

Multidisciplinary antenatal and perinatal palliative care
Perinatal palliative care is a fairly new subspecialty within the areas of paediatric palliative care, neonatology, fetal medicine and obstetrics. Involving parent-centred, non-judgemental shared decision making, it aims to provide high levels of comfort and care for babies and holistic multidisciplinary support for their families. The focus of antenatal and perinatal palliative care should be to support and enable families to spend time with their baby, make informed choices and build memories. Children’s hospices have proved extremely valuable in this area of palliative care.
Fauzia PaizeMbChB, MRCPCH, MD
Consultant Neonatologist, Neonatal Unit, Liverpool Women’s NHS Foundation Trust
fauzia.paize@lwh.nhs.uk
Pregnancy, more often than not, is a very much desired event in people’s lives. It is a time of hope and expectation of the impending life that is soon to join yours. This can begin as soon as the viewing of a positive pregnancy test. The worlds of expectant parents suddenly change whether this is the first child or one that is joining others. Does the family need to move house? Change car? Work family-friendly hours? There is an assumption in our society that pregnancy results in a baby that is going to share a fulfilled life with its parents. When a pregnancy goes wrong it can be a devastating event and also an isolating and lonely one. Sometimes parents need to make decisions that they never thought they would have to think about and meet healthcare professionals that they never knew existed.
When devastating news is shared about an unborn baby, a baby is delivered very prematurely or a perinatal event occurs that requires life-saving interventions, the toll on families is immense and needs to be approached with great sensitivity and support. Perinatal palliative care is a fairly new subspecialty that involves parent-centred, non-judgemental shared decision making and aims to provide high levels of comfort and care for babies and holistic multidisciplinary support for their families. Antenatal and perinatal palliative care should aim to support and enable families to spend time with their baby and build lasting memories.
The challenges
There are huge challenges in the world of perinatal palliative care and despite there being established national frameworks and clinical pathways for palliative care after birth1-8 there remains no unified pathway guiding care for women and families.
If a problem is detected antenatally there is the potential for discordance between the antenatal findings and the possibility of the affected organs being able to sustain life. Antenatal diagnostic uncertainty is a significant challenge. It is impossible to accurately predict what the lungs of a baby with a diaphragmatic hernia will do, or the circulation of a baby with transposition of the great arteries with an intact ventricular septum. This leads to a need for parallel planning – hoping for the best while planning for the worst. The baby may do A, B or C when it is delivered so we need to have a plan in place for each eventuality.
Babies can deteriorate and die with great speed, much faster than older children or adults. This may be due to organ failure post-birth or death due to withdrawal of life-sustaining treatment. Both can make death seem very sudden, highlighting the importance of parallel planning and a management plan to introduce effective and planned palliative care support for these babies and their families. The time parents have to spend with their baby alive can be very short and precious so there is only one opportunity to get it right.
Some pregnancies end due to a termination of pregnancy following the detection of a serious problem such as anencephaly. Babies from these pregnancies are often born alive and may have supportive needs but we must not forget that these families will need emotional support too.
Challenges arise if mothers are not fit to be transferred to a neonatal unit when they have health needs of their own. For multiple birth pregnancies, there may be one or more sick babies to care for alongside babies who do not have a life-threatening condition. There may be queries about organ donation – something neonatal departments are not always fully prepared for, although donations do successfully happen. One baby may die in utero triggering off bereavement during an ongoing pregnancy.
Fathers have their own specific needs; they often struggle to take in information and feel very torn between the needs of the baby and their partner.
For parents the grief that ensues can be lonely. When a baby dies very soon after birth there can be a lack of support from their usual circle of friends and family. With little understanding of what they have gone through, most do not know what to say or how to provide comfort.
There are different and often multiple teams and services involved in this particular area of health care, for example obstetricians, midwives, neonatal nurses, neonatologists and fetal medicine specialists. These are sometimes based in different hospitals and so there is a need for high levels of efficient, compassionate and accurate communication to prevent individuals from having to repeat their stories over and over again. Neonatal transport services deserve consideration, as there may be risk of resuscitation or death on route. We should consider the transportation of babies with palliative care needs in the same way as babies that are being transferred for critical care needs; they should be included in care planning pathways.
Making a better plan: antenatal advanced care planning
Integrated multidisciplinary care with effective communication and documentation is key for this area of palliative care. Families should be provided with value-neutral information about all options, including termination of pregnancy, continuation with palliative care or continuation of pregnancy with an active postnatal care plan. It is important to openly discuss parents’ priorities, hopes and fears, in order to facilitate shared decision making.
Conversations about the most common outcomes and the process of pregnancy and delivery should take place and be documented. Establishing and maintaining trust is crucial in this evolving relationship; continuity of care with the same clinicians is advised. It is vital to communicate clearly with all parties about the certainties and, importantly, the uncertainties of each case.
Parallel planning enables clinicians to compassionately explore care with the parents. Items that should be covered include: the event of death in utero, deciding the mode and timing of delivery, monitoring during labour, resuscitation plans at birth depending on the condition of the baby, active or palliative care after birth, symptom management, further tests, and the possibility of transitioning to a community setting if the baby shows signs that it may survive for longer than expected. Families may ask about organ or tissue donation and this should be supported if appropriate, with involvement of the local specialist nurses for organ donation.
Decisions do not always need to be made at the time of the first meeting; plans can evolve over several meetings and should be formalised in a written advanced antenatal palliative care and birth plan. The wider multidisciplinary team (MDT) should be introduced (fetal medicine, neonatology, children’s hospices, palliative care teams, the referring centre labour ward, community midwifery and general practice teams) and importantly the plan should be shared among the MDT, ideally kept in the maternal handheld notes, as most fetal medicine units are regional services seeing families across a wide geographical area. This is a difficult environment to maintain high standards in, but clarity of communication and efficiency of documentation with all parties is key at this stage.
Children’s hospices
Children’s hospices are extremely valuable in this area of palliative care and work in partnership with local fetal medicine, neonatal, community midwife and palliative care teams. The hospice can enable families to be emotionally supported throughout their pregnancy. The family can make plans to transition to the hospice immediately after discharge from hospital or be supported at home by hospice staff. Families can visit the hospice prior to their baby being born to see if this is somewhere that they would like to spend time with their baby and extended family (figure 1).
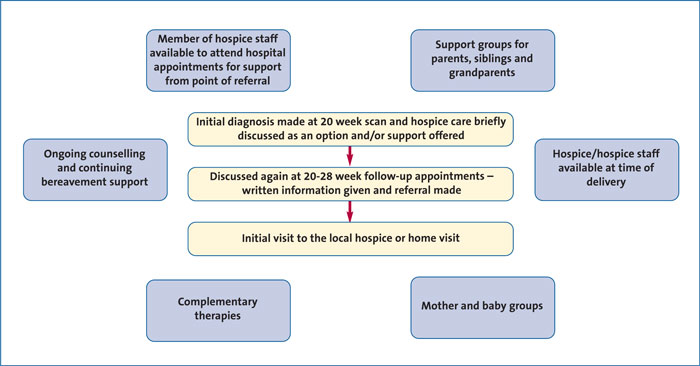
FIGURE 1 Children’s hospices: a way to provide supportive antenatal care.
Children’s hospices can offer a home-from-home setting allowing families as much privacy or support as they need and provide one-to-one, family-led palliative and end-of-life care to babies with a variety of complex needs (table 1). They allow some normality in a supported environment, such as parents being able to sleep in the same room as the baby. This allows them to balance their expectations and independence; it gives potential for fulfilling their hopes of parenthood.
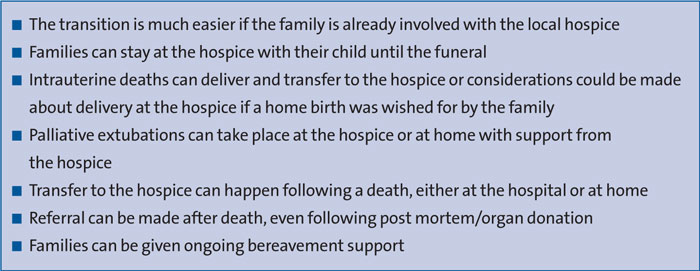
TABLE 1 End-of-life care at a children’s hospice.
Children’s hospices can offer to have household tasks taken care of so that parents can spend time more with their baby (eg meals and laundry). Staff are also experienced in memory making, symptom control, supporting families at home as a step down from hospital for those babies that may not die imminently, offering respite care at home, and arranging local services to provide ongoing support and end-of-life care.
Following death most hospices have cooled bedrooms and a cooled ‘cuddle cot’ that enable parents to spend time with the deceased baby at the hospice or at home with support. Hospices also aid in funeral planning, registering the birth and death of the child and ongoing bereavement support for the extended family, including siblings and grandparents.
Conclusion
Parallel planning and clear documentation is vital for this area of medicine to function well. Respect for the values and choices of parents are central to providing compassionate, tailored supportive care. Healthcare professionals should work towards being able to offer those choices.
Or read this article in our
Tablet/iPad edition
- Parallel planning and clear, honest documentation is vital for antenatal and perinatal palliative care.
- Parents who have chosen to continue their pregnancy following antenatal diagnosis of a life-limiting condition should be offered multidisciplinary support from professionals with experience in perinatal palliative care.
- Personalised antenatal, birth and postnatal care plans should be drawn up and appropriately communicated to all centres likely to be involved in the family’s future care
Also published in Infant:
