

Therapeutic hypothermia in neonates: do we cool outside the entry criteria?
This survey reviews current cooling practice of level 3 neonatal units (NNUs) in the UK with regard to treatment of babies who do not fulfil the existing cooling entry criteria. We collected replies from 78% of tertiary NNUs. More than 80% of tertiary units consider cooling or have cooled babies from at least one of the ‘outside the entry criteria’ categories. An analysis of the replies is discussed.
Ourania PappaMSc Neonatal Medicine Student, Cardiff University
Neonatal Fellow, Leeds Teaching Hospitals NHS Trust
ourania.pappa@nhs.net Aliki Bogiatzopoulou
ST7 Neonatal Grid Trainee,
North West Deanery Elisa Smit
Consultant Neonatologist, Cardiff and Vale University Healthboard
Senior Clinical Lecturer MSc Neonatal Medicine, Cardiff University Archana Mishra
Consultant Neonatologist, Royal Bolton Hospital NHS Trust
Therapeutic hypothermia: what is already known?
- Perinatal asphyxia (PA) severe enough to cause hypoxic-ischaemic encephalopathy (HIE) and requiring cooling occurs in approximately 1-3.5 per 1,000 births in the UK1
- Systematic reviews have confirmed that 72 hours of therapeutic hypothermia (TH) to a core temperature of 33-34°C initiated within six hours following birth, improves death and disability rates at 18 months2 from 25% to 9% and from 20% to 16%, respectively3
- The vast majority of neonatal intensive care units (NICU) in the UK follow the TOBY cooling guidance and it involves meeting three different sets of criteria4
- Now that TH is known to be effective and without adverse effects, the time has come to investigate whether other groups outside TOBY could benefit from it. A therapeutic ‘creep’ has been observed over the recent years, where TH is being offered outside the accepted cooling criteria5,6
- Small observational studies have reviewed the effectiveness and risks of cooling in further subcategories of babies.
Background
HIE of the term and near-term infant occurring around the time of birth is caused by a combination of diminished oxygen in the blood supply (hypoxaemia) and reduced amount of blood perfusing the brain tissue (ischaemia); the combination of these events generates neuronal injury and glucose depletion. However, HIE is not a ‘stand-alone’ event, but a continuously evolving situation that leads to cell destruction.7
Shoulder dystocia, uterine rupture, cord prolapse, maternal hypotension and placenta praevia are some of the primary hypoxic events that could result in PA. In the newborn brain a lack of adenosine triphosphate (ATP), and functional failure of sodium-potassium pumps leads to increased lactate production cellular oedema and necrosis. Subsequent glutamate accumulation in the synaptic crest leads to calcium influx and further cell death (primary energy failure).8
In the scenario of successful resuscitation and reperfusion, there is a brief period of time when cellular metabolism is restored; however, the initially restored cerebral blood flow becomes again compromised (latent phase) and triggers further apoptosis and inflammatory reaction through accumulation of oxygen free radicals and subsequent mitochondrial collapse, known as the secondary energy failure stage.9
The subsequent apoptosis or necrosis leads to oxidative stress, which is partic-ularly harmful to the neonatal brain, due to high consumption of oxygen during the transition from fetal to neonatal life and low concentration of antioxidants.8 Days or even months after the initial insult, the ongoing inflammatory response in the developing brain leads to impaired neurogenesis, altered synaptogenesis, loss of trophic support and impaired neuronal axonal growth (tertiary phase); all these changes are closely linked to cerebral palsy.10
TH is the treatment of choice for babies with moderate to severe HIE. Systematic reviews since 2005 confirm that cooling reduces death and disability at 18 months of age and increases the number of infants with normal neurodevelopmental outcome.2 TH reduces cerebral metabolism by 5% for every degree of temperature reduction, suppresses oxygen free radicals, reduces apoptotic cell death,11 and extends the duration of the secondary hypoperfusion (latent) phase, which has been linked with improved outcome.12
The majority of NICUs in the UK follow the TOBY criteria to decide on cooling (TABLE 1). In the context of a history suggestive of PA, infants who meet criteria A will be reviewed and assessed to decide whether they meet clinical criteria B. If both criteria A and B are met, amplitude integrated electroencephalography (aEEG) should be performed and if found abnormal within six hours following birth, the baby is eligible for cooling.4
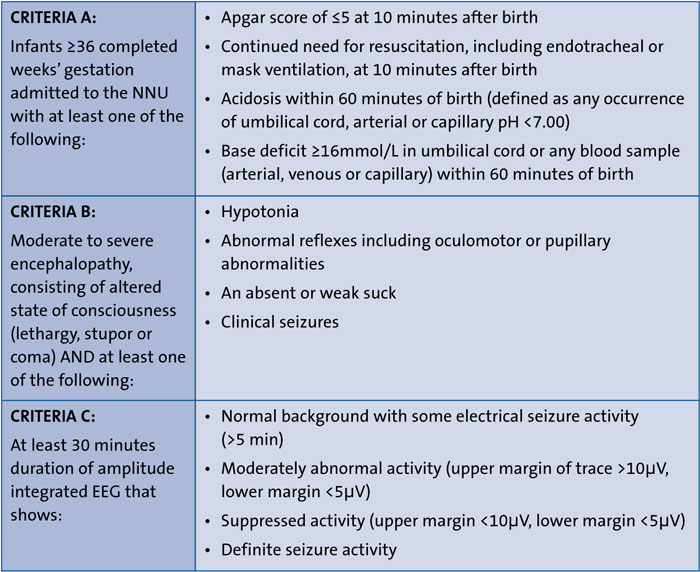
TABLE 1 TOBY entry criteria.4
New challenges: infants who fall outside of current cooling criteria
With TH being a recognised and safe treatment for infants born at or after 36 weeks of gestational age, a therapeutic creep has been observed over the recent years, where TH is being offered outside of the currently accepted cooling criteria.5,6 One of the most crucial aspects when extending criteria to categories that do not fall under TOBY guidance is safety and efficacy. There are ‘grey case scenarios’ that could potentially benefit from cooling, but the literature available is minimal.
Late preterm infants
There are currently no published randomised controlled trials (RCT) to support the use of TH in infants less than 36 weeks’ gestation. The infants who did not meet the entry criteria in two large randomised trials13,14 were not followed up and there was no opportunity to study the outcome of those screened, but not cooled.15 The literature is limited to case series from cooling centres, which anecdotally offer treatment to premature babies from 33-35 weeks’ gestation. There is a large RCT in progress (Preemie Hypothermia for Neonatal Encephalopathy study: NCT01330576) and it aims to compare cooling versus normothermic infants with HIE between 33-35 weeks gestational age with regards to death and moderate to severe neurodevelopmental compromise.16
The short-term outcomes that have been described to date included coagulopathy, hypotension, seizure activity and hypoglycaemia.17 Two recent studies16,17 concluded that the overall mortality after cooling late preterm infants was lower than the rates that have been reported in the large term RCTs13,14 and overall compromise in survivors did not differ from the infants who were cooled fulfilling the entry criteria.17 However, the small sample size is a significant limitation of these studies.
Infants with mild neonatal encephalopathy
There is no widely accepted definition of mild encephalopathy and the criteria to identify the condition vary among clinicians. The underlying mechanism is unclear: secondary energy failure has been seen in animal models of severe and moderate HIE and it is not thought to be a characteristic of mild HIE.18 However, a clear impact on later neurodevelopment has been described.19
There is no original research that reviews the effect of TH exclusively in cases of mild encephalopathy. Kariholu et al analysed pooled data from large cooling trials,20-23 focusing on the subcategory of mild HIE. They concluded that there is no statistically significant difference in either death or neurodisability between the cooled and non-cooled groups. However, the observation of adverse neurological outcomes in almost 20% of the infants with mild encephalopathy in both groups, highlights the not-so-innocent nature of the condition.24
Infants after sudden unexpected postnatal collapse
A sudden early postnatal collapse (PNC) in a previously well term infant is a rare but life-threatening scenario; the reported incidence is 0.03-0.5 per 1,000 live births with very high mortality rate and severe neurodevelopmental compromise in the survivors.6 No clinical trials of TH have specifically addressed PNC and the only cohort study that examined the effects of cooling after such an insult, included 10 infants who had a comparable outcome to the control group of cooled infants fulfilling cooling entry criteria.17 Another study that reviewed 12 infants who suffered PNC, described the importance of differentiating the underlying reasons that lead to collapse before the initiation of cooling. No comments on the potential impact of TH were made on this study.25
Infants identified between 6 and 24 hours
A multicentre RCT was conducted and compared infants with moderate or severe encephalopathy treated with cooling at or after six hours, but before 24 hours, compared with non-cooled infants.26 The analysis of data showed non-statistically significant differences between the two groups. A review of 11 late cooled infants in a UK centre17 did not indicate either favourable or harmful results. Early identification of the cases remains of paramount importance, but in cases of late presentation a thorough approach of the case should be made and careful consideration of risks and benefits.
Infants with surgical conditions
Due to concerns about significant complications (wound healing, cardiovascular compromise and coagulopathy), infants that have undergone surgery have not been included in TH trials. However, congenital cardiac conditions that require surgery and cardiopulmonary bypass, have traditionally been exposed to hypothermia in order to preserve the brain from ischaemia.17 A case series published the findings of a six-year review on asphyxiated babies with congenital heart lesions; 10 babies were cooled, and the intervention was withheld in two of them due to short-term complications. The operative outcome was good and none of the babies has abnormal neurological findings on follow-up.27
One case series that included babies with major cranial haemorrhage, strongly suggests avoiding TH as overall outcome was very poor.17 In the same study, neonates who had undergone abdominal surgery while being cooled, showed no complications from the intervention and neurological outcome was favourable.
Objectives
The aim of this work included the design and distribution of a web-based survey programme (SurveyMonkey) questionnaire to all neonatal networks in the UK, in order to identify all level 3 centres and their current practice with regards to cooling outside the entry criteria.
Survey design and administration
The survey focused on eight questions (TABLE 2) and was designed by the author, OP, a student at University of Cardiff in conjunction with the NNU of Royal Bolton Hospital.
The survey was administered over a six-month period between June-November 2019. It was initially distributed to colleagues with neonatal interest, by being published in one of the newsletters of the British Association of Perinatal Medicine (BAPM) website and two months later by emailing the clinical leads of all level 3 units of the UK. Web addresses were found on either BAPM’s official site or each hospital’s internet page. Neonatal network directors were also contacted directly, and they distributed emails with the survey to all level units of each deanery.
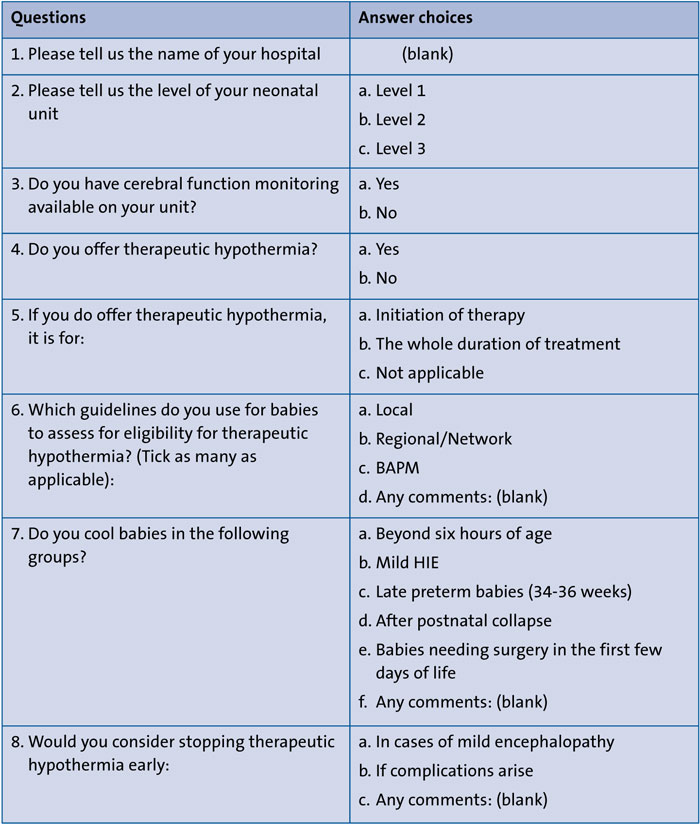
TABLE 2 SurveyMonkey questionnaire and answer options.
Results
A total of 85 responses were collected (FIGURE 1). Twenty-nine responses were from level 2 units that only offer TH for initiation of therapy and they were excluded from the analysis of results. Furthermore, duplicates were not taken into consideration (n=13).
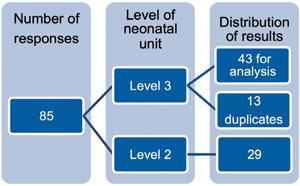
FIGURE 1 Breakdown of responses.
Complete responses were received from 43 out of 55 cooling centres (78.1%). All had the necessary equipment for cerebral function monitoring and offered TH for the whole duration of treatment (100%). The majority of units (83.7%) follow their regional/network guidelines; four perform cooling based on their local/in-hospital criteria (9.3%), two (4.6%) NNUs in Scotland follow their national neuro-protection pathway and one unit (2.3%) follows BAPM guidelines exclusively. TABLE 3 summarises the SurveyMonkey findings for the sub-categories investigated.
In cases when a decision to stop hypothermia was made, 32.5 % of NNUs (14/43) discontinued it in infants with mild hypothermia and 69.7% (30/43) when complications arose. Furthermore, two units stated that they also stop in occasions of reorientation of care.
Discussion
Despite a lack of evidence to support this practice, most cooling centres in the UK now offer TH to babies who do not fit the TOBY guidance. What is the rationale behind this decision and do neonatologists feel confident when extending the cooling criteria?
Many responders commented that their decision to cool or not is based on careful consideration of risks and benefits and also after a thorough discussion with the parents, who were actively involved in the decision-making process (10/43; 23.2%). Moreover, some of them highlighted that the decision depended on each individual consultant’s background and personal choice (5/43; 11.6%) in comparison to some others who highlighted that it was based on team consensus, which includes the majority of the neonatal consultants (3/43; 6.9%). Adherence to cooling protocols has remained of paramount importance in each subcategory. However, there are several challenges when cooling outside the entry criteria. Determination of encephalopathy among preterm infants will need to separate neurologic findings of prematurity from those of encephalopathy and assessment of safety is challenging given the overlap between effects of HIE and hypothermia.
Early identification of babies with mild encephalopathy is also of paramount importance: there have been numerous cases with a normal initial neurological examination, which deteriorated in subsequent hours and even presented with clinical seizures.28 Thus, a lot of clinicians decide to initiate TH, clinically review the baby in regular intervals and even discontinue cooling if deemed necessary. Several responders have mentioned a ‘cooling pause’, which helps them reassess the situation and determine whether there is a consensus that to continue cooling is medically indicated. It is not an actual time pause, but a time interval in which they carefully review the case.
A recent study of 42 cooled babies with mild encephalopathy, out of which 10 had treatment discontinued prior to completion, showed that half had unfavourable magnetic resonance imaging findings, and they also presented with mild motor impairment or language delays on their 24-month neuro-developmental assessment.29
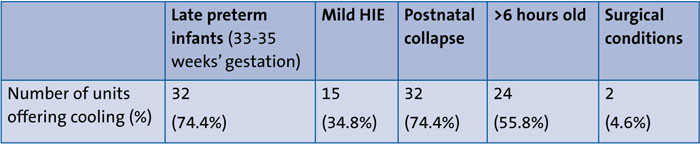
TABLE 3 Number (percentage of total) of cooling centres that offer treatment to babies outside entry criteria.
Infants identified after six hours of life, in the absence of other available treatments or harm, could undergo TH and similar action should be taken for infants who have sustained PNC. Decision making should involve a second senior clinician in conjunction with the parents who should be fully made aware of risks and benefits.30
In the rare occasion of a surgical infant requiring TH, a thorough clinical assessment should be made by a highly experienced neonatal team; case series have shown favourable results apart from babies with major cranial haemmorhage.17 BAPM recently updated its framework for practice in relation to TH and provides some guidance on the categories explored in the survey.30,31
Conclusion
This survey confirms the already observed therapeutic creep, where TH is being offered outside of the currently accepted cooling criteria. Meticulous studies focusing on knowledge gaps are crucial to maximise the benefit of treatment and avoid any potential harm in the process.
Acknowledgements
This article is the end result of the dissertation project by Ourania Pappa: Therapeutic Hypothermia for Hypoxic-Ischaemic Encephalopathy Outside of Standard Entry Criteria: a Review of Literature.
OP would like to thank the University of Cardiff for an exceptionally well organised part-time, online master’s course and the neonatal team for the hard work and support that they provided. Special thanks to the supervisor of the project, Dr Elisa Smit, for her generous contribution in time and expertise.
The survey would not exist without the help and valuable support of Dr Archana Mishra and Dr Aliki Bogiatzopoulou.
Or read this article in our
Tablet/iPad edition
- A therapeutic ‘creep’ has been observed in which TH is offered beyond the accepted cooling criteria.
- Meticulous studies focusing on knowledge gaps are crucial to maximise the benefit of treatment in ‘grey case scenarios’.
- When evidence is limited, the decision to cool must be made by a team of experienced clinicians along with the parents.
Also published in Infant:
