

Preterm weaning guidance in the UK: background to the updated Bliss parent information
The weaning process, also known as introduction of complementary foods, is much more than just a change in the type of food a baby takes to obtain nutrition. It also has social, developmental, psychological, physical and medical connotations. Food and meals are the centre of many celebrations and often define cultural identity. Therefore, guiding parents to help their babies build a healthy and pleasurable relationship with food and eating is a key objective during weaning, and this can be aided by having comprehensive and unified guidelines. Such weaning publications have been provided by Bliss (a national independent parent support organisation) since 2002. The most recent update of the Bliss preterm weaning guidance features some adjusted recommendations;1 this article provides a summary of the history of Bliss weaning recommendations to date and provides an insight into the rationale for the adjusted recommendations.
Caroline King
Retired Neonatal Dietitian formerly of Imperial College Healthcare NHS Trust
Clinical Specialist Neonatal Dietitian, Royal Hospital for Children Glasgow
Annie Aloysius
Clinical Specialist Speech and Language Therapist (Neonatology), Imperial College Healthcare NHS Trust
Stephanie Tagani
Clinical Specialist Neonatal Dietitian, Imperial College NHS Healthcare Trust
Ailie Hodgson
Care Coordinator and Clinical Specialist Neonatal Occupational Therapist, South Tyneside and Sunderland NHS Trust
Rosie Hurlston
Clinical Specialist Neonatal Psychologist, Imperial College NHS Healthcare Trust
Charlotte Xanthidis
Clinical Specialist Neonatal Physiotherapist, The Royal Wolverhampton NHS Trust
Summary of changes between the 2017 and 2023 guidelines
The main changes between the 2017 and 2023 versions of Bliss guidance are summarised in TABLE 1 and discussed in the following sections.
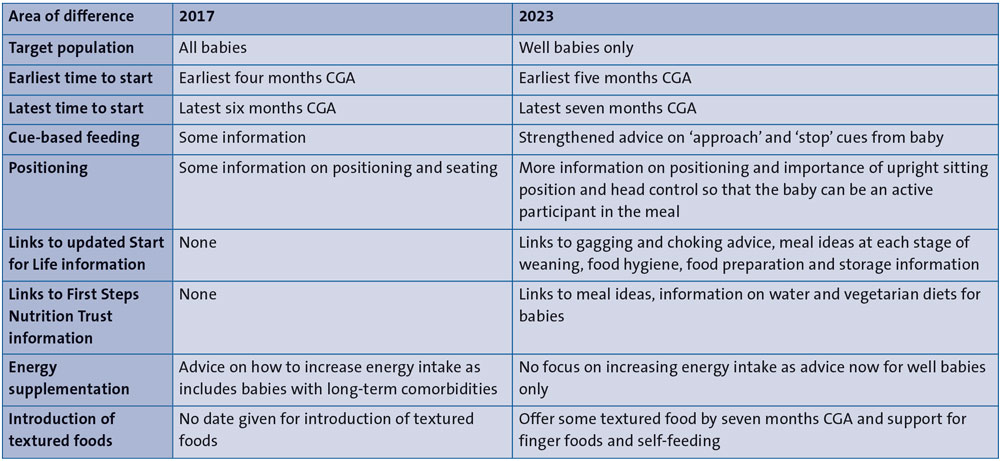
TABLE 1 Differences between 2017 and 2023 Bliss guidance. Key: CGA=corrected gestational age.
A focus on well preterm babies
For this update we acknowledge that a single piece of advice cannot serve the needs of all babies in a population, such as babies born preterm. Therefore, an important change in the current guidance is that it focusses on ‘well/healthy’ preterm babies. It is known that motor skills in preterm babies can lag behind term babies.2 The skills needed for weaning may be impacted further in those with long-term conditions and therefore these babies will need individual advice.3,4 Conditions such as cardiac, gastrointestinal (eg reflux disease), respiratory problems (eg bronchopulmonary dysplasia) and neurodevelopmental delay may all impact on progression through the weaning process.
Postural control can be delayed in preterm babies, with medical complications being the best predictors of this delay during the first year of life.5 Support for parents to manage these issues during weaning may involve a number of different health professionals, for example, an occupational therapist or physiotherapist to help with positioning. Babies with conditions impacting oro-motor function would benefit from the advice of a speech and language therapist in addition to dietetic input. Often support is best given by a multidisciplinary team (MDT), including those mentioned above and psychology support. Some babies may not be categorised as high risk for issues during weaning but may show them once weaning has started, for example oro-motor feeding problems.6 There is also useful information available for health professionals and parents considering adapted baby-led weaning in babies with developmental delay and other feeding challenges.7
Window for starting weaning
As can be seen in FIGURE 1, the window now suggested for weaning overlaps with the previous recommendations. A later window is recommended for starting weaning in the new guidance as it is considered more likely that babies will progress faster through tastes and textures as their skills will be more developed. They should also be closer to sitting unaided and more able to incorporate a baby-led weaning approach, with exploration of finger foods and self-feeding by the baby, alongside cue-based spoon feeding. Following the previous advice, babies would start weaning earlier but would be likely to be spoon fed purees for longer before they had the skills to move forward with textures and finger foods. Being spoon fed puree is not a required stage of weaning and does not aid in the development of important self-feeding skills.
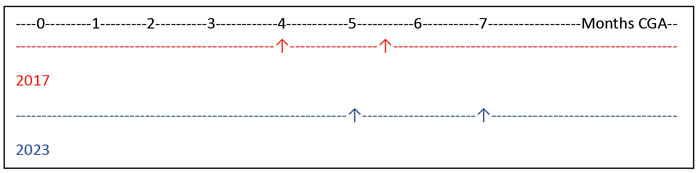
FIGURE 1 The window for weaning suggested in 2017 compared with 2023.
Strengthened advice on cue-based feeding
The widespread consensus on the importance of looking at developmental readiness for certain skills on neonatal units has influenced the approach and support babies now receive to manage their transition to suck feeding. Using a cue-based approach to weaning can be seen as a continuation of this responsive approach to feeding, now adopted by many neonatal units.
This new approach to suck feeding in neonatal units has led to improved outcomes such as decreased length of time to full oral feedings and hospital stay,8 while also increasing parents’ involvement in their babies feeding.9 The adoption of cue-based feeding early on gives parents more opportunity to get to know their babies’ behaviours, this knowledge can then be employed during the weaning process post-discharge. It moves away from scheduled feeds or fixed dates that a skill is expected and focuses on observing and responding to an individual baby’s developmental cues and abilities at the time they occur.
Improved positioning advice
The best position for weaning is one in which the baby can hold its head up easily, be supported to sit upright and be able to bring its hands together. There is also evidence that being able to sit or supported to sit, and therefore able to look round at its environment, helps the baby’s development in many other ways besides weaning.10
Visual attention and object manipulation are essential for cognitive development, these are both aided by sitting. There is some evidence that intake and processing of visual information is related to, and accelerated by, sitting.11,12 Earlier sitting has been associated with increased vocabulary size later on.13
Supporting a baby with hands-free sitting can allow them to reach for and manipulate food and other objects with greater ease, to interact with caregivers, and help them learn about mealtimes and eating by watching others.
Preterm babies often lag behind their term counterparts in sitting so we suggest that before they can sit independently but once they have developed good head control, they can be positioned on a parent's lap with appropriate trunk support.
This will enable them to watch mealtimes and others eating, explore food and, if they are showing appropriate cues, be offered some initial food tastes.
Links to national websites
Start for Life (www.nhs.uk/start-for-life/baby/weaning) and First Steps Nutrition Trust (www.firststepsnutrition.org/eating-well-in-the-first-year) are included in the updated Bliss guidance to provide valuable information on meal planning and to avoid repetition. They both have comprehensive, clear visual guidance on meal types and textures, as well as important practical advice.
Advice on energy enhancement
In previous guidance, advice was given on how to increase dietary energy intake in babies that might have increased energy requirements, for example those with a range of long-term co-morbidities. As the guidance is now for well babies only, such advice is no longer necessary. If a high energy diet is given to a well baby with no increased requirements, there is the risk that they will down regulate their intake and therefore take in a lower range of all nutrients.14,15
It is important to ensure that parents are supported to understand what constitutes an appropriate growth pattern for their baby, which may differ from their expectations. This can help to reduce anxiety around how much and what type of food their baby needs to eat to grow well. Failure to support parents can lead to early weaning, overriding a baby’s cues in an attempt to accelerate growth.16 However, babies with significant growth concerns should be referred to a dietitian for individualised support.
UK national preterm weaning guidance
Weaning babies born preterm is relatively neglected as a research topic, thus it is difficult to put together guidelines based on a wide body of evidence. Until around 20 years ago, different units across the UK devised their own weaning advice based on individual clinical experiences rather than published evidence.
In 1994, the UK government-based Committee on Medical Aspects of Food and Nutrition (COMA) published a report on weaning in the UK.17 It included a small section on weaning preterm babies based on factors thought to be relevant to this group, however, no published study was available to quote. It was suggested that weaning could commence when babies achieved the following: 5kg in weight, a diminished tongue thrust reflex and able to achieve lip seal around a spoon. It also advised a diet which was nutritionally adequate during the weaning process. The report hypothesised that compared to term babies, preterm babies experience accelerated maturation of some of their developmental pathways by the time they reach term. This would be due to their earlier more frequent exposure to various external stimuli. It was thought that many of these exposures would prepare them to wean at an earlier age than term babies.
No specific age for starting weaning was given. These recommendations lead to a wide variation in age at which a baby could be deemed ready. With respect to reaching 5kg, some of the smallest babies growing below the 0.4th centile would be over six months corrected gestational age (CGA), and some of the largest, only two months CGA.
In 2001 the UK Scientific Advisory Committee on Nutrition (SACN) discussed proposals around the optimal time for exclusive breastfeeding and, by default, the timing of commencement of weaning onto solids in term babies.18 The discussions highlighted that the considerations of low birthweight infants would need to be met under a different set of recommendations.
Thus, despite national expert group discussions on term weaning, the resulting guidance was sparse for preterm babies. This accentuated the need for detailed guidance based on neonatal practitioners’ experience and data extrapolated from studies of term babies.
International preterm weaning guidance
An Australian group recommended three months CGA.19 One Italian group suggested individualised advice based on a baby’s developmental abilities.20 In another Italian publication the advice was that a window between five and eight months uncorrected gestational age (UCGA) and at least three months CGA seemed appropriate.21 These groups based their suggestions on a review of the literature published in the UK in 2009.22
A European-wide group suggested a start point could be three months CGA, once a baby had gained sufficient head control, but advice should be adapted for individual babies.23
Inception of the Bliss weaning guidelines
Before the availability of the Bliss guidance, parents received contradictory advice from different sources including MDTs on neonatal units, health visitors, general practitioners, paediatricians, friends and other family members. In some cases, printed advice was funded by infant formula manufacturers, with the risk of commercial bias.
When the first randomised controlled trial (RCT) of preterm weaning was published,24,25 the need for unified guidelines was highlighted by researchers in the field.26 In discussion with the authors, it was agreed that it would be more appropriate to have such advice published by an independent organisation rather than an infant formula manufacturer, as was mooted at the time. The first weaning guide was co-produced in 2002 by the consensus of an expert professional group in partnership with Bliss. The guidance has been regularly updated over the last two decades with various changes in the composition of the expert group.
The evidence base for Bliss weaning guidelines
Editions 1-8 (2002 to 2012)
Despite the 1994 COMA guidance,17 preterm babies in the UK were frequently weaned before reaching 5kg, one study reporting that 20% were weaned before reaching this weight.26 They were also more likely to be weaned before four months CGA than term babies in the USA27 and in the UK.25,28-30 Practice in neonatal care and the conclusions of Marriott et al24,25 determined that weaning earlier than the available guidelines for term and preterm babies was more appropriate.
The study of Marriott et al assessed the growth and iron status in 68 babies who were randomised to an early intervention group advised to wean at 13 weeks UCGA.25 This translated to weaning at 6.3 weeks CGA, compared to 9.9 weeks CGA in the control group. The early group were advised on solids with enhanced nutritional value and given preterm formula to mix in food where liquid was needed. This resulted in improved length measurements but not head circumference or weight. Iron status was significantly better in the early group at six months CGA.
An article published in 2009 gave a more extensive rational for the original Bliss guidance drawing on many observational studies in preterm and term babies.22 In summary, it suggested that babies born at <34 weeks’ gestation could be weaned between five and eight months UCGA, but that they should at least have reached three months CGA to allow sufficient head control. The actual start time of weaning, within the three-month window, would depend on individual babies’ cues. It was felt that babies born ≥34 weeks’ gestation could be weaned along the same guidelines as term babies.
This early Bliss advice was based on the same premise as the COMA report17 – development in many spheres important for weaning could be accelerated with earlier exposure to relevant stimuli – and gave a window of ages these skills would potentially emerge. There was a caveat that very few babies would be weaning at the earliest or at the latest ages recommended.
There is evidence for accelerated maturation of many aspects of gastrointestinal function with early milk feeding leading to early appearance of some digestive enzymes, improved motor activity and promoting small intestinal growth,22 all of which would lead to a preterm baby having better digestive capacity by term age, compared to a baby born at term and enable digestion of a weaning diet by three months CGA.
Renal function is also accelerated, triggered by the contraction of extracellular water that occurs postnatally.31 One study found normal serum biochemistry in preterm babies weaned from two weeks CGA.28 This precocious renal maturation suggests adequate preparation for weaning by three months CGA.
One of the concerns about weaning preterm babies as early as three months CGA was that it would put them at increased risk of allergy. However, evidence does not support this belief.22 A paper looking at timing of weaning in preterm babies did not find a relationship to atopy.29
Advice to wait until three months CGA gave time for progression with some motor skills, such as adequate head control ready for weaning.23 However, it was recognised that some other key developmental abilities are not accelerated by early exposure to extrauterine life. Motor development matures according to post-conceptional rather than postnatal age, and both fine and gross motor development, including sitting, can be delayed by preterm birth.4 In one study, 50% of preterm babies sat unsupported at around seven months CGA compared with the term group where 50% were sitting at around six months.32 Head control and trunk stability provide the necessary gross motor skills for fine motor control of hands and mouth during weaning.23
Baby-led weaning was suggested for term babies where they are presented with pieces of food to pick up and feed themselves. This can only be done from a sitting position and with sufficient motor development. This may be challenging for some preterm babies who are not yet sitting; therefore, this approach was not promoted in the earlier editions.
There is a concept of a critical period during which babies would be developmentally ready to make the transition from an all-milk diet to solid food with more texture, and a concern that not starting weaning during this time could result in feeding difficulties. This has been illustrated by reports of babies kept nil-by-mouth or on pureed food during the first year of life, who then have great difficulty in learning to manage textured food. Thus, demonstrating a sensitive period for texture acceptance but failing to pinpoint exactly when this is.33 In term babies, there is some suggestion that a delay in having textured food until after 9-10 months is associated with eating fewer family foods and being more difficult to feed than those given textures before 9-10 months,34 with the association persisting until seven years of age.35 The Bliss guidance recommended that some textured food should be offered by around nine months UCGA to allow for a gradual increase in managing textured food according to each baby’s ability.
In later editions, emphasis was put on increasing variety in the diet to improve later food acceptance and finger foods to help babies manage more texture. Enabling babies to explore food by touching, smelling and tasting as soon as they show an interest, can help the development of self-feeding skills using hands and fingers. More textured foods may be better accepted as finger foods as the child can hold them and bring them to their mouth when they are ready.
Term babies accept a wider range of flavours later on if they are introduced to a wide range earlier in the weaning process, eg at around 4-5 months old.36 Also in term babies, 4-7 months old, giving repeat exposure to a food will increase acceptance in the majority of cases.37-39 Offering a food every day for 10 days or alternate days for two weeks, appears to be a helpful approach.
In preschool children, food acceptance is enhanced with the inclusion of the child in larger groups at meal times.40 This gives them opportunity to watch, learn about and imitate feeding. Strong family similarities have been noted in preferred foods,41 and intake of general food groups in toddlerhood could be predicted by their frequency of consumption during infancy.42
As well as advice to follow the babies’ cues of weaning readiness, the guidance included information on how to recognise satiety cues and when babies want to stop eating so that any form of pressure to eat more or forced feeding is avoided. It was advised that feeding is stopped if the baby shows any sign of refusal, such as keeping their mouth closed, turning away, actively spitting food out or becoming distressed when food is offered.
Editions 9 and 10 (2017 and 2023)
Both the 9th and 10th editions use CGA rather than UCGA, and a later age window within which to consider weaning. Using CGA further acknowledges the motor changes important for weaning, which occur according to a developmental clock.
In 2017, an RCT of preterm weaning in a lower middle-income country was published.43 Babies born at <34 weeks’ gestation (n=403) were randomised to weaning at four versus six months CGA. The primary outcome was weight at 12 months CGA, which did not differ between the two groups. No difference in secondary outcomes were seen, including neurodevelopment, body composition, bone mineral content and density, insulin resistance, lipid profile, blood pressure and serum ferritin. Breastfeeding rates between groups were similar and both groups had good compliance with commencement of weaning at the time advised by the researchers. Babies assigned to the early weaning group had more hospital admissions than those in the late group. The authors noted that the breastfed babies in the late weaning group appeared to increase their milk intake compared to those in the early weaning group. Therefore, they speculated that the increased hospital admissions could be due to a lower intake of breast milk in the early group, rather than potential contamination of weaning foods. Although not suitable to apply fully to a higher income country, it demonstrated that weaning at six months was not detrimental in the context of this study.
In 2018 an observational study based in Scotland looked at oral feeding outcomes associated with weaning at 4-6 months CGA.44 Babies had been inpatients on a neonatal unit that employed a developmentally supportive care approach in the management of preterm infants, which included weaning based on developmental readiness and corrected age. The babies were monitored up to 12 months CGA and there were no reported problems with progression through textures, feeding related problems or aversions. This further supported the adoption of a later weaning window for the Bliss guidance.
A more recent RCT looked at two time points for weaning. Babies (n=177) were randomised to weaning at 10-12 or 16-18 weeks CGA.45 There was no difference between the groups in primary outcome, which was length at one year CGA, neither was there any difference in any of the other anthropometric measurements. The authors concluded that preterm babies should be started on solids according to neurological abilities rather than nutritional intake and growth, and they felt 10-12 weeks CGA was too early.
These three studies support the move to recommend a later window for weaning. The emphasis remains that this is a window and that the earliest time to consider weaning is not signalling the time to start. The numbers weaning at the earliest and latest times would be very small with the majority of babies weaning around the middle of the window and following the pattern of a bell-shaped curve (FIGURE 2). Unfortunately, the earliest date is often taken as the time to start, as illustrated in Marriott et al 2003,25 where parents in the control group were advised to choose when they thought their baby was ready as long as it was after 17 weeks UCGA. In fact, most chose a time very close to 17 weeks; the mean age of starting was 17.8 weeks UCGA.
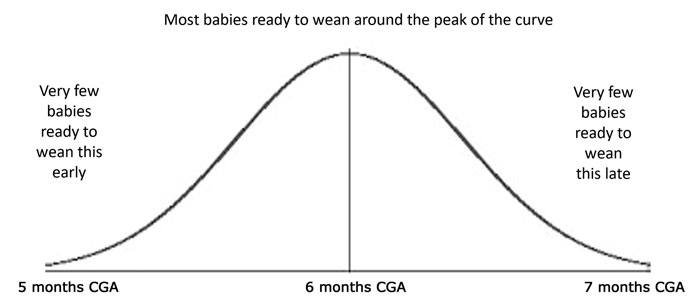
FIGURE 2 Bell-shaped curve indicating numbers of babies likely to be ready for weaning within the suggested window of 5-7 months CGA.
Summary
After intensive monitoring and involvement from specialist health professionals on the neonatal unit, parents can feel uncertain about aspects of caring for their baby post-discharge. It is hoped that the Bliss guidance will continue to provide a useful source of information for parents and community health professionals during the weaning period. The updated Bliss guidance has expanded the information for parents to be able to navigate the weaning process more easily. With more parental involvement on neonatal units, parents are becoming experts in their own baby’s care earlier. With this knowledge, it is hoped parents can have the confidence to make the best decisions about weaning their baby – following their own individual baby’s developmental path. A guiding principle in the current recommendations is that the baby leads the process and is a more active participant than in previous guidelines.
Disclaimer
No funding from any source was received by the authors for writing this article.
Acknowledgements
The authors extend thanks to: Connor Lane (former Senior Information and Content Officer, Bliss); Madinah Thompson (Senior Information and Content Officer, Bliss); the Bliss parents’ group, which reviewed the drafts of the new weaning guidance; specialist neonatal therapists from dietetics, speech and language, physiotherapy, occupational therapy and psychology, and Gill Rapley, writer and lecturer in baby-led weaning and parenting.
Or read this article in our
Tablet/iPad edition
