

Implementing the national Maternity and Neonatal Safety Improvement Programme (MatNeoSIP) in North East and North Cumbria
The Maternity and Neonatal Safety Improvement Programme (MatNeoSIP), previously named the Maternal and Neonatal Health Safety Collaborative, is one of the priorities of the National Patient Safety Improvement Programme (NatPatSIP). These national priorities are identified to address the most important safety issues that are amenable to quality improvement. The MatNeoSIP national team drives forward and oversees the programme, which is delivered at a regional level by 15 Patient Safety Collaboratives (PSCs). All PSCs, which span the whole of England, have been involved in MatNeoSIP since its inception in 2017. Currently, funding for MatNeoSIP is through the Maternity and Neonatal Programme (MNP). A licence agreement, including an operating model and specification, forms the basis of an agreement between NHS England and Health Innovation Networks (previously called Academic Health Science Networks) for the delivery of the NatPatSIP priorities.
Julia WoodMaternity and Neonatal Safety Improvement Lead – Patient Safety Collaborative, Health Innovation North East and North Cumbria, julia.wood@healthinnovationnenc.org.uk
Sundeep Harigopal
Consultant in Neonatal Medicine, Newcastle Upon Tyne NHS Foundation Trust and Clinical Lead, Northern Neonatal Network
MatNeoSIP: aims, objectives, workstreams and measures
The overarching aims of MatNeoSIP have remained consistent for some time. However, as national priorities change, the MatNeoSIP objectives are aligned, which also means the workstreams and measures change too.
Aims
- Contribute to the national ambition set out in Better Births,1 to reduce the rates of maternal and neonatal deaths, stillbirths and brain injuries that occur during or soon after birth by 50% by 2025.
Contribute to the national ambition, set out in Safer Maternity Care,2 to reduce the national rate of preterm births from 8% to 6%.
Improve the safety and outcomes of maternal and neonatal care by reducing unwarranted variation and provide a high-quality healthcare experience for all women, babies and families across maternity and neonatal care settings in England.
Objectives for 2023/24
- To improve the optimisation and stabilisation of the preterm infant.
To improve the prevention, identification, escalation and response (PIER) to maternal and neonatal deterioration.
Objectives aligned to the Three-Year Delivery Plan for Maternity and Neonatal Services.3
Workstreams and measures for 2022/23 and 2023/24
The workstreams and subsequent measures have remained relatively consistent over the past two years.
Workstream: Optimisation and stabilisation of the preterm infant
Measures and rationale:
- Percentage of babies born in an appropriate care setting (place of birth) <27 weeks’ gestation or <800g, or all multiples <28 weeks’ gestation. An appropriate care setting improves survival and neurodevelopment outcomes.
Percentage of babies <30 weeks’ gestation that receive magnesium sulphate 24 hours prior to delivery. Magnesium sulphate reduces the risk of cerebral palsy.
Percentage of babies <34 weeks’ gestation that receive intrapartum antibiotic prophylaxis in established preterm labour. Intrapartum antibiotic prophylaxis reduces the risk of group B Streptococcus and sepsis.
Percentage of babies <34 weeks’ gestation that receive antenatal corticosteroids within one week of delivery. Antenatal corticosteroids reduce the risk of preterm lung disease, brain haemorrhage, necrotising enterocolitis (NEC) and sepsis.
Percentage of babies <34 weeks’ gestation that receive optimal cord management. Optimal cord management reduces the risk of brain haemorrhage as well as the need for blood transfusion.
Percentage of babies <34 weeks’ gestation that have an optimal normothermic range (between 36.5-37.5°C), which is measured within one hour of birth. An optimal temperature reduces the risk of mortality and brain haemorrhage, NEC and sepsis.
Percentage of babies <34 weeks’ gestation that receive maternal breast milk within 24 hours of birth. Maternal breast milk reduces the risk of sepsis and NEC.
In addition, in 2023/24, PSCs were asked to investigate the administration of caffeine and volume targeted ventilation (VTV). Caffeine prevents apnoea and facilitates extubating. VTV reduces the risk of lung injury and bronchopulmonary dysplasia in preterm babies.
Workstream: Early recognition and management of deterioration of women and babies
Measures and rationale:
- Ensure the use of the national Maternity Early Warning Score (MEWS) is embedded within an effective PIER pathway for managing deterioration. Although MEWS are widely used, they have often been locally developed resulting in considerable variation in charts for vital signs and also the range and number of parameters between what would be normal and abnormal. The development of a standardised national MEWS, adopted by all, will reduce this variation.
- Ensure the use of Neonatal Early Warning Trigger and Track (NEWTT2) is embedded within an effective PIER pathway for managing deterioration. NEWTT2 succeeds NEWTT and was developed to align to current recommendations for newborn care.
The national improvement approach
Outlined in the 2023/24 specification were the following refreshed set of improvement principles:
- Shift the overall patient safety approach from bureaucratic to proactive and generative.
- Learn from what works, and learn from and with organisations that are making it work.
- Provide more improvement support for those struggling, employing different strategies to help shape solutions.
- Understand the scale of problems alongside the improvement potential, acknowledging that some areas may require further research.
- Move from an obsession with individual problems to an obsession with system problems.
- Utilise networking and collaboration to help provide a focus on major safety challenges.
- Support systems to demonstrate ‘marginal gains’ in the absence of ‘silver bullets’.
- Co-design improvement approaches with outcome-focused ambitions.
- Utilise a robust prioritisation process for national issues.
An overview of NENC
North East and North Cumbria (NENC) covers a large geographical area of rural and city communities. Overall public health is among the worst in the country, with high levels of unemployment, low levels of adequate housing and significant areas of deprivation. These contribute to some of the starkest health inequalities, early death rates and the highest levels of ill health in England. NENC has the highest prevalence of maternal risk factors that subsequently contribute to poorer outcomes.
NENC has 10 maternity and neonatal units, spanning eight NHS Trusts. Three of these are neonatal intensive care units, with the remainder being special care baby units. The number of births in 2022/23 was 28,040 and of those, 648 were born at <34 weeks’ gestation. Currently, all trusts in NENC have developed their own MEWS charts and all use the original NEWTT.
NENC MatNeoSIP
A MatNeoSIP leadership team was established in 2017 and continues to meet regularly. Membership includes the NENC MatNeoSIP Lead, the NENC Patient Safety Lead, the NENC Clinical Leads and network managers from the Northern Neonatal Network, the NENC Maternity Network and the NENC Local Maternity and Neonatal System (LMNS). The leadership team steers the direction of the workstreams in NENC and ensure that work is joined up across the system.
NENC builds on the national improvement approach by utilising a range of improvement science methodologies that are underpinned by the Framework for High Reliability Healthcare (FIGURE 1).4 These include, but are not limited to: aim setting, process mapping, driver diagrams, a robust data strategy, the Model for Improvement, plus sustainability and spread approaches. The British Association of Perinatal Medicine (BAPM) quality improvement toolkits5-8 have been utilised to support this work.

FIGURE 1 The Framework for High Reliability Healthcare.4
As previously mentioned, the MatNeoSIP aims and objectives link to other national priorities, including Better Births,1 Safer Maternity Care2 and the Three-Year Delivery Plan for Maternity and Neonatal Services.3 Because of this, NENC MatNeoSIP has adopted a system-wide approach, tapping into existing system level entities and their existing infrastructures, including the Northern Neonatal Network, NENC LMNS, Maternity Clinical Network NENC, and NENC Integrated Care System (ICS), plus the eight trusts and 10 units that deliver maternity and neonatal services. This collaborative approach maximises capacity and impact, and reduces duplication. Also, where appropriate, NENC combines efforts with Health Innovation Yorkshire and Humber (Y&H) to deliver specific pieces of work.
Numerous topic-specific events are held, with attendance regularly reaching 60 delegates or over. These events have provided NENC stakeholders with the opportunity to hear from national and regional experts and also to share and learn from each other.
The MatNeoSIP Lead attends meetings and conferences and takes every opportunity to share information about the programme. Quarterly newsletters are also produced and there is a NENC MatNeoSIP hub on FutureNHS (www.england.nhs.uk/futurenhs-platform), where information relating to the workstreams is hosted.
Where measures require additional focus, the NENC MatNeoSIP has responded by hosting events and providing trust-level quality improvement support. During 2023/24 there has been an enhanced focus on place of birth, intrapartum antibiotics, optimal cord management and optimal temperature.
In addition, the MatNeoSIP Lead for NENC receives regular support from the National MatNeoSIP Team. Time is allocated for all MatNeoSIP regional leads to come together to learn from each other and share progress, plus 1:1 support is provided. This ensures that NENC keeps on track with the programme.
Impact
Workstream: Optimisation and stabilisation of the preterm infant
FIGURE 2 shows the progress made across NENC and demonstrates the following:
- In recent months, improvements have been made in place of birth, intrapartum antibiotics, optimal cord management and optimal temperature – the areas where additional focus has been given.
- The administration of magnesium sulphate is stable. In previous years a considerable amount of work took place regarding this as part of the PReCePT programme,9 and the improvements made have been sustained.
- The administration of antenatal steroids is stable, albeit poorly administered, and further work is required.
- The maternal breast milk measure has shown some positive improvements but has unfortunately recently returned to previous levels, demonstrating the need for robust sustainability approaches to be put in place.
The national requirement during 2023/24 to understand the baseline regarding caffeine and VTV has been completed.
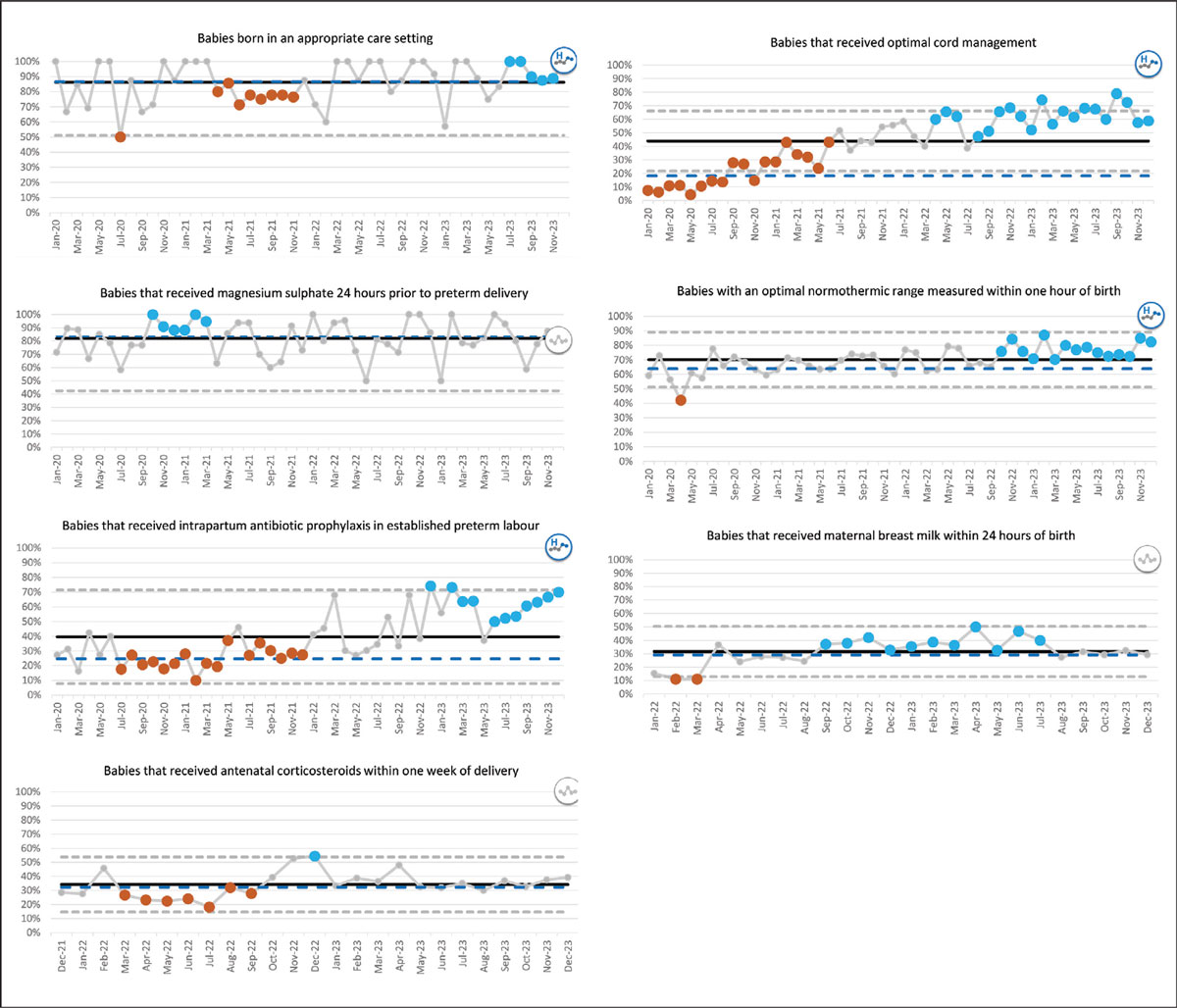
FIGURE 2 The progress made across NENC. Note: data are pulled from Neonatal BadgerNET and shared using statistical process control charts (SPC). Orange demonstrates a negative statistical change and blue a positive statistical change. In some cases, data collection began at different times and so some start points vary, but the majority of the baselines were between January 2020 and March 2021.
Workstream: Early recognition and management of deterioration of women and babies
Across the country, rollout of MEWS and NEWTT2 is happening in paper-based units. The national digital specification is in development and, because of the digital configuration across NENC, rollout has yet to start. However, in preparation for this, NENC and Y&H have run a series of events regarding the Royal College of Obstetricians and Gynaecologists Escalation Toolkit10 and the Birmingham Symptom Specific Obstetric Triage System.11 Also, considerable communications have happened in preparation for the rollout to begin.
Next steps
It is anticipated that the commission from NHS England for 2024/25 will continue to focus on the two workstreams that have been outlined here. There is still work to do regarding a number of the preterm birth measures and NENC is planning to have an enhanced focus over the coming months on antenatal steroids, maternal breast milk, caffeine and VTV. NENC will also continue to prepare for the digital rollout of MEWS and NEWTT2.
Learning points
- Maternity and neonatal units are under huge pressure and scrutiny at present and therefore focusing on national and system priorities helps support engagement and buy-in.
- A collaborative approach benefits all in terms of learning and sharing from each other, plus being able to pool resources and reduce duplication.
- Sharing data at both a system-wide and trust level, and understanding the reasons for changes in the data, ensures that time and resources are targeted appropriately.
- Using tried and tested improvement methodologies supports both implementation and sustainability.
Or read this article in our
Tablet/iPad edition
