NAS. However, because of the complex nature of withdrawal and the unknown effects of various licit and illicit drugs, there are currently no uniformly accepted pharmacological interventions or standardised regimens for the management of NAS.
Several pharmacological agents have been used to ameliorate symptoms associated with neonatal opioid withdrawal but only a few studies have examined pharmacological efficacy. The American Academy of Pediatrics recommends matching drug selection to the type of agent causing withdrawal but there are only a few randomised studies with pre-specified sample size calculations to support pharmacologic treatment regimens. In the last 20 years, only five such randomised clinical trials with pre-specified sample size calculations (four neonatal and one maternal treatment) have been published. Each of these trials was small and tested different therapies, limiting the extent to which the results can be aggregated/generalised.
Morphine and methadone remain the most common first-line medications, although the evidence is lacking for which agent is superior.26 The most recent systematic review of pharmacological agents for NAS suggests that buprenorphine is the optimal treatment but the limitations are considerable and wide-scale adoption requires a large multicentre trial. Oral morphine (the most commonly used pharmacological agent for NAS treatment) is the lowest ranked opioid for the duration of treatment and hospital stay.27,28 A description of individual pharmacological agents used in the management of NAS is presented in the article by Toone, Johnson and Harrison in this issue of Infant.29
Community support and weaning strategies
A systematic review of outpatient pharma-cological weaning for NAS identified 154 studies, of which only six met all the inclusion and exclusion criteria. These studies identified that outpatient weaning for select infants was associated with shorter hospitalisation compared with infants weaned in hospital and may potentially be effective in reducing associated healthcare costs. However, the duration of pharmacologic treatment was longer in the outpatient weaning groups in the majority of the studies. Furthermore, the adverse events were rare and compliance with the follow-up treatment was high among those who received outpatient weaning.30
Over the years we have seen a major shift in our management strategies for babies needing pharmacotherapy to control their NAS symptoms. A few years ago, it was the norm to admit the baby needing medical treatment for NAS to the neonatal unit; we are now at a stage where hardly any are admitted and the majority remain with their mothers on the postnatal ward until fit for discharge. The only reason to admit an NAS baby is for situations when the mother is not in a safe state (physical or mental) to look after her baby or social services have decided for the mother not to have access to her baby. This has become possible with the establishment of an effective transitional care facility, development of pragmatic NAS guidelines for the postnatal ward, regular training and education of midwifery staff as well as the active involvement of a community neonatal nursing team.
When a baby at risk of developing NAS is born, the neonatal team members meet with the family to explain what NAS is including symptoms, strategies to manage these symptoms and reasons for the increased length of stay, as well as practical advice to look after their baby after discharge. They are also provided with an information leaflet that further explains the overall management of NAS and has details of the community nursing team. The leaflet provides parents with information and answers to common questions (TABLE 2).
An effective and well-coordinated discharge plan involving an inter-professional healthcare team and outlining a comprehensive medications weaning schedule is essential to ensure a seamless transition from hospital to community, and for maintaining continuity of care. This is mostly led by the community neonatal nursing team.31,32
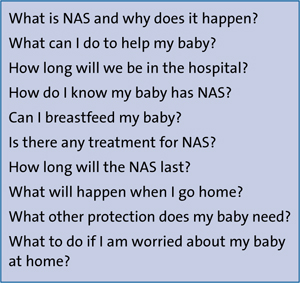
TABLE 2 Common questions asked by parents of babies at risk of NAS.
If a baby is to be discharged on oral morphine, the community team meets with the family before discharge, provides them with their contact details, visits them at home within 2-3 days after discharge and then twice weekly until fully weaned off the medicine. The team follows up with a phone call between visits to ensure the parents are well supported and reassured. They also monitor growth, give feeding advice and provide weaning strategies for the morphine in liaison with the named consultant neonatologist.
Follow-up and long-term outcomes
Currently, there is a lack of good quality longer-term outcome studies to accurately assess the effects of chronic in utero exposure to various substances of misuse, especially the opioids. Certainly, prenatal (multi/poly-drug exposure, prematurity, low birth weight, intrauterine growth restriction, antenatal care) and postnatal (continued maternal drug use, exposure to violence, and socioeconomic and educational level) confounding factors make it difficult to assess the specific impact of NAS on the long-term health outcomes. In a systematic review of case control studies, there were no clinically significant neurobehavioural differences between children exposed to either prenatal methadone or heroin, although there was a trend towards poorer outcomes.33 However, this analysis is limited by the low to moderate quality of the included studies. The Maternal Opioid Treatment: Human Experimental Research (MOTHER) study reported no differences in growth and neurodevelopmental out-come at 36 months between children with either buprenorphine versus methadone exposures or those who received NAS pharmacotherapy versus those with no medication therapy for NAS.34
There is no current national guideline or consensus from national bodies to suggest a follow-up plan for babies with NAS. Variability exists in short and long-term follow up arrangements from unit to unit and region to region as well as inter-nationally depending upon the difference in prevalence, local impact and available resources. Studies to assess these aspects are essential to encourage clinicians to come together to further develop manage-ment strategies and follow-up services in their individual units or neonatal networks.35-37 There is a need to collaborate with obstetricians (to start management antenatally including maternal education) as well as general and community paediatricians and public health departments to develop services specific to the need of their local population. These developments will go a long way to help this group of patients, which become almost a ‘lost tribe’ as soon as they are discharged from the neonatal unit and lost to meaningful follow-up.
With regards to antenatal management, we would like to highlight a dedicated antenatal clinic offered to pregnant women with alcohol and substance misuse problems in our obstetric department. This is a joint clinic between the Hospital Intervention Liaison Team (HILT) and the obstetric team (led by an obstetric lead consultant). HILT is a support service for people coming to the hospital who have alcohol or drugs related problems. It provides a liaison between hospital and community services to help with various therapeutic interventions. Specific to pregnant women with such problems, HILT and the obstetricians aim to offer appropriate support to allow pregnant women to minimise the risks as much as possible and to make the most of the available opportunities. They coordinate multi-agency working to provide a comprehensive package of support for the best possible outcomes for mothers and babies. The women are identified through the community midwifery team and are referred to the clinic. Over the years this collaboration has helped to reduce non-attendance rates, better prepare for delivery and address any safeguarding concerns for mother and baby.
Future directions
Given the impact of NAS on families, health care and society, there is a strong need to focus future research into developing a further pathophysiological understanding of this complex problem.
At present, all NAS cases are generalised into the same kind of screening, monitoring and treatment categories as those for opioid withdrawal. The scoring or monitoring tools need to be simplified and modified according to the type of drug used (opioid or non-opioid). The further evaluation of pharmacological versus non-pharmacological interventions are required to provide a holistic package for these families, with an emphasis on maximising community-based family integrated support systems rather than prolonged hospitalisation. Although widely used, morphine may not be the most suitable drug to counteract withdrawal symptoms and other pharmacological agents would need to be studied with comparative designs. There has been some growing evidence to suggest advantages of buprenorphine. The research is also needed in long-term health outcomes including physical, neurodevelopmental, behavioural and psychological impact. Researchers have found it difficult to account for the potential confounding of maternal polysubstance use. Standardised corroborated maternal assessment is probably required in order to take some of these variables into consideration. Studies to clarify timelines for the onset of NAS and the relationship between the severity of symptoms and the maternal dose and fetal biotransformation of medication prescribed to the mother (eg methadone) are also needed.
Summary
Alcohol and substance misuse in reproductive age women continues to be a significant public health problem that has been further compounded by its increasing incidence in pregnant women. NAS is not a new entity but the knowledge gain in this problem area has not been in line with the various other confounding factors that have contributed to its evolving disease profile (polydrug use, prematurity, associated blood-borne viral infections, other chronic illnesses related to smoking and obesity, mental health issues as well as different management strategies across the world). Although the evidence is still insufficient to support an association between any particular diagnostic or treatment approach and its impact on long-term neurodevelopmental outcome, there is justification to consider providing a collaborative multidisciplinary approach starting during the antenatal period and continuing well after discharge from the hospital. This kind of approach will help to address issues more rationally and reduce the knowledge gaps in this disease. The emphasis should be to bring parents on board with the ongoing management and to reduce maternal-infant separation by developing better transitional care and community-based support systems. Future research should also focus on the genetic impact on the severity of NAS.
Or read this article in our
Tablet/iPad edition
- Maternal substance misuse is common and poses a significant threat to the exposed infant.
- In utero drug exposure may result in NAS. Infants with NAS often have long and costly hospital stays and prolonged separation from their mothers.
- A collaborative multidisciplinary approach should aim to involve parents and reduce maternal-infant separation by developing better antenatal, transitional care and community-based support systems.
Also published in Infant:
