

Keeping Mothers and Babies Together: implementing a single, simplified pathway for at-risk infants
Despite falling birth rates, admissions to neonatal units are increasing. National drivers aimed at reducing term admissions have concentrated on identifying reasons for admission and tackling each individually. National and local guidelines differ in their approach to managing infants at risk of postnatal compromise dependent on the specific risk factor identified, adding to the confusion and leading to significant variation in postnatal care delivery. A more radical approach to managing all infants at risk of postnatal compromise focusing on simplifying and standardising postnatal care for the late preterm and more vulnerable term infants is described.
Shanthi ShanmugalingamConsultant Neonatologist and KMB2 Co-Lead
shanthi.shanmugalingam@nhs.net
Charlotte Edgington
Paediatric Trainee and KMB2 Trainee Representative
Lorraine Gallagher
KMB2 Programme Manager
Rose Villar
Consultant Midwife and KMB2 Co-Lead
Royal Free London NHS Foundation Trust
Despite decreasing birth rates, admissions to neonatal units continue to rise.1 Admission to the neonatal unit is a traumatic experience for families, with long-term impact on breastfeeding rates, infant-parent bonding and perinatal mental health.2 The Atain (avoiding term admissions into neonatal units) programme1 has garnered energy nationally to address this issue by identifying the main reasons for admissions (respiratory conditions, hypoglycaemia, jaundice, asphyxia) and providing tools for action. Variations in clinical guidelines add to the challenges of delivering clinically coherent care. This variation extends to the management of late preterm (34+0 to 36+6 weeks’ gestation) infants who are at higher risk of postnatal compromise and who are often separated from their mothers pre-emptively. To date, the focus of maternity and neonatal teams has been to address each individual cause separately. Indeed one of the quality improvement pathways for the Maternal and Neonatal Health Safety Collaborative focuses on reducing term admissions with hypoglycaemia. However, in order to truly address the barriers to delivering consistent high quality postnatal care, we need to adopt a more radical approach.
Unwarranted variation in health care
Variation in clinical management that promotes individualised patient-centred care is described as warranted variation and is positively encouraged. Unwarranted variation cannot be explained by a patient’s symptoms or needs and often reflects variation in individual clinical knowledge or how the systems within departments work. While the impact of unwarranted variation on clinical outcome and efficiency is well described,3 the challenge remains to identify the root causes of unwarranted variation within any system.4
Unwarranted variation within a single trust
The Royal Free London NHS Trust has embraced the group model of care5 to drive down unwarranted variation that may be harmful to patients and families and adversely impact effective healthcare provision. The Royal Free London NHS Trust has two acute maternity units: Royal Free Hospital with a co-located special care unit and Barnet Hospital with a co-located local neonatal unit. The Keeping Mothers and Babies Together (KMB2) team was tasked with identifying and addressing unwarranted variation in the care of term and late preterm infants across the whole trust with the primary aim of reducing avoidable admissions to the neonatal unit.
We observed the clinical journey for infants with risk factors for postnatal compromise (‘at-risk’ babies) as defined in the Newborn Early Warning Trigger and Track (NEWTT).6 This highlighted the complex pathways we were expecting our teams to navigate. Locally, each guideline differed as to the frequency and length of NEWTT observations depending on the risk factor. For example, observations were required at one hour then two-hourly for meconium and sepsis observations (with different regimes for significant (thick) and non-significant (thin) meconium) and four-hourly for late preterm infants. Observations were discontinued at 12 hours for babies with meconium stained liquor, 24 hours for infants of mothers who screened positive for group B Streptococcus with no specified time for late preterm infants. Regimes also differed across sites for the same risk factor. In essence, we were making it really hard for our teams to deliver consistent high quality clinical care.
Discussions with parents and parent diaries highlighted how disempowered and vulnerable they felt in looking after their ‘at-risk’ baby. The need for standardisation and simplification was clear.
The KMB2 clinical pathway
The Royal Free KMB2 pathway centres on standardising care through the introduction of a single, simplified pathway focusing on first hour care of all infants and the care of at-risk infants. Each aspect was tested and refined using a model for improvement7 before incremental introduction of another facet of the pathway. Key elements include:
- standardised assessment of early respiratory distress
- first hour care bundle
- orange ‘hat-risk’
- unified observation regime for all at-risk infants and revised NEWTT chart
- written information for families.
Standardised assessment of early respiratory distress
Often it is the most junior member of the neonatal team who assesses the infant with early respiratory distress. They can find it challenging to differentiate between infants transitioning to ex-utero life who will settle rapidly and those with significant symptoms requiring neonatal admission. We proposed the development of a standardised assessment tool for respiratory distress. This first aspect of the KMB2 pathway was the most controversial. Scores for assessment of early onset respiratory distress focus on escalation
of respiratory support8-10 with little in published literature or expert consensus guiding clinical decision-making around the need for admission to the neonatal unit. We adopted a pragmatic approach by exploring senior clinicians’ unspoken internal framework of clinical assessment and then refined the tool through staff focus groups and feedback forms during testing (FIGURE 1). Criteria-based assessment of work of breathing, heart rate and pre-ductal saturations guide decision-making to one of the following:
- immediate admission
- review within 30 minutes
- standard KMB2 care.
The respiratory distress assessment tool gives junior doctors confidence to assess infants with respiratory distress and guides management plans. Junior doctors’ feedback included: “easy to follow” and “wish we had this from the beginning.”
They also noted that following the standardised assessment enabled them to avoid admission and reduce the number of babies having septic screens.
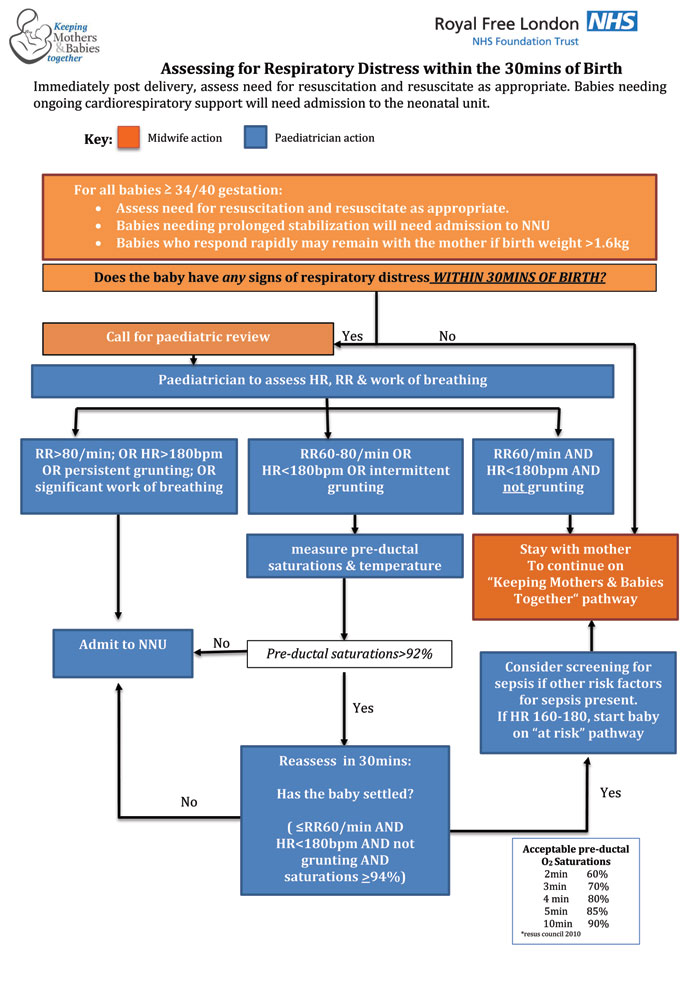
FIGURE 1 A tool for criteria-based assessment of work of breathing, heart rate and pre-ductal saturations to guide decision-making.
First hour care bundle
In initial discussions, all midwives were confident that they consistently initiated skin-to-skin, supported the first feed and undertook a set of observations within the first hour of birth for all infants. However, in situ observations revealed significant variation in practice with regard to how skin-to-skin is administered (specifically in relation to infant thermoregulation) and in ensuring mothers are supported in giving the first feed. Observations within an hour of birth were often delayed or missed altogether. A significant amount of time was spent in documenting care delivery, taking the midwife away from the mother and her newborn. A single-sided document (FIGURE 2) was introduced with specific detail on each aspect of first hour care, together with the appropriate actions if there were any concerns. All that was required for documentation was circling and initialling of actions, freeing the midwife to support the family during this crucial first hour.
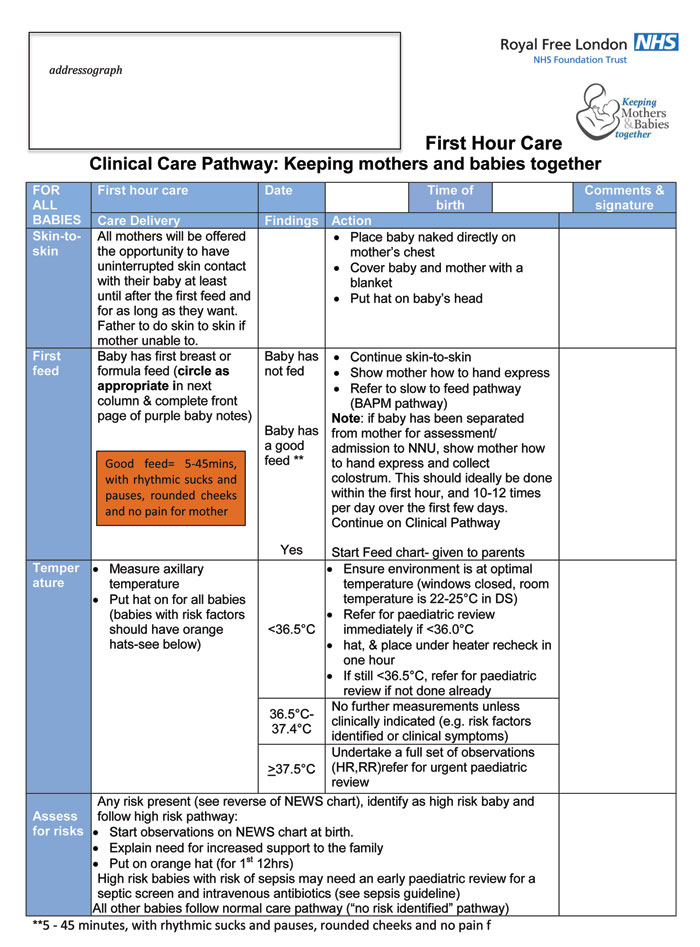
FIGURE 2 The first hour of care: care delivery and appropriate actions.
Orange ‘hat-risk’
Recognising the challenges of looking after approximately eight mother-infant dyads on the postnatal ward, we aimed to make it easy for staff to identify families needing enhanced postnatal care. Modelled on Thaler’s nudge theory,11 we introduced orange hats to easily identifying at-risk infants. This simple measure has been enthusiastically welcomed with staff saying that the hat highlights at a glance those infants needing additional support, as soon as you walk into a bay. Parents reported feeling reassured with some mothers also stating that the hat made them feel empowered to ask for additional assistance.
Unified observation regime for all at-risk infants and revised NEWTT chart
The complexity of knowing which observations are needed for which infant and for how long was removed by the introduction of a single observation regime for all at-risk infants. Initial concerns regarding increased workload due to increased observations for some infants were quickly allayed as staff became confident and efficient in applying a consistent observation schedule.
The NEWTT chart was also modified to not only include tick boxes for all risk factors (facilitating documentation of why enhanced postnatal care is indicated) but also a summary of the pathway actions from admission until discharge (FIGURE 3). Staff reported that this made a significant impact on the way they were able to plan each shift.
