

Champagne and bloody taps: can we improve the success rate of neonatal lumbar punctures?
Neonatal lumbar puncture is an essential and common procedure. Its relatively high failure rate can have a significant impact on patients, parents, clinical teams and healthcare resources. NeoCLEAR is a large randomised controlled trial investigating whether success rates are affected by positioning, or timing of stylet removal. If successful, this trial may contribute to the future of neonatal care by reducing the need for repeat lumbar punctures, avoiding prolonged antibiotic courses and minimising postnatal hospital stays.
Andrew Marshall
Manish Sadarangani
Alexandra Scrivens
Rachel Williams
Jean Yong
Ursula Bowler
Louise Linsell
Virginia Chiocchia
Eleri Adams
Ed Juszczak
Charles Roehr
Neonatal lumbar puncture (LP) is a common1 but technically challenging procedure; hence the traditional promise of champagne if the sample obtained is perfectly clear – a ‘champagne tap’. Usually, however, the reward remains elusive, either because the cerebrospinal fluid (CSF) is blood-stained (a ‘bloody tap’) or because no sample is obtained at all.
Getting it right is crucial: LP is the only reliable test for meningitis and gives important information about other conditions (eg mitochondrial disease), as the clinical signs are non-specific.2 Meningitis affects at least one in 4,000 neonates and carries high rates of mortality (approximately 10%) and morbidity (approximately 25%).3 Obtaining an interpretable CSF sample is essential for diagnosis, which subsequently determines treatment and follow-up.
Success rates for neonatal LP are only 50-60%4 compared with 80-90% in older children.5 Most of us have witnessed the consequences of a failed LP: the diagnostic uncertainty, the possibility of repeat procedures causing further discomfort for the patient and distress for the family. If meningitis cannot confidently be ruled out, cautious management plans to cover for possible meningitis tend to involve prolonged courses of intravenous antibiotics, often requiring several venous cannulae and/or long-lines. Wider implications for healthcare systems include the risk of antimicrobial resistance and increased length of hospital stays, with their associated costs.6 The potential for delayed discharge also impacts the whole family as plans for returning home with their newborn are rewritten.
Despite suboptimal success rates, the technique most commonly used for neonatal LP has remained essentially unchanged since the procedure was first described over 125 years ago.7 Previous neonatal research has investigated several modifications to traditional LP technique: the use of sedation, analgesia, additional training, sitting position, formulae for needle insertion depth, early stylet removal, and ultrasound guidance.8
Most of these studies have either been observational (low-grade evidence, open to bias) or too small to generate firm conclusions, or have made recommend-ations that appear difficult to implement widely.9 For these reasons, two easily-implementable modifications to current LP practice have been chosen for investigation.
1. Sitting versus lying position
FIGURE 1. Sitting increases the space between the spinous processes and may increase lumbar CSF pressure. It has been used in babies as small as 1,000g without additional cardiorespiratory instability.10
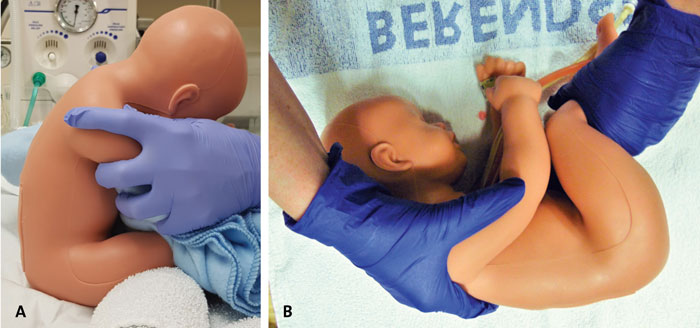
FIGURE 1 A manikin in the sitting and lying positions. A) Sitting position with a towel under the knees to improve lumbar flexion, shoulders held still and the head resting on a blanket. B) Lying position with thighs/legs held to improve lumbar flexion and shoulders held still. Photos taken using LumbarPunctureBaby manikin, Simulab, USA.
Early versus late stylet removal
The stylet (a thin piece of metal that sits inside the needle) is traditionally removed ‘late’, once the tip is assumed to have reached the CSF. Some evidence supports removing the stylet ‘early’, after going through the skin, and then slowly advancing the needle until CSF flows out. This may reduce the chances of inserting the needle beyond the CSF space into the venous plexus and obtaining a blood-stained sample.5
For both modifications there is observational evidence of improved success rates, but a large randomised study is needed to conclusively prove any significant benefit.
NeoCLEAR
NeoCLEAR – Neonatal Champagne Lumbar punctures Every time: A Randomised controlled trial – is one of the first well-powered randomised trials to investigate neonatal LP technique.11 The NeoCLEAR team is aiming to recruit 1,020 patients. Most infants under neonatal care will be eligible to take part (TABLE 1). To investigate both techniques simultaneously, NeoCLEAR uses a ‘2x2’ design where infants are randomised to one of four techniques (TABLE 2). The study team will regularly visit sites to train staff in each of these techniques. Outcome data (TABLE 3) are collected before and after the LP(s) and at discharge. The primary outcome is the proportion of infants with a successful first LP, ie obtaining a CSF sample with <10,000 red blood cells/mm3.
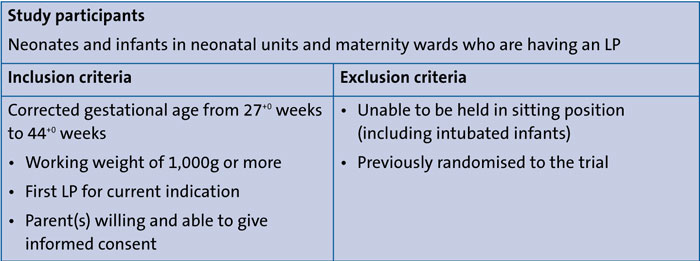
TABLE 1 The NeoCLEAR trial: inclusion and exclusion criteria.

TABLE 2 The ‘2x2’ trial design.
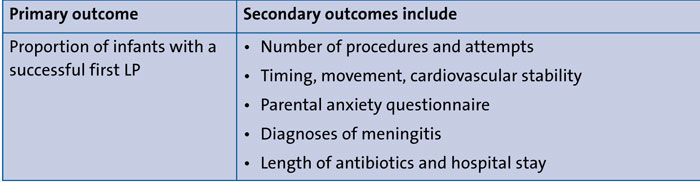
TABLE 3 Primary and secondary outcomes. Outcome data are collected before and after the LP(s) and at discharge.
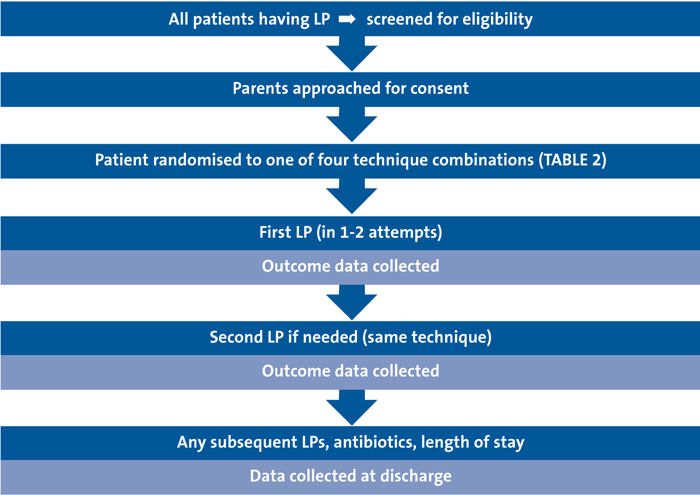
FIGURE 2 Overall flow of trial participants.
The pilot phase of NeoCLEAR is underway, involving 10 units in the UK and aiming to recruit 250 patients by spring 2019. Beyond this, further study sites may be able to join for the remainder of the trial. The overall flow of trial participants can be seen in FIGURE 2. Progress updates, study documents, and training videos for different techniques can be found on the NeoCLEAR website (www.npeu.ox.ac.uk/neoclear). Parents and patient representatives, including colleagues from a local neonatal charity (www.ssnap.org.uk), have been involved in designing this trial. The trial is funded by the National Institute for Health Research Health Technology Assessment (NIHR HTA), co-ordinated by the National Perinatal Epidemiology Unit Clinical Trials Unit (NPEU CTU), and sponsored by the University of Oxford.
Or read this article in our
Tablet/iPad edition
- Despite suboptimal success rates, the technique for neonatal lumbar puncture (LP) has remained essentially unchanged for over 125 years.
- NeoCLEAR is one of the first well-powered randomised trials to investigate neonatal LP technique. The primary outcome is the proportion of infants with a successful first LP.
Also published in Infant:
