

Who looks after neonates with intestinal failure in the UK? A survey of practice
Intestinal failure (IF) is a grave condition that carries extensive morbidity and mortality. A multidisciplinary team approach has been shown to be associated with improved survival; however no clear framework for the management of neonates with IF exists in the UK. In order to determine the clinical care arrangements for infants with IF, a questionnaire related to place of care, multi-professional and paediatric gastroenterology involvement was distributed to clinicians at surgical care units within the UK using an online survey tool.
Rebekka JonesMD, MRCPCH
Neonatal Transport Fellow
Pamela Cairns
MBBCh, FRCPCH, MRCP, MD, MSc
Consultant Neonatologist
pamela.cairns@uhbristol.nhs.uk
Neonatal Intensive Care Unit, St. Michael’s Hospital, University Hospitals Bristol NHS Foundation Trust
Intestinal failure (IF) is a devastating condition in which the gut is either dysfunctional or too short to absorb sufficient nutrients for survival and normal growth. The most common causes of IF in the neonatal population are:1
- necrotising enterocolitis (NEC)
- gastroschisis
- malrotation with volvulus
- intestinal atresia
- Hirschsprung’s disease.
Most commonly short gut occurs as a result of extensive bowel resection, the need for which is only apparent at surgery. Neonatal IF itself carries considerable morbidity and mortality and may be complicated by other health problems such as prematurity.2,3
These babies will require parenteral nutrition (PN) for months and potentially years. A proportion may eventually undergo intestinal transplant. They need consistent, meticulous care in order to maximise the likelihood of eventually achieving enteral autonomy while avoiding IF-associated liver disease in the meantime. A multidisciplinary approach to intestinal rehabilitation encompassing fully integrated care by fostering coordination of surgical, medical and nutritional management has shown to be associated with improved survival.4
Currently, no clear guidelines exist in the UK for the management of infants with IF and the service provision model of surgical care for the neonatal population varies greatly between surgical centres. The Department of Health neonatal toolkit (2009),5 which includes a set of principles for high quality neonatal services, and the House of Commons Public Accounts Committee report (2008)6 both endorse the principle of neonatal care being organised as part of a managed clinical network. As a result, neonatal surgical care is provided in designated neonatal surgical centres, within a managed network of care. However, although neonatal surgery services should be co-located with neonatal intensive care units (NICUs), frequently surgical and specialised paediatrics services are geographically separate from neonatal services, which might hinder optimal multidisciplinary collaboration.
Aim
The aim of the survey was to establish where and by which professionals preterm and term infants with IF are looked after in the UK.
Methods
A list of paediatric surgical centres that provide surgical care to neonatal patients was compiled. Subsequently, the consultant paediatric surgeons with a special interest in neonatal surgery from each centre were identified by reviewing hospital websites and information available on consultants from the British Association of Paediatric Surgeons (BAPS) website.
Paediatric surgical consultants were contacted via email with an invitation to complete the survey through a link in the email. Up to two reminders were sent to non-responders. If no response was received after three emails, an alternative contact from the centre with a special interest in nutrition (consultant neonatologist or paediatric gastro-enterologist) was contacted and invited to complete the survey. Invitations were sent out between January and July 2016.
The questionnaire consisted of 10 questions relating to two fictitious cases of short bowel syndrome: a preterm infant and a term infant with a series of suggested answers for each question (FIGURE 1 ).
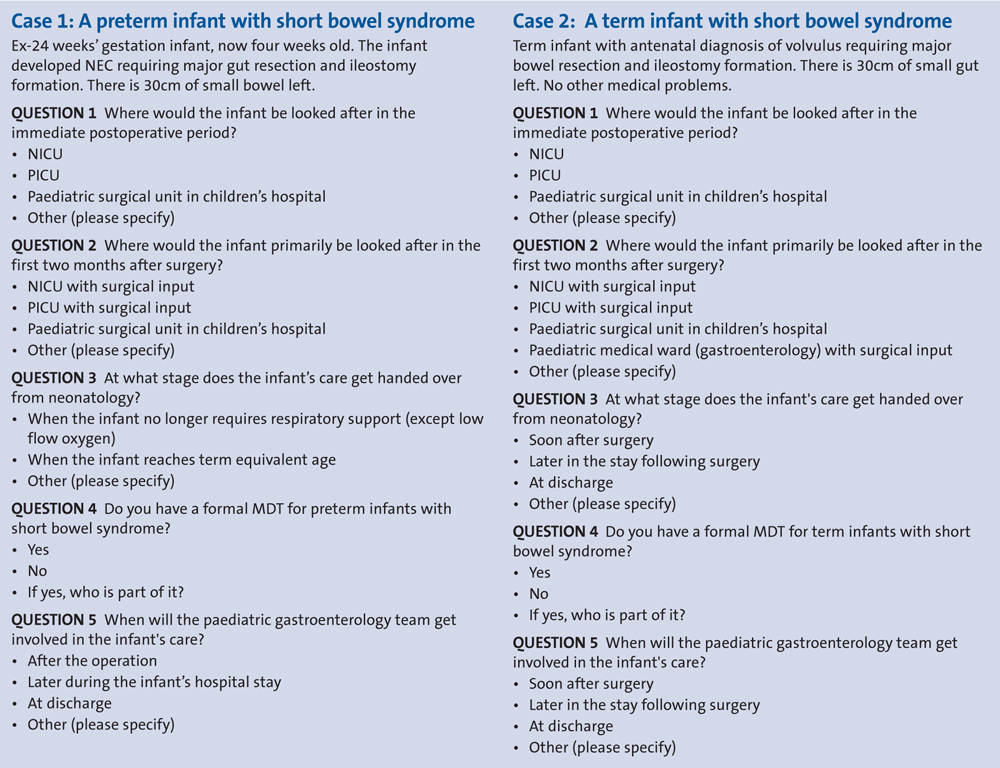
FIGURE 1 The questionnaire comprised 10 questions relating to two fictitious cases of short bowel syndrome: a preterm infant and a term infant, with a series of suggested answers for each question.
Results
Twenty-four responses were received pertaining to 22 out of 25 (88%) centres with one response per centre for 20 units and two responses per centre for two centres. Responses came from 21 paediatric surgeons, two consultant neonatologists and one paediatric gastroenterologist.
Postoperative care setting
Preterm infants are more likely to be managed in a NICU in the immediate postoperative period than term infants (91% vs 71%) (FIGURE 2 ). They are also more likely to remain in a NICU in the first two months (83% vs 29%).
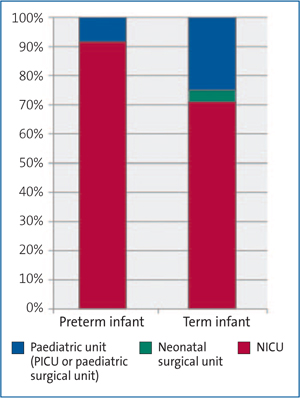
FIGURE 2 Care in the immediate postoperative period.
Term infants are more likely than preterm infants to be cared for in a paediatric cot (paediatric intensive care unit, or paediatric surgical ward; 25% vs 4% of hospitals). Both term and preterm infants would be cared for in a paediatric surgical unit at one children’s hospital for their entire postoperative course.
Transfer of care from neonatology
The transfer of care from primarily neonatology to surgery and/or gastro-enterology was variable. For preterm infants, 21% reported that care would be handed over from neonatologists when the infant no longer required respiratory support (except low flow oxygen), 38% responded that this would be when the infant reaches term-equivalent age and 21% reported other time points relating to the infant’s due date with responses varying from one to six months post due date. Eight per cent reported that the infant remains under neonatal care with input from other specialists.
In comparison, care of term infants was handed over soon after surgery in 33% of responders and later in the infant’s stay by 54%. Four per cent reported that ongoing care would be jointly managed between the neonatology, gastroenterology and surgical teams.
Paediatric gastroenterology involvement
Although in the majority of institutions the gastroenterology team would become involved soon after the operation in term babies (75%), this was not the case in preterm infants where it would occur in only 46% (FIGURE 3 ).
In one hospital the gastroenterology team would only become involved prior to discharge on home PN for both term and preterm infants.
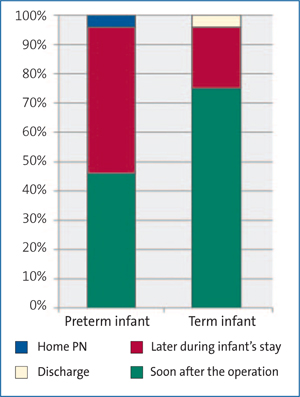
FIGURE 3 Paediatric gastroenterology involvement.
Formal MDT management
Eighty-three per cent of institutions reported that formal MDT management was taking place at their centre for term infants with slightly less (75%) for preterm infants. These consisted of consultant neonatologists, paediatric surgeons, paediatric gastroenterologists and dietitians in most centres. Some centres also reported to have a pharmacist, a specialist nurse and a psychologist on their teams.
Discussion
Using a simple online survey, it was possible to obtain important information from the majority of centres providing care to infants with IF in the UK regarding the service provision to this group of highly complex patients.
The analysis revealed large variation across the country, particularly in the care of preterm infants. Although it is not surprising that preterm infants were more likely to remain in a NICU rather than a paediatric environment, they are also less likely to benefit from MDT management that includes a gastroenterologist. Although there is no specific framework for the management of infants with IF there is convincing evidence showing that intestinal rehabilitation programmes delivered through MDTs reduce morbidity and mortality in paediatric patients with IF.7 Preterm infants with IF are a particularly challenging group to manage as they are uncommon, may have multiple pathologies and more prone to complications such as IF-associated liver disease.8 As many teams now work with an on-service system, rotationally being responsible for inpatient management, each individual clinician may have relatively limited experience in this area. The advantages of a multidisciplinary nutritional team include consistency of approach, more discussion between specialties, continuity of care, earlier treatment of complications and learning from the accumulation of experience. In addition, communication with families is enhanced by consistency across specialties.9 Currently few preterm infants will have data added to national databases such as the British Artificial Nutrition Survey (e-bans; www.e-bans.com). This skews the information available if these databases only contain information from survivors who have been transferred to gastroenterology care.
In a number of centres, MDT working may be limited as a result of geographical constraints, ie neonatal care being provided in a separate hospital from other paediatric specialties. Management in a paediatric ward may enable greater involvement of paediatric gastroenterologists and other specialists early. Equally there are some advantages to having postoperative babies with IF being initially cared for on neonatal units, over and above the requirements of prematurity. Examples include supporting mothers with long-term pumping and storage of breast milk, relative protection from infection (in comparison to a paediatric ward), medical skill at placing percutaneous long lines in small babies with poor veins and nurses skilled in developmental care. Variation in place of care should not, however, lead to variation in standard of care and it is concerning that this seems likely.
There are some important limitations to this survey. The results are based on individual responses to two illustrative cases. We do not have data on care and outcomes of actual patients. Thus although we may infer that the variation is likely to lead to variation in clinical outcomes, we have no direct evidence of this from the study. Despite this, we think our data demonstrates the large variations in service provision between centres and highlights the need for a clear framework of practice for this patient group.
Conclusion
There is wide variation in the care setting and multi-professional involvement for the management of infants with IF in the UK. Early formal collaboration of neonatologists, paediatric surgeons, gastroenterologists and dietitians from soon after surgery is likely to benefit patients in order to ensure optimum management of infants and to improve short- and long-term outcomes.
Or read this article in our
Tablet/iPad edition
- This survey found wide variation in service provision for neonates with intestinal failure in the UK.
- In particular, preterm infants, who often suffer from considerable additional morbidity, have delayed involvement from multidisciplinary teams (MDTs).
- This study sets the scene for further work on outcomes, morbidity and mortality in infants who have wider MDT input earlier on.
Also published in Infant:
