

Delivery room cuddles for preterm babies: should we be doing more?
Early delivery room contact between a preterm baby and a parent is now offered more frequently in units across the UK but it is yet to be accepted as standard care. This article presents data from the neonatal unit at Great Western Hospital in Swindon regarding time to first parental contact, a suggested standard operating procedure for facilitating a delivery room cuddle and four case studies written by parents about their first contact with their preterm babies.
Sarah Bates
Consultant Paediatrician and Neonatologist
sarah.bates16@nhs.net, @SarahBates18
Lucie Edwards
Neonatal Unit Sister
Charlie Peters
Neonatal Unit Staff Nurse
Pippa Morrish
Midwife
Kirsty Ashton
Medical Student
Harriet Nicholas
Foundation Doctor
Charlotte Sullivan
Consultant Obstetrician
Department of Women and Children’s Health, Great Western Hospitals NHS Foundation Trust, Swindon
Preterm birth is a leading cause of neonatal morbidity and mortality; strategies to optimise outcomes for this vulnerable population are essential.1 The benefits of parental contact, through skin-to-skin or kangaroo care, are well documented.2 Parental contact and voice seem to encourage cardiorespiratory stability, improve breast milk supply and provide long-term cognitive benefits for the baby.3-5 The benefits for parents are similarly well evidenced: improved parenting skills, reduced anxiety and improved parental wellbeing.5,6
When a baby is admitted to the neonatal unit (NNU) the family-centred/integrated care approach entails that the parents remain central to all that we do. Perhaps we have unintentionally lost sight of this in the delivery room, as focus has been on prompt post-stabilisation transfer to the NNU, separating baby and parents. Some teams endeavour to ‘show’ the parents their baby briefly en-route to NNU, possibly allowing a brief touch. There is then an indeterminate amount of time until the parents can be with their baby. This can lead to parental stress, additional anxiety, loss of control and potential long-term bonding issues.7 Evidence suggests the intimate contact that usually happens immediately post ‘normal’ term birth may represent a sensitive period for programming future physiology and behaviour.2
Given the benefits of parental contact and family-centred/integrated care, are we missing a key opportunity in our urgency to get the baby to NNU? Could we do things differently?
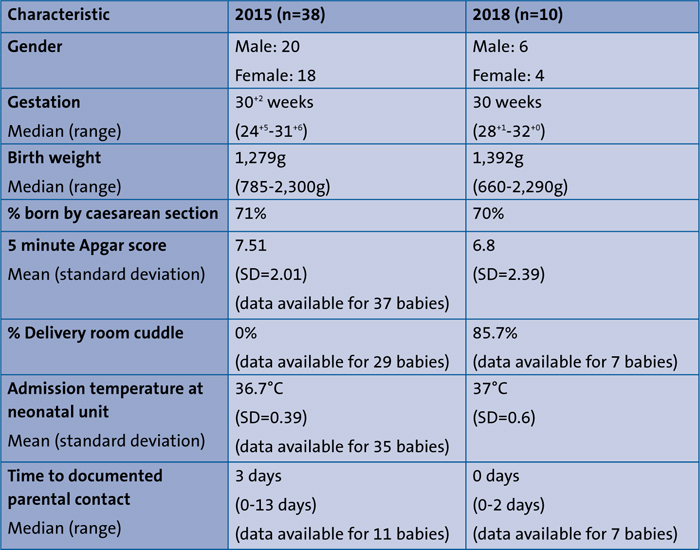
TABLE 1 A comparison of the two study cohorts.
The delivery room cuddle
The delivery room cuddle (DRC) allows the mother to hold her baby with skin-to-skin contact (through a bag, when necessary) for a period prior to departure to NNU. Stabilisation of the airway, breathing and circulation (ABC) remains the priority but once these are established, the baby is placed on the mother’s chest close to her face, with respiratory support maintained by the neonatal team. This takes planning and excellent communication between all members of the perinatal team: the procedure of transferring the baby, providing respiratory support and monitoring the baby should be discussed beforehand with clear guidance for each individual’s role.
The parents should be briefed and photos and/or video footage recorded according to parental wishes. The mother is encouraged to kiss and touch her baby, to support transfer of the maternal microbiome to the baby.8 Throughout the cuddle, the parents are updated and the baby is supported, observed and monitored closely. A suggested standard operating procedure for the DRC is seen in FIGURE 1, although some elements are likely to differ across units depending upon space, teams and equipment.
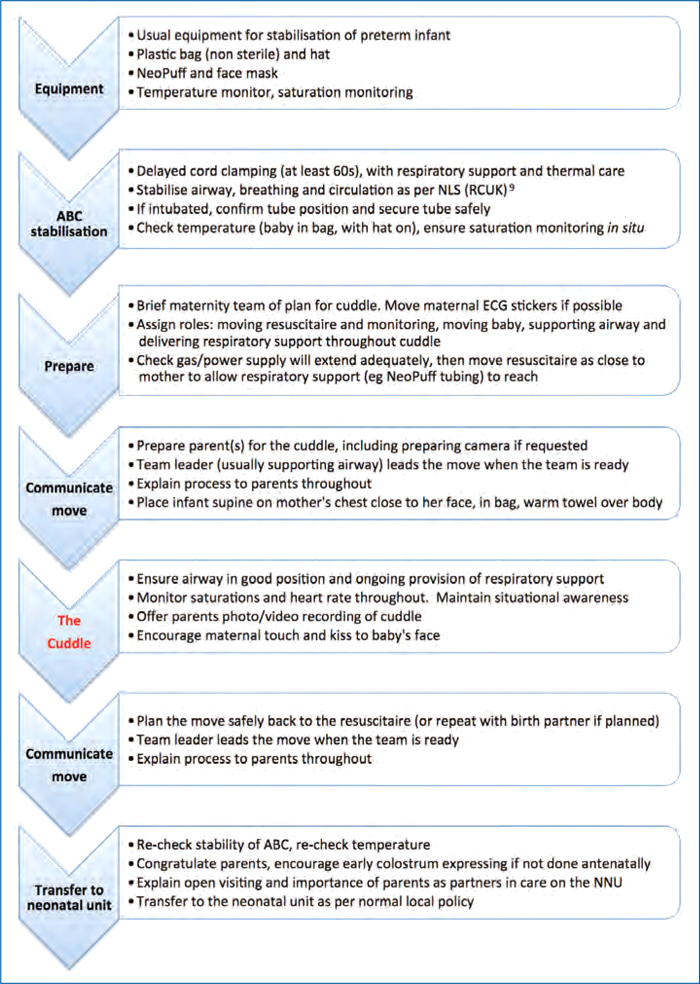
FIGURE 1 The standard operating procedure for the preterm delivery room cuddle.
Methods
The Great Western Hospital (GWH) in Swindon, Wiltshire, averages 4,500 births per annum. It has a consultant-led maternity unit and an 18-cot local neonatal unit (LNU) operating within the South West Neonatal Network.
Data were collected from BadgerNet for two cohorts of babies admitted to the NNU at less than 32 weeks’ gestation: from 1 January to 31 December 2015, and from 1 August to 30 November 2018, which represented the historical change in culture of offering the DRC. The data concerned gender, gestation, birth weight, mode of delivery, Apgar scores and admission temperature. Neonatal and maternal notes were sourced to determine whether the babies had a documented DRC and, if not, how long it was until their first documented parental cuddle.
Data on provision of the DRC were not available for nine babies in the 2015 cohort, of whom five were outborn. Of the 29 babies with notes available, none had a documented DRC. The time until first documented cuddle with the parents ranged from five hours to 13 days, with a median of three days. These data were only available for 11 babies; eight babies were either repatriated from or transferred to another hospital in the postnatal period and 19 had no documentation of a cuddle with parents anywhere in their maternity or neonatal notes. It is possible that more babies were offered earlier contact with their parents but it was not documented.
Delivery room notes were not available for three babies in the 2018 cohort, of whom two were outborn. Of the seven babies with notes available, 85.7% (all but one) had a documented DRC. The time until first documented cuddle with parents after delivery ranged from 0 days (at delivery) to two days, with a median of 0 days.
DRC case studies
Four parents have kindly consented to share their very personal and special stories. Each gives a unique perspective on the DRC and contains a medical summary of the neonatal course, followed by the parental voice on their experience. Each parent expressed that the motivation for sharing their story was to encourage the wider neonatal community to offer more delivery room parent-baby contact. They feel that this early parental contact, the cuddle, really does matter.
Amie and Lillie-Rose’s story
Extremely low birthweight baby with a 19-year-old first-time mum
- emergency caesarean section at 28+1 weeks weighing 695g due to severe intrauterine growth restriction
- moderate condition at birth, received inflation breaths and thermal care during 60 seconds of delayed cord clamping (DCC), Apgar scores of 7, 10 and 10
- intubated at nine minutes, surfactant at 15 minutes, mother-baby cuddle at 21 minutes old
- ventilated using NeoPuff via an endotracheal tube (ETT), stable in air with good saturations throughout
- admitted to NNU at 30 minutes; temperature 36.4°C
- Extubated to continuous positive airway pressure (CPAP) at 45 minutes
- received maternal colostrum within one hour of birth
- ex utero transfer to tertiary neonatal intensive care unit (NICU) at 12 hours of age for birth weight <800g.

Amie and Lillie-Rose during their DRC.
Amie says: “I never thought she would come 12 weeks early. I felt so frightened – I didn’t know if she would survive. I remember being in theatre feeling so panicked, seeing her and thinking how small she was. Then I remember the doctors bringing Lillie over and putting her on me in the plastic bag. She had one eye open looking at me. Holding Lillie changed everything – it made me feel much calmer. I can’t really explain it, it makes you feel complete, it makes you feel positive, as if everything could be OK. Holding Lillie made me feel strong, and I knew that I could do it, I knew I could be a mum.
“The next time I could cuddle her was 48 hours later, as Lillie went to Bristol. We were apart but I didn’t feel the separation so badly because I had already held her, the bond was instantly formed and I felt calm and attached to her. The photos and videos of the cuddle were amazing.”
Ashley, Scott and Luke’s story
The first preterm baby born in a family of five following multiple obstetric complications
- emergency caesarean section at 33 weeks’ gestation weighing 2,397g after preterm labour with major obstetric complications including substantial antepartum haemorrhage
- born in good condition, 60 seconds of DCC, Apgar scores of 6, 8 and 9
- significant early respiratory distress requiring positive end-expiratory pressure (PEEP) in up to 100% oxygen
- mother-baby cuddle at 11 minutes old, supported with facemask PEEP throughout
- oxygen requirement was initially 90% but within two minutes of being on his mother he was able to be weaned onto air, and saturated well throughout
- father-baby two minute cuddle with a brief rise in oxygen requirement to 30%, otherwise stable
- admitted to NNU at 27 minutes; temperature 36.5°C
- briefly required CPAP otherwise an uneventful neonatal course.

Scott, Luke and Ashley during their DRC
Ashley says: “I loved that you told me he was more stable on me – it made me feel useful, in a situation where you feel a bit useless and out of control. Nothing about Luke’s birth was ‘normal’ – holding him was the only bit of normal and it meant so much. With all the commotion, it mattered to me to know that Luke recognised the connection and was better when he was on me. The cuddle is such a special personal, family moment. I was worried about postnatal depression and bonding and I think if I hadn’t had the cuddle I might have felt distant and unconnected but I didn’t – I felt so connected to him straight away. So many experiences are lost during an emergency preterm delivery; it is wonderful that the first cuddle is not one of the things we missed out on.”
Jess, Russ, Florence and Matilda’s story
Twins born in 2015 when DRC was not standard care
- primigravid mother, dichorionic-diamniotic twins
- spontaneous preterm labour and vaginal births at 30+3 weeks’ gestation weighing 1,279g and 1,333g
- both born in good condition with good Apgar scores, short period of DCC. Both required PEEP with up to 30% oxygen
- DRC not offered with either twin
- admitted to NNU by 20 minutes of age; temperatures 36.5 and 37.2°C
- transferred (for capacity reasons) to another LNU shortly after birth
- first cuddles several days later.

Russ touching Matilda for the first time at three hours old.
Jess says: “Florence arrived at 5:39am and was stabilised in the room before being taken to SCBU and I remember my husband looking between her and me while I focused on delivering Matilda. Neither of us were particularly aware of her leaving the room, something we can’t quite believe now. Matilda was delivered at 5:45am and held over me only very briefly before being taken away.
“We were then taken back to the delivery room expecting to be told when we could see the girls without much of an update on them for what felt like ages. Around 8:30am we asked if we could see them. Matilda was already being prepared for transfer and we were able to touch them through the incubators but no one mentioned holding them.

Jess holding Florence for the first time at two days old.
“Florence was transferred later that day during which time I saw her again but did not hold her. Throughout this time we felt we didn’t know what to do to help our babies. It was two days before I could be re-united with the girls. Needless to say this was a completely surreal experience and the longest two days of my life. I longed to hold them. My husband was struggling with us being apart and he wasn’t offered the chance to hold the girls when he visited without me. I felt quite detached from them. Looking back I think we were both in shock although we didn’t realise it at the time.
“When we were eventually reunited I was able to have my first kangaroo care cuddle. I can still remember the blissful feeling of Florence’s body on my chest, feeling her breathing and her warmth and hearing her little noises. I can’t look at that photo without tears coming to my eyes. We finally felt like we could start bonding with them.
“When I think about their premature arrival, I feel that having my babies placed on my chest as they arrived is the bit we were denied. It’s the bit you imagine when you’re pregnant, when you imagine the birth. It feels like what makes you a mother, especially as they were often so calm and content when we did kangaroo care, it feels like how it’s meant to be.”
Laura, Paul and Miller’s story
Emergency delivery at 29 weeks. Sadly passed away at two days of age
- multiparous mother, reduced fetal movements reported
- caesarean section due to pathological cardiotocography at 29 weeks’ gestation weighing 1,185g
- born in poor condition, Apgar scores of 3, 4 and 8
- received inflation breaths during 60 seconds of DCC
- intubated at 14 minutes for poor respiratory effort, ventilated in up to 90% oxygen
- mother-baby cuddle at 21 minutes lasting six minutes. Ventilated via ETT throughout. Oxygen requirement fell from 90% to air, as saturations improved markedly during the cuddle
- admitted to NNU at 28 minutes; temperature 37.5°C
- increasingly unwell over first 12 hours requiring increasing ventilatory and inotropic support, with very little respiratory drive and hypotonia. Transferred to tertiary NICU for escalation of intensive care
- blood cultures confirmed a listeria infection. Continued to deteriorate and later developed significant haemorrhagic brain injury
- passed away when care was re-orientated at 48 hours of age
- apart from the initial DRC, the only time the parents were able to hold their baby was at the point of withdrawal of care.
Laura says: “After a healthy pregnancy, at 29 weeks I decided to attend hospital just to put my mind at rest as baby Miller hadn’t moved for most of that day. After a night of monitoring, it was decided that we should deliver. My husband Paul was away for work and wasn’t going to make it in time for the delivery.
“After Miller was born I got to see her for the first time while the team was attending to her and I was then handed Miller to hold up by my chest. It was so amazing to hold her and feel her next to me; I kissed her little face and saw how beautiful she was. The team talked to me throughout and told me that her signs were better when she was on me and I definitely took comfort in knowing that she was happy with me. My mum took some photos, which we later sent to my husband. It felt so lovely to have just a few moments together and it is what I would have wanted after any type of birth.
“Later that same day I was able to visit Miller on the special care unit, it was upsetting to see our little baby on support and I touched her little hand through the incubator. We didn’t realise how sick Miller was until later that evening when the team came to tell me that she needed more support and would be transferred to Bristol. I was so worried for her and couldn’t follow straightaway as I hadn’t been discharged. It was a long night not being with our baby but the next day I visited her in Bristol. We were told that Miller was very sick, she had contracted listeria and the prognosis was not good. It was devastating to know that she would not survive. The next morning we made the decision to switch off the support. Paul and I had the amazing but heartbreaking opportunity to hold Miller while she passed away. I initially thought I wouldn’t be strong enough to do it but actually it brought a kind of peace to us in those last few moments and the main thing is that I wanted her to know we were there for her at that time.
“We couldn’t have anticipated what was going to happen to Miller and looking back it was so important to have had a hold and cuddle with our beautiful baby in the delivery room.”
Discussion
Although each case study is deeply per-sonal and individual with a unique perspective on the DRC some common themes emerged for parents and these are summarised in TABLE 2.
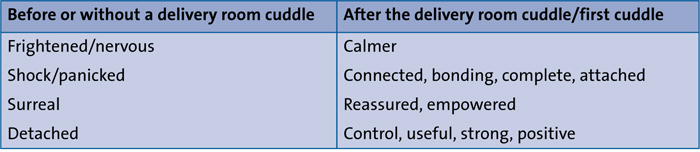
TABLE 2 Summary of themes from the case studies.
Impact of the DRC on the preterm baby
Studies have described how, during parental contact, a newborn baby experiences maternal heart sounds, rhythmic maternal breathing and warmth, all of which offer gentle stimulation across the auditory, tactile and thermal sensory systems. This may moderate perception of pain and help achieve cardiorespiratory and temperature stability.2,4,10 Our experience of delivering this intervention would concur: we have not seen any adverse impacts on cardiorespiratory stability, nor any compromise to thermal care. Indeed, in Miller and Luke’s cases, both achieved significant improvement in their respiratory status during parental contact (both going from a high oxygen requirement into air). These cases demonstrate that a DRC can be safe, feasible and perhaps even beneficial in even the smallest (Lillie-Rose) and sickest (Miller) of preterm babies.
Impact of the DRC on the parents
In the case studies the parents eloquently describe the powerful impact that the DRC can have. They discuss the importance of early establishment of the vital mother-baby bond and how contact with their baby helps to alleviate maternal stress, providing reassurance at a frightening and traumatic time. Ashley talks of how so little about a preterm delivery is normal. The DRC can be an incredibly important aspect of ‘normality of birth’ and, as such, is very highly valued by parents.
Research has suggested that parents of premature babies are twice as likely to suffer from postnatal depression as parents of full term, healthy babies.11 The case studies describe how the DRC can have a positive impact on perinatal mental health; potentially mitigating some of the traumatic effects a preterm delivery can have on a family. However, as is so poignantly described in Laura and Miller’s story, some babies will not survive and this is often impossible to predict at the point of delivery. When a baby becomes extremely unstable parental contact is often limited or unfeasible and sometimes only possible at the point of re-orientation of care. Facilitating a DRC for all babies at the start of life could mean that, for the few who cannot survive, the only parental cuddle and hold is not at the end of life.
Separation and postnatal transfer
In the UK it is not uncommon for newborn babies to be transferred, either because of capacity issues or because they require more prolonged intensive care. It is rare for a mother to be transferred simultaneously with her infant, usually because of ongoing maternity or obstetric needs. Inevitably, a significant geographical distance separates the family unit, for hours and even days. The impact this can have upon family bonding and parental wellbeing is described honestly and emotively by Jess. However, the value of a DRC in mitigating some of the negative impact of separation is important, as described in Amie and Lillie-Rose’s story.
Teamwork and the DRC
Facilitating the DRC and embedding this as standard of care can require a significant shift in team culture. It needs great focus on teamwork, human factors, communication and planning of practicalities. It can be adopted into any neonatal and maternity setting but will require leadership for implementation and adaptation to each unique clinical environment.
The obstetric and midwifery perspective
Although healthcare professionals are very aware of the importance and benefits of early skin-to-skin contact, until recently it has been difficult to achieve this for preterm babies. Implementation of the DRC has not interfered with obstetric practice or increased complications. New mothers have emphasised how early contact with their baby has had a beneficial effect on their perinatal mental health, especially when they are separated for neonatal care.
At the essence of midwifery is advocacy and markedly so for women and their families at a time where they are exceptionally vulnerable. When women feel scared and events are out of their control, we should restore some of that control; let us recreate normality and remember that at the heart of everything is a mother and a newborn baby.
Where do we go from here?
Many teams across the UK are beginning to implement the DRC and should be encouraged to share their experiences of safety, feasibility and efficacy including the parental voice whenever possible. A multi-centre study of feasibility and efficacy of the DRC with outcome measures of neonatal and parental wellbeing would be welcomed.
Conclusion
We have described how the provision of a DRC for preterm infants has increased in our unit. The four case studies have helped to demonstrate how this intervention can impact so positively on the babies and their families. We conclude with the parental voice: “When I think about a delivery room cuddle, it just makes sense – why wouldn’t you do this? It makes all the difference even if it just takes 30 seconds.”
Dedication and acknowledgement
This article is dedicated to the memory of Miller.
The authors are indebted to the parents who shared their personal stories of preterm birth and for their commitment to increasing awareness of the importance of the DRC. Thanks also to:
- Professor Paul Clarke (neonatologist, Norwich) and Emma Allen (parent of preterm twins) for pioneering work in inspiring us to implement the practice of the DRC.
- The maternity and neonatal teams from GWH for embracing this practice and providing family-centred care from the moment of birth.
Or read this article in our
Tablet/iPad edition
- The delivery room cuddle (DRC) has a strong positive impact on babies and their families.
- Parents describe how early contact with their baby helps bonding and stress relief at a traumatic time.
- Perinatal teams are encouraged to embrace the DRC to provide family-centred care from the moment of birth.
Also published in Infant:
