

Technical advances in point-of-care testing to identify haemolysed samples and reduce errors in potassium readings
The normal range for serum potassium in neonates is typically 3.5-6.0mmol/L. Hyperkalaemia (K+) is defined as a serum potassium concentration greater than 7mmol/L. It is a potentially life-threatening condition leading to lethal cardiac arrhythmia that requires immediate interventions to stabilise the neonate and return them to normal electrolyte levels.
Marie HinesInfant Editor
In collaboration with
Werfen
712 The Quadrant, Cavendish Avenue, Birchwood, Warrington, Cheshire WA3 6DE, UK. Tel: +44 (0)1925 810 141. sales.uk@werfen.com

Werfen’s GEM Premier 7000 with iQM3
Hyperkalaemia in the preterm infant is most associated with non-oliguric hyperkalaemia in the first 72 hours of life. It is exacerbated by metabolic acidosis due to exchange of intracellular K+ with extracellular H+, renal impairment and hypovolaemia.1
Haemolysis is caused when the red blood cell membrane ruptures, causing potassium to leak into the surrounding fluid. The main causes for this are deemed to be the fragility of neonatal red blood cells and the capillary sample collection, when the heel is squeezed by the clinician to obtain adequate blood volume. This leads to an elevation in potassium results, meaning that a low potassium may be reported as normal and a normal potassium level will be reported as high. Haemolysis elevates potassium by up to 152%.2
Haemolysis accounts for up to 70% of pre-analytical errors.3 It was found by a study carried out in one academic hospital, that the percentage of haemolysis in the NICU was 39.6-46.4%,4 compared to 8.8-18.1% in the emergency department and 5% in the adult ICU.3,5
When capillary blood samples are haemolysed, an artificially high potassium reading may be given by point-of-care (POC) testing. Unfortunately, POC testing machines are unable to detect haemolysis due to the fact that they use a whole blood sample, rather than a sample which is spun down to expose the cell free plasma. The presence of haemolysis can produce ambiguities and delays in diagnosis and management. It is important for premature neonates especially, that blood samples are accurate and are not wasted. The clinician should not be taking additional samples because blood has clotted or haemolysed. Therefore, where a haemolysed sample is suspected, the first step should be to confirm high serum K+ with a non-haemolysed venous or arterial sample through the central laboratory.
Hyperkalaemia must be treated immediately. All exogenous intravenous solutions such as 10% dextrose with added potassium, or total parenteral nutrition (TPN) must be stopped or re-prescribed accordant to the new readings. It is therefore imperative that clinicians have accurate readings.
When to treat hyperkalaemia
Treatment of hyperkalaemia should begin with performing a 12 lead ECG, or to monitor the continuous ECG. Bloods should be sent to repeat the K+ in the central laboratory and all fluids or drugs that contained or affected K+ should be stopped. ECG changes should be expected to show peaked/tented T waves; wide QRS complex; long PR interval; diphasic QRS complex (sine wave); flat/loss of P waves; VF/asystole.
In severe hyperkalaemia, IV 10% calcium gluconate should be given to stabilise the cardiac membrane and prevent arrhythmias, with the dosage dependent upon the infant’s age.
In moderate hyperkalaemia, salbutamol should be given to move K into cells. Insulin/glucose should also be given to assist with moving K into cells.
In neonates with mild hyperkalaemia, IV furosemide assists with elimination of K+. Nebulised salbutamol assists with moving K+ into cells and calcium resonium also increases K+ elimination.
POC testing versus laboratory testing
POC testing is routinely used by neonatal clinicians. Being able to take smaller samples and get expedited results enables clinicians to make immediate changes to patient care. However, it is well understood that there may be discrepancies between POC and laboratory results.7 This
is due to the different technologies that are used with POC testing.
When using POC testing of samples, specimens cannot be tested for the presence of haemolysis. In the laboratory, the red colour of haemoglobin is routinely measured using spectrophotometric methods when serum or plasma is tested. Haemolysis will be detected and clinicians will be updated with the results. For samples that are not sent to the central laboratory, but are carried out at the point of care, haemolysed samples may be interpreted and treated inaccurately. This can lead to inaccurate therapeutic decisions as well as delays in neonate discharge.8

Degrees of hyperkalaemia depending on age of neonate.6
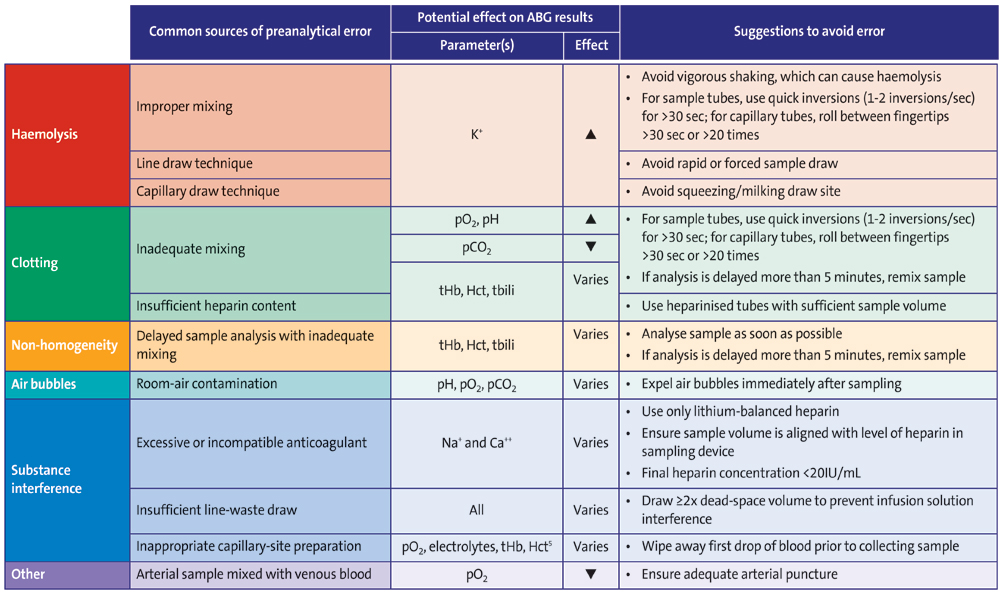
How clinicians may contribute to the reliability of POC blood testing. Up arrowhead = increase result. Down arrowhead = decrease result.
Improving POC analysis
To reduce haemolysis and improve the accuracy of POC analysis, there is a need to consider how clinicians may improve the reliability of point of care blood testing.
- Reducing the risk of pre-analytical errors such as initial error of haemolysis. A clinician is always careful in line and capillary draw technique. When drawing blood samples from a line, it is important that sufficient blood mixed with the saline flush is withdrawn initially, so that the final testing sample does not still contain a mix of saline. When drawing capillary blood, it is important to ensure that the infant is well perfused, with warm peripheries. This allows for a draw that is not squeezed or prolonged, leading to incorrect potassium results, for example. When the sample has been collected, tubes should not be shaken, but gently inverted once or twice per second, or capillary tubes may be gently rolled. Both actions assist in preventing clotting. Haemolysis is the number one source of pre-analytical error and can impact potassium results.9,10
- Procurement needs to ensure that sufficient heparinised tubes are available to clinicians to take samples that have reduced chance of clotting. Any clotting can lead to reduced accuracy of pH, pO2, pCO2, tbili (total bilirubin), Hct (haematocrit) and tHb (total haemoglobin).
- One common issue with some POC blood analysers is that analysis of samples may be held up while the system or performs quality control. This can be a lengthy wait that results in error of tHb readings, Hct and tbili. Clinicians reduce this issue by being aware of the time that their system is due to calibrate and avoid taking samples at that time.
- Air bubbles are a common occurrence and mean that the sample is contaminated and usually will lead to a reading error in pH, pCO2, pO2 or meaning that the sample needs to be repeated altogether because the machine cannot analyse the sample. This leads to increased discomfort for the patient and increased time spent by the clinician.
Werfen’s GEM Premier 7000 with iQM3 POC blood analyser is the first of its kind with the ability to detect haemolysis in whole blood testing at the point of care. The GEM Premier 7000 and its iQM3 quality management system with integrated haemolysis detection provides automated quality assurance with every whole blood sample, continuously and in real time, unlike traditional quality control. In a transformative step toward enhancing patient outcomes in acute care, GEM Premier 7000 with Intelligent Quality Management 3 (iQM3) provides lab-quality detection of haemolysis, in whole blood. iQM3 ensures sample quality across the most common pre-analytical errors (eg haemolysis, clots, bubbles, benzalkonium), detecting haemolysis in 45 seconds to help inform appropriate patient management decisions.
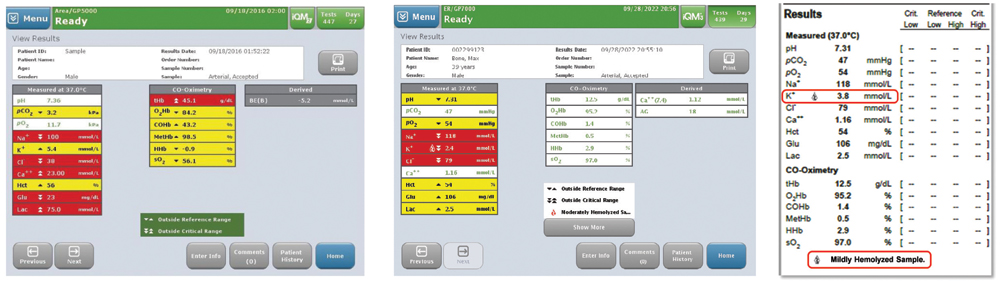
From left to right: The results screen shows true K+; results screen flags haemolysis; and haemolysis is flagged on the result print out.
GEM Premier 7000 with iQM3 utilises patented technology for haemolysis detection, similar to that used in traditional laboratory analysers. Based on a photometric measurement of whole blood, the haemolysis module includes acoustofluidic flow cell integrated into the sample fluidic pathway for simultaneous measurement of all measured analytes and haemolysis detection.
Plasma is separated locally within the haemolysis module on a small portion of the sample without requirement for additional sample volume.
The optical detector and LED light source are implemented to illuminate the optical flow cell for absorbance calculation at each wavelength. By using photometric measurement of plasma-free haemoglobin, the level of haemolysis in the sample is then determined.
How is whole blood haemolysis detection possible?
- iQM3 ensures sample quality across the most common pre-analytical errors, and detects haemolysis in 45 seconds.11
- Haemolysis indices are configurable to fit with the institutional laboratory current protocols
- iQM3 detects errors faster than traditional (auto or manual) QC – in seconds vs hours12
- Performs continuous checks before, during and after every sample analysis. Traditional QC methods can miss sample-specific transient errors, including haemolysis, micro-clots, micro-bubbles, and benzalkonium, potentially impacting sample integrity
- Provides immediate and automatic corrective actions
- The all-in-one GEM PAK cartridge automates labour- and skill-intensive processes
The iQM3 assures quality of results, expediting critical patient management decisions with quality-assured results. It detects errors faster than traditional (auto or manual) QC in seconds versus hours. If haemolysis is detected, it will be flagged on the results screen and on the printout and on the electronic patient record or HIS/LIS.
The iQM3 ensures confidence in potassium results, enabling faster decision-making and, subsequently, better patient care.
What this means for patients
By looking to improve accuracy in collection of blood samples and by using new POC equipment that detects haemolysis, critical decisions that affect patient care can be expedited. The neonate can be managed quickly and safely in the knowledge that quality-assured results are being provided. The need for repeated samples should be reduced, so that the infant’s discomfort from repeated heel pricks may be minimised. The time that the clinician needs to dedicate to blood sampling from a single patient may also be reduced, allowing for their effective use of time.
