

Are we on the right pathway to manage babies born at 22 weeks’ gestation?
Locum Neonatal Consultant, MMUH Birmingham, Sandwell and West Birmingham NHS Trust
ahmed.yousef3@nhs.net
I would like to put forward the question of whether it is appropriate for neonatal teams to follow a risk-based approach in decision-making to actively resuscitate extremely preterm babies as per the 2019 framework published by the British Association of Perinatal Medicine (BAPM),1 or whether there is an alternative. Currently, BAPM is revising the framework to reflect present data, but it remains interesting to reflect upon how neonatal units are currently managing their extreme premature deliveries.
In questioning how resuscitation of extreme premature infants should ideally be managed to achieve optimal outcomes, we must consider how neonatal teams defer to management strategies for the tiniest babies and suggest how we could develop new strategies in resuscitation management and attempt to improve their outcomes, to reduce mortality and morbidity.
Identifying risk factors
Risk factors focus on congenital anomalies and their severity, the short and long-term outcomes and the consequential impact on parents and their community. Parental counselling is extremely important to ensure that parents are aware of the risks of birthing such an extremely premature infant. They need to be aware of potential distressing outcomes. At the same time, staff can still respect their wishes, and the agreed approach might be the cornerstone of the resuscitation management plan.
Necessary questions to ask
Is the NHS ready to accommodate decreasing the viable gestation age to 22 weeks? It should be questioned whether there are enough level three NICU cots to receive the increasing numbers of 22-week-old babies either in utero or post delivery, transferred from either level one or level two neonatal units. The question to the level three units will be: Are you ready to receive 22-week-old newborns? Do you have the staffing to manage potential one-to-one infants?
It is helpful to know whether the mother has received steroids (identified risk factor1). This risk factor can be addressed by following or developing a new strategy of giving steroids earlier to mothers who are at high risk of delivering at around 22 weeks’ gestation.
Optimising outcomes
If ideal outcomes are to be anticipated, the clinical treatment of infants born at 22 weeks’ gestation needs to be well planned and consistent. Publications from multiple international centres have shown that therapies should be neither random nor inconsistent, even though there may be variations in certain areas of care for this vulnerable population. It is important to consider their distinct anatomy, physiology and biochemistry when developing a standardised strategy.
Addressing risk factors for extreme premature births
It is important that we look to eliminate or reduce risk factors. Copying best practices such as those carried out in Japan, Sweden or the USA is a good option. We would concentrate on how to improve the service, resources and neonatal workforce that we currently have. We can develop new management strategies for respiratory support and nutrition and consider whether present treatment options are adequate.
The experience of a lone Japanese tertiary facility in caring for peri-viable newborns delivered as early as 2013 (2013-20) was described by Motojima et al.2 Overall, this cohort of 29 newborns showed promising results, with over 80% of them surviving. Remarkably, just two infants (11%) in this group had severe neurodevelopmental impairment and only one newborn (5%) in this group developed long-term cerebral palsy. Prenatal steroid use at comparable rates (34%), together with the prevalence of caesarean sections as the primary delivery route, are both linked to higher survival rates in this group.
The American College of Obstetricians and Gynaecologists has amended its guidelines to explore prenatal steroids for infants with gestational age of 22 weeks to 22 weeks and six days, given the overall better survival rates.3 The overall survival rates of infants at 22 weeks’ gestation in the United States are improving and there is currently a positive correlation between the use of antenatal corticosteroids and caesarean section delivery.4
A cross-sectional study also carried out in the USA looked at 137 NICUs between 2008 and 2021. Results indicated that a larger portion of resources in the USA was dedicated to caring for babies born at 22 weeks of gestation, which reflects changes in national clinical guidelines.5
A prospective study was carried out in Sweden to explore associations between perinatal activity and survival in infants born at 22 and 23 weeks’ gestation. It verified that Swedish neonatal units have adopted more proactive perinatal approaches for handling preterm births at 22-23 weeks’ gestation. Consequently, there was a fourfold rise in the survival rate of newborns delivered alive at 22 weeks over time, with no accompanying increase in significant neonatal health problems.6
The UK has not made significant progress in reducing the incidence of premature births yet. In 2020, preterm births made up 7.8% of all births, down from 8.3% in 2017. The UK’s preterm birth rate is higher than the European average of 6.9%. Based on data from 2010 to 2021, the neonatal mortality rate for babies born before 24 weeks’ gestation in England was 844.87 per 1,000 live births. For babies born between 24 and 27 weeks, the neonatal mortality rate is significantly lower, at 219.71 per 1,000 live birth and it continues to decrease with increasing gestational age.7
In Japan, the results of a survey conducted in infants at 22 to 23 weeks’ gestation indicated favourable survival rates and effective resuscitation efforts for live-born infants. The survival rates for infants born at 22 and 23 weeks’ gestation who were discharged from the NICU were 54% and 78% respectively among all live births, and 63% and 80% among those who received resuscitation at birth. Japan has implemented various innovative clinical management strategies, despite the lack of robust supporting evidence8 (TABLE 1).
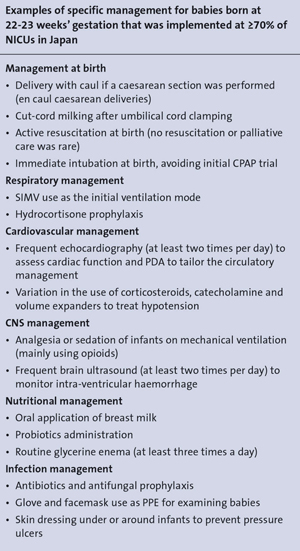
TABLE 1 Survival and unique clinical practices of extremely preterm infants born at 22-23 weeks’ gestation in Japan.
Thoughts to conclude
Having an increase in the number of extreme premature infants is a challenge to neonatal units and the NHS. I am hopeful that, with the use of evidence-based research and careful management plans for resuscitation, a real improvement in the outcome of 22-week gestation infants will be achieved.
Yours sincerely
Dr Ahmed Yousef, Locum Neonatal Consultant, MMUH Birmingham, Sandwell and West Birmingham NHS Trust
ahmed.yousef3@nhs.net