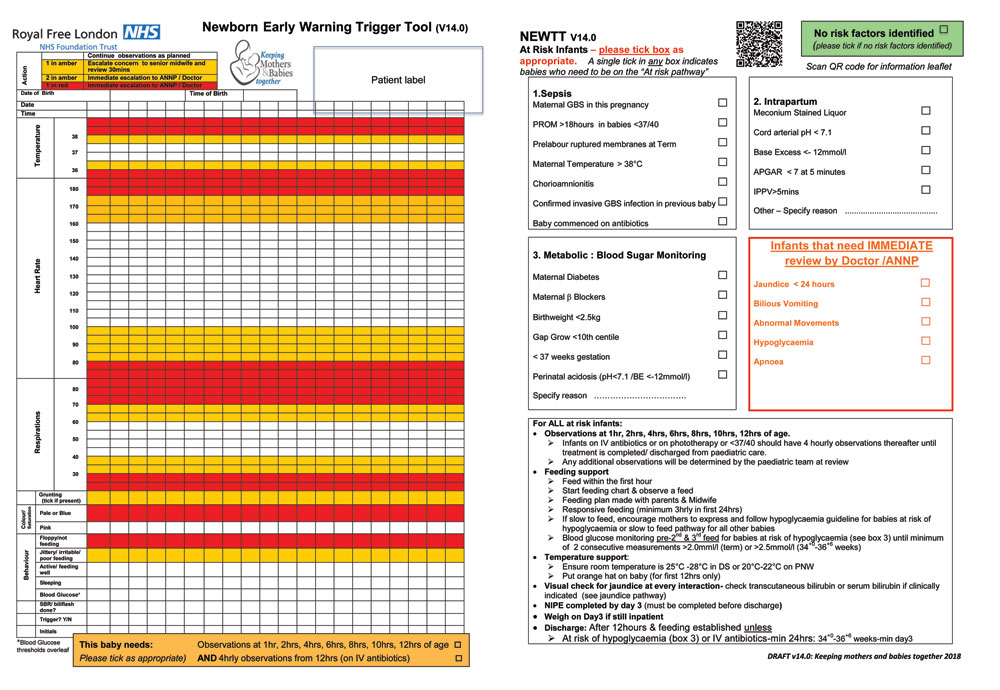
FIGURE 3 The modified NEWTT chart.
Written information for families
Families are crucial members of the caregiving team and while parent diaries confirmed that team members consistently discussed care, the lack of written information and nuances in the way information was delivered often led to feelings of vulnerability and confusion. Simplifying the at-risk pathway enabled the development of a single parent information leaflet that is given to parents with greater consistency than the multiple different leaflets available previously. The use of a QR (quick response) code allows parents to download the leaflet directly onto their mobile phones. Posters with the QR code have been placed in the antenatal clinic, delivery suites and postnatal wards so that parents are able to access the information as soon as a risk factor is identified. For example, mothers with gestational diabetes admitted to the delivery suite are already aware that their babies will need blood glucose monitoring, will have an orange hat and that they will receive support with feeding. All families are also given a feed chart to document feed frequency and volumes incorporating details of how to know if feeding is going well. Both families and staff have found this extremely useful and this has enhanced parents’ confidence in establishing feeding as they transition to community teams.
Co-design
Collaboration with families and staff has been central in producing the pathway. The pathway team includes a father. Parent diaries were used to explore families’ experience of postnatal care focusing specifically on emotional hotspots. Additionally, focus groups and one-to-one interviews were used to inform the development of the pathway documents.
The parent voice proved a powerful tool in driving change and challenging staff preconceptions. Co-design with families resulted in a common language and purpose for staff and families enabling rapid adoption of the new pathway. For example, staff were worried that the introduction of the orange hat-risk would result in families feeling stigmatised. Parental feedback was overwhelmingly positive leading to its rapid adoption. This approach continued during every plan-do-study-act (PDSA)7 cycle with parents and frontline staff providing real time feedback in the form of questionnaires and video feedback. This allowed rapid revision and retesting to hone the accessibility and utility of the pathway.
Measuring impact
Pathway testing commenced in November 2017 with the modified NEWTT chart. The final aspect introduced was the standardised assessment tool for early respiratory distress. Each PDSA cycle was used to refine the tool and is offset by continuing interrogation of all term admissions with respiratory distress, to ensure that admission has not been inappropriately delayed. Absolute numbers for term respiratory distress are small and as such it is too early to demonstrate a significant effect on admission rates. However, fewer infants are being separated from their mothers during the crucial first hour after birth (FIGURE 4).
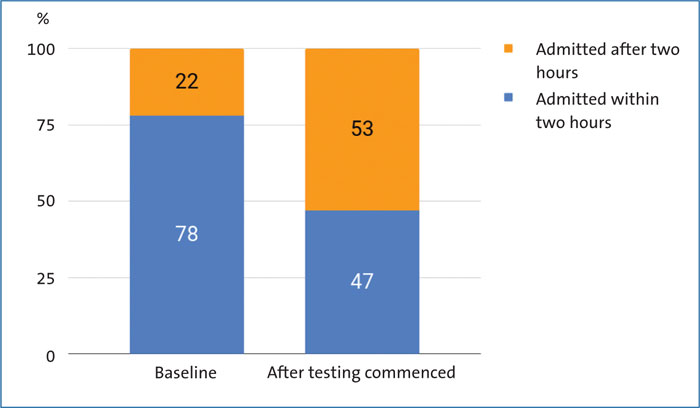
FIGURE 4 Percentage of term infants admitted to the neonatal unit for respiratory distress who were admitted within two hours of birth. Fewer infants were separated from their mothers during the crucial first hour after birth.
In the six months before implementation of the KMB2 pathway, our baseline rate of neonatal admissions was 8.3% of all babies born ≥34 weeks’ gestation. Since commencing testing in November 2017, this rate has fallen to 6.5% representing a reduction of over 20%. As we continue to implement and embed, and ultimately digitise this pathway, we hope this rate will continue to fall.
The length of stay of mothers on the postnatal wards has not increased. Additionally there has been no increase in accident and emergency attendances or readmissions within the first seven days of life, suggesting that these infants are being safely managed on the postnatal wards with a smooth discharge to the community midwifery teams.
Conclusion
There is a significant gap between work ‘as done’ versus work ‘as imagined’ (ie care delivery as defined by clinical guidelines) in the care of newborns in our maternity units. The multitude of different, often conflicting guidelines, makes it difficult for staff to deliver consistent high quality care. Reducing unwarranted variation by the implementation of a simplified, single KMB2 pathway makes it easier for staff to focus on clinical care delivery. Using quality improvement methodology for implementation with emphasis on co-design with parents and staff has resulted in a model of care that is useable, accessible and being embraced by families and healthcare teams. As we move to concentrate on sustainability through digitisation, we hope to continue to see more mothers and babies safely kept together after birth. You can follow our journey on twitter @MumBaby2gether.
Acknowledgements
The KMB2 team is a multiprofessional team of neonatologists (Drs Marice Theron, Isioma Onyekpe, Karen Job and Cheentan Singh), midwives (Marianne Renkin, Ran Liang, Rujina Khatun, Lori Fuller, Sabha Rafiq, Meg Wilkinson and Jenny Woods), infant feeding consultants (Jenny Marshall and Jenny Whelehan), and a parent representative (Michael) brought together with the common goal of keeping mothers and babies together when safe to do so. The maternity and neonatal teams at both Barnet and Royal Free Hospitals have positively embraced the KMB2 pathway. Their energy, drive and passion has been matched by the families who have contributed to producing this pathway. Thank you to each and every one of you. Your continuing contribution is making a difference.
Or read this article in our
Tablet/iPad edition
- Standardising care by introducing a single, simplified pathway for all ‘at-risk’ infants reduces unwarranted variation and avoidable neonatal admissions.
- The parent voice is extremely powerful in driving change. Co-design with families enabled rapid adoption of the new pathway.
Also published in Infant:
