

The National Neonatal Audit Programme: improving standards of care and driving quality improvement
Since 2006, the National Neonatal Audit Programme (NNAP) has assessed whether neonatal unit babies receive consistent, high-quality treatment. The summary report on 2022 data showed that variations persist in the rates of key outcomes of neonatal care. These variations are seen between units and networks.
Rachel Winch
NNAP Project Manager, Royal College of Paediatrics and Child Health
nnap@rcpch.ac.uk
Sam Oddie
NNAP Clinical Lead, Consultant
Neonatologist, Bradford Teaching Hospitals NHS FT
The NNAP1 is commissioned by the Healthcare Quality Improvement Partnership (HQIP) and delivered by the Royal College of Paediatrics and Child Health (RCPCH). The summary report on 2022 data was published in October 2023 (FIGURE 1).2 The report summarises the key messages and national recommendations developed by consensus by the NNAP Project Board and Methodology and Dataset Group, based on NNAP data relating broadly to babies discharged from neonatal care in England and Wales between January and December 2022, and Scotland between 1 April 2022 and 31 December 2022.
FIGURE 1 The NNAP summary report on 2022 data, published in October 2023.
Outcomes of neonatal care
Variation persists in rates of key outcomes of neonatal care, ie mortality, bronchopulmonary dysplasia (BPD), necrotising enterocolitis (NEC) and bloodstream infection. This variation is not new but is a matter of concern. This variation is seen between units and between networks and is seen even when measured background characteristics are accounted for. For example, rates of mortality in very preterm infants range from 4.8-8% between neonatal networks. Furthermore, the overall rate of BPD or death is rising in very preterm infants (2015-2017=36.3%; 2020-2022=39.7%, p< 0.001), rather than the desired decrease over time. There is a need and an opportunity to deliver significantly improved outcomes for babies if the poorest performing networks across each measure improved to the level of the best performing networks.
The NNAP measurement of preterm brain injury is confounded by high rates of missing data. For example, the overall figure for missing data for intraventricular haemorrhage is 13.9%, but this varies by operational delivery network from 1.9% to 57.4%. There has been some improvement in the proportion of NNAP neonatal unit clinical leads who were able to assure their NNAP data on preterm brain injury (2022=71.8%; 2021=66.3%). Describing this critical outcome of neonatal care must be a priority for neonatal units and networks to facilitate quality improvement (QI) and assurance and also to allow measurement against the national ambition to reduce rates of brain injury during, or soon after, birth.
Optimal perinatal care
Deferred cord clamping (DCC) rates continue to rise. Considering only very preterm infants, 55.4% had DCC in 2022 compared to 43% in 2021. The neonatal community should be proud of its practice change in this regard. Neonatal network managers should support those units where further improvement in DCC is required. On average, significantly higher rates of DCC are achievable, without needing to try the as yet unproven technique of ‘cord intact stabilisation’.
Adherence to timely administration of a full course of antenatal steroids is highly variable, ranging from 45.9% to 58.5% across neonatal networks. Overall, 52% of mothers who delivered a baby between 23 and 33 weeks gestational age received a full course of antenatal steroids within one week prior to delivery. This reflects the challenge of delivering antenatal steroids in a timely fashion to maximise clinical benefit. It is also possible that use of a 12-hour interval between doses of betamethasone, even though this has not been found to be beneficial, might confound some of this measurement. The NNAP team is concerned about the lack of concurrent description through maternity data of the number of women treated with antenatal steroids, some of whom will not deliver preterm.
In 2022, 76.3% of babies had a temperature within the normal range that was measured on time. There has been a sustained year-on-year improvement in the proportion of babies admitted with a normal temperature, from 58.1% in 2015. There has been no associated significant increase in the proportion of babies admitted with hyperthermia.
Parental partnership in care
Breast milk feeding of preterm babies at discharge is not improving in the UK. In 2022, the proportion of babies receiving breast milk feeding at discharge home ranged from 48.6% to 79.3% between neonatal networks. For the first time in 2022, the NNAP also reports the proportion of babies receiving breast milk within the first two days of life; this ranges from 34% to 76.7% between neonatal networks. Improving rates of initiation of breast milk feeding may maximise the early benefits of breast milk and increase the chances of establishing longer term breast milk feeding. FIGURE 2 indicates the rates of breast milk feeding at two and 14 days of life and at discharge home.
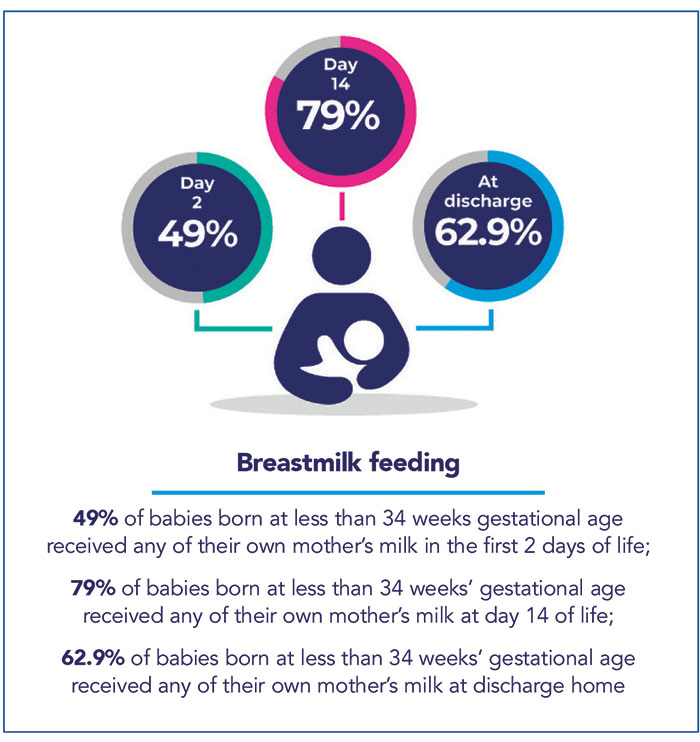
FIGURE 2 Breast milk feeding rates.
There is wide variation between neonatal units and between networks in the proportion of consultant ward rounds with parental involvement. Parents were included in ward rounds on 47.2% of care days, ranging from 36.8% to 60.3% between neonatal networks. A ward round is recorded as not taking place on 10% of baby care days, and data were missing for 23.2% of baby care days.
The proportion of neonatal admissions where a consultation with parents took place within 24 hours of admission has remained static over the past five years, with parents having a consultation with a senior member of the team for 95.9% of admissions in 2022.
Nurse staffing levels
The proportion of neonatal nurse shifts staffed according to recommended levels in 2022 across England, Wales and Scotland is 71.1% (FIGURE 3), having fallen for a second year in a row (2021=73.9%; 2020=78.6%, England and Wales only). The continuing decline in neonatal nurse staffing levels is a matter of serious concern to those providing and commissioning neonatal services, given its association with increased mortality.
FIGURE 3 The proportion of neonatal nurse shifts staffed according to recommended levels.
Care processes
The NNAP introduced a new measure for 2022 in order to identify any variation in the exclusive use of non-invasive breathing support, which is recommended by the National Institute for Health and Care Excellence (NICE) for support of the least mature infants. The proportion of babies in neonatal intensive care units receiving only non-invasive breathing support in the first seven days varies from 16.5% to 71.4%; analysis shows this variation is unexplained by gestational age mix.
For the first time, the NNAP reports adherence to the updated UK screening for retinopathy of prematurity (ROP) guideline,3 published in March 2022. Overall, 69% of eligible babies were screened appropriately according to the new guideline. This proportion should not be compared to previous results that reported against the previous ROP guideline and so do not offer a fair comparison. The variation between neonatal networks in on-time screening is wide (49.8% to 77.3%) and concerning, as it was under the previous guideline.
NNAP national recommendations
TABLE 1 gives a summary of the main report recommendations. Full national recommendations and actions for local QI can be found in the summary report.2 The report webpage includes a range of other resources such as the extended analysis and recommendations table.
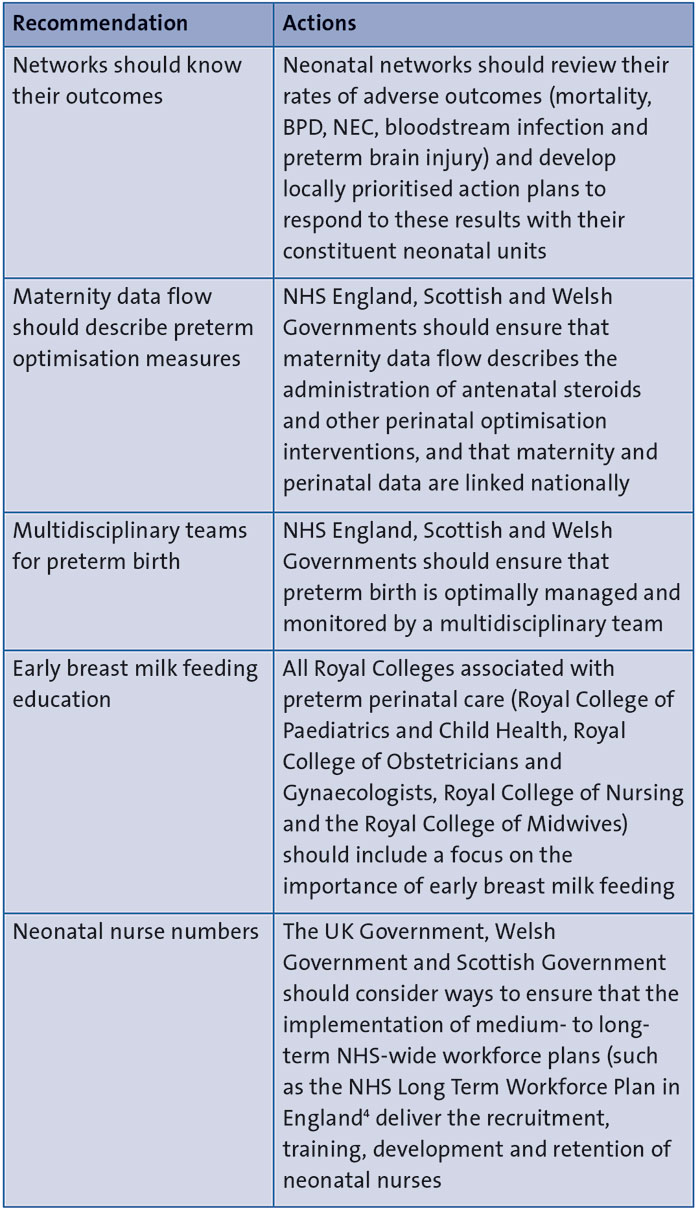
TABLE 1 A summary of the main report recommendations.
NNAP resources
The NNAP produces a wide range of resources to enable you to review your local results alongside the recommended actions for local QI to help you formulate priorities and action plans. Details of these resources can be found in Table 2.
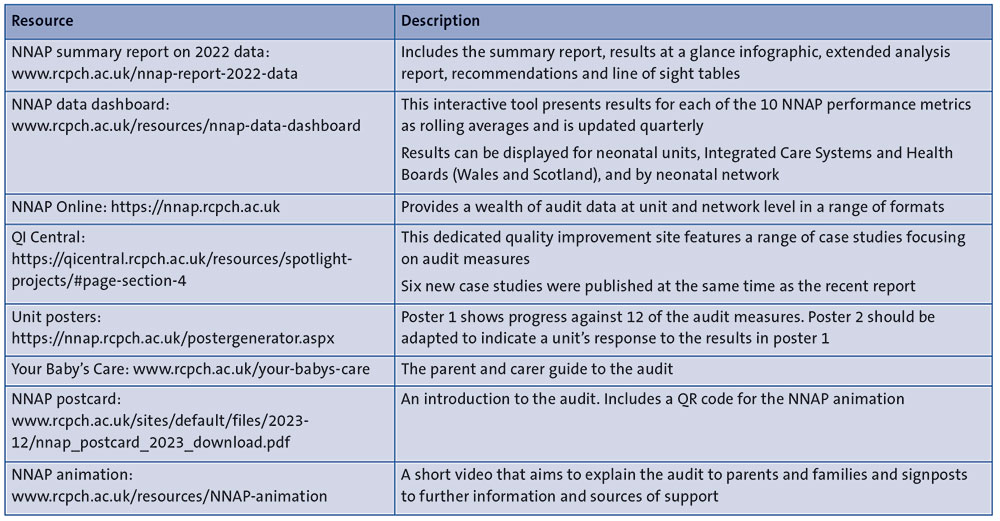
TABLE 2 NNAP resources.
Unit posters, Your Baby’s Care and the NNAP postcard were sent out to all clinical leads at participating units towards the end of last year. We encourage neonatal teams to consider the best ways to share these resources with parents and families using their service, to make sure they are aware of the NNAP, why it is important and how their baby’s information is used.
What next for the NNAP?
Reviewing and validating your data
Early in 2024 we will be issuing final data quality and completeness reports to units and networks giving them the opportunity to conduct a final review of their 2023 data. We will also be writing to clinical leads to ask for assurance that all their bloodstream infection, NEC and preterm brain injury data are complete and accurate. To support this process the NNAP held a webinar on data completeness on 10 January 2024. To access the recording please follow the link from the NNAP homepage.1
Frequent reporting of NNAP results
The NNAP launched its new data dashboard in summer 2023.5 The dashboard presents results for each of the 10 NNAP performance metrics as annual rolling averages and will be updated quarterly. Results can be displayed for neonatal units, Integrated Care Systems and Health Boards (Wales and Scotland), and by neonatal network. A restricted access section of the dashboard will be available early in 2024 where authorised users will be able to review unit level data.
Supporting services to reduce health inequalities
Throughout 2023, we asked services to improve completeness of their postcode and ethnicity data to support reporting of NNAP metrics by ethnicity and deprivation indices. In 2024, we intend to produce supplementary national level reporting for the first time, which will enable exploration of health inequalities in the delivery of neonatal care.
Or read this article in our
Tablet/iPad edition
