

NEO-TRAIN: an educational QI initiative to drive sustainable evidence-based change on a neonatal intensive care unit
Neonatal GRID Trainee
Corrina Proctor
Advanced Neonatal Nurse Practitioner
Nitesh Singh
Consultant Neonatologist
Sarah Louise Williamson
Consultant Neonatologist, sarahlouise.williamson@nhs.net
Neonatal Intensive Care Unit, University of Coventry and Warwickshire NHS Trust, Coventry, UK
McDermott H., Proctor C., Singh N., Williamson S.L. NEO-TRAIN: an educational QI initiative to drive sustainable evidence-based change on a neonatal intensive care unit. Infant 19(6): 219-21.
About the QI initiative
Quality improvement (QI) is an essential part of delivering high quality care on the neonatal unit. As new research and guidelines are introduced, it can be difficult to remain up-to-date and to introduce and adopt new ways of working into daily clinical practice. As we strive to provide the best possible care for our babies in line with current evidence, this is most effective when planned and delivered by an interprofessional team, to provide a combination of skills, knowledge, experience and credibility.1
QI methodology has been shown to facilitate, embed and streamline such evidence-based practices using changes ideas, systematic implementation and frequent snapshot measurements driving improvements. However, we found that this is not widely taught or embedded into the workplace. Therefore, introducing evidence-based changes can be challenging. Other barriers include frequent staff rotations, lack of resources and teams and individuals working in isolation without regularly sharing their learning.1
The NEO-TRAIN QI educational initiative was developed and introduced in September 2020, aiming to create a robust, structured, sustainable evidence-based programme to support change on the neonatal intensive care unit at University Hospital Coventry and Warwickshire (UHCW).
This was designed and led by a neonatal consultant with a higher degree and experience in QI, a senior neonatal grid trainee and an advanced nurse practitioner. The first step was to assemble interprofessional QI teams. This included a consultant and advanced neonatal nurse practitioner lead, a neonatal nurse and other members relevant to each project including nursery nurses, obstetric and midwifery representatives. Trainees were allocated to a group during placement to contribute to an ongoing project and be part of a longer-term change, despite usually only being in post for six months.
Each group focuses on a key area of neonatal care, chosen based on British Association of Perinatal Medicine (BAPM) recommendations, national neonatal audit programme (NNAP) data and local clinical need. Each team chooses a name and logo for their team and project, encouraging creativity and team bonding.
The second step was to provide regular training on QI methodology. This is now face-to-face educational meetings, scheduled twice a month as part of the departmental teaching programme. It includes interactive interprofessional educational sessions, time for groups to discuss planning, present change ideas and measures in their projects and receive constructive feedback. There is also a six-monthly department poster competition for groups to share their achievements.
This is supported by a step-by-step QI toolkit, adapted from the Institute for Healthcare Improvement QI essentials toolkit 2017,2,3 covering:
- Planning/designing a QI project: principles, SMART (specific, measurable, achievable, realistic, time frame) aims and how to create a process map, fishbone diagram, driver diagram and pareto chart.
- Measuring/monitoring: choosing clear and specific data points to monitor, creating run charts.
Simple, common examples of processes such as ‘making a cup of tea’ or ‘baking a cake’ are used in the toolkit (FIGURE 1) and a six-monthly delivery of face-to-face teaching by the QI programme lead, to illustrate the ways in which these methods can be utilised.
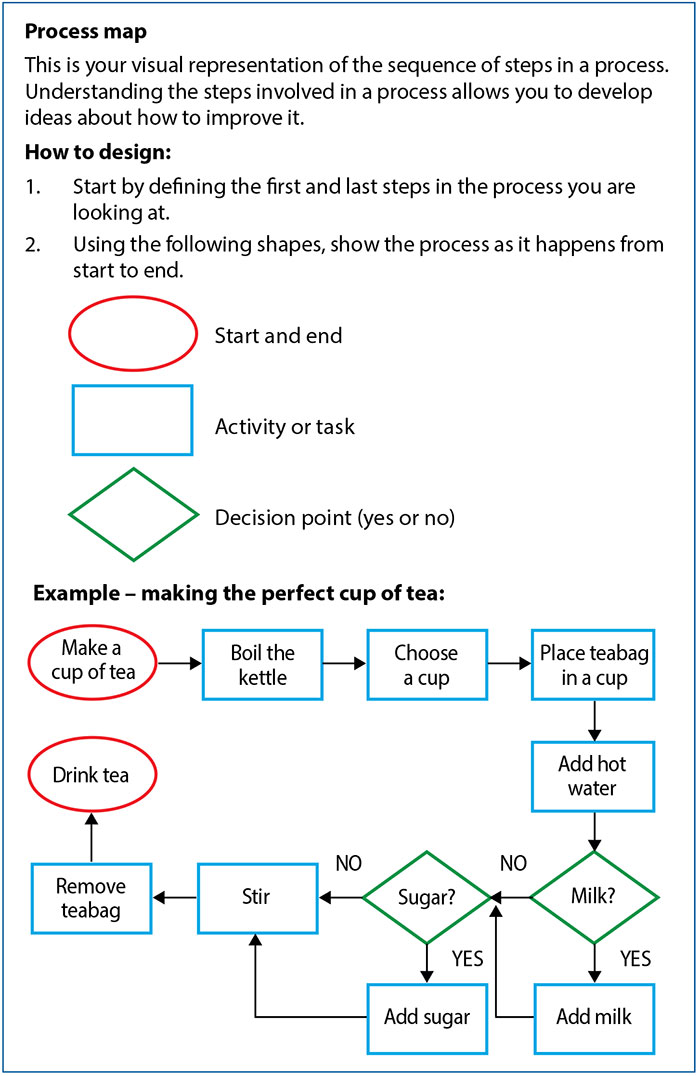
FIGURE 1 Simple, common examples of processes such as making a cup of tea or baking a cake are used in the UHCW neonatal department QI toolkit. These visual representations help with understanding the steps involved in a process.
All groups use PDSA (plan, do, study, act) cycles to implement and test change ideas. Measures also include monitoring for any unintended consequences when changes are being implemented, so that these can be quickly identified and addressed to ensure ongoing patient safety.
Prospective data are displayed using visual boards and discussed at daily huddles, disseminated through department WhatsApp groups, bi-weekly ‘safety champion’ meetings with the perinatal team and presented at regional MatNeo (maternity and neonatal) safety meetings. Successes and challenges have been presented at the hospital trust briefings, grand rounds and at the quarterly neonatal network QI meetings. Increased awareness of QI work at trust and local level has led to increased buy-in from stakeholders.
QI groups
Between 2020-2023, there have been 10 groups, with six groups currently running (FIGURE 2). These have evolved, to ensure sustainable change. These include:
- The OptiClamp project (2022) focuses on improving optimal umbilical cord management (OCM) and thermoregulation at delivery. Our unit was identified as a negative outlier in 2021 NNAP data for OCM. Our OCM >1 minute has since improved from 38% to 75%. This evolved from the group ‘STAMPED’ (2020), which focused on the BAPM antenatal optimisation toolkit4 for improving antenatal steroid administration, magnesium sulphate and neonatal counselling for pregnant women presenting with preterm labour.
- The PEEP project (2021) aims to reduce bronchopulmonary dysplasia and initially focused on implementation of an early respiratory care bundle, which successfully reduced ventilator days and need for intubation of extreme preterm babies at delivery. This is now subdivided into PEEPon (early respiratory) and PEEPoff (late respiratory), standardising weaning from non-invasive ventilation using oxygen saturation histograms.5
- The XPRES project (2021) focused on early administration of buccal colostrum. This evolved to include the implementation of probiotics and donor human milk, demonstrating a 20% improvement in breast milk at discharge rates.
- Bug Busters (2021) focuses on infection. Subgroups are currently focussing on central line-associated bloodstream infection (CLABSI) rates, having already successfully introduced:
• a sepsis risk calculator6,7 to reduce antibiotic administration to term babies with risk factors for early onset neonatal infection
• administration of antibiotics within 60 minutes of decision to treat time,7 which has reached 100% and has been over 90% for many months.
- Midline Matters (2023) concentrates on developmental care, specifically positioning, midline positioning within the first 72 hours of life and management of painful procedures.8
- NeoBalance (2023) reviews fluid management in the first week of life, particularly in extreme preterm babies.
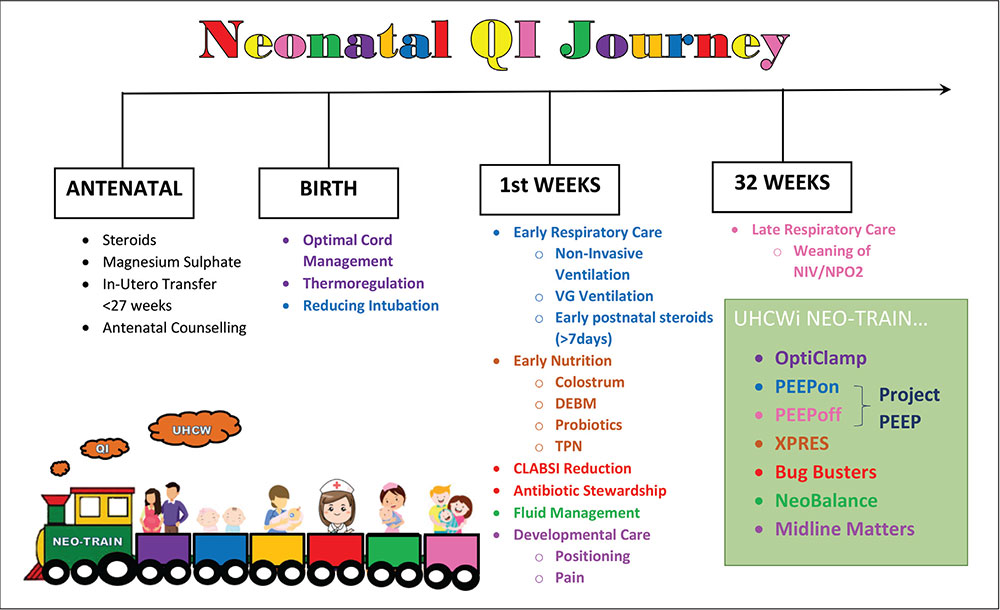
FIGURE 2 Between 2020-2023, there have been 10 QI groups at UHCW, with six groups currently running. Key: VG=volume guaranteed; DEBM=donor expressed breast milk; TPN=total parenteral nutrition; NIV/NPO2=non-invasive ventilation/nasal prong oxygen.
Supporting professional development
Team members have been supported and empowered to share their work at local, national and international forums. This has given them opportunities to learn how to write abstracts, create conference posters and deliver oral presentations, with all who have been involved in the project credited.
Challenges
Both time and resources are a continuous challenge in the NHS. We have found that evolving a successful group to allow a continuous focus on around six topics at once seems to be the most effective way of maintaining focus and engagement, without over-stretching resources. Any further ideas can be considered, supported, and implemented in future. Each unit will find themselves at a different junction in their QI journey and will need to pace it accordingly to maintain the ‘gain’ and sustain the improvements.9,10 It is also important that each team has a nominated lead. This helps maintain general oversight, team composition and task allocation. Having a variety of professionals in the team is beneficial, however, ‘too many’ members can be counterproductive.
Trainees in the department receive scheduled days they can dedicate to audit, admin, research or clinic if the clinical workload allows, as per the Royal College of Paediatrics and Child Health (RCPCH) trainee charter.11 This can be more challenging to achieve for nursing, midwifery and allied health professional team members.
Conclusion
We recommend this as a viable model for departments to embed QI, respond to changing clinical problems and drive sustainable change.
Our recommendations for units looking to embed QI:
- Assemble an interprofessional team and engage parents or parent groups locally or nationally, eg Bliss.
- See QI as an opportunity to learn, teach and embed changes.
- Plan projects using relevant QI toolkits.
- Review data regularly and as contemporaneously as possible (eg every two weeks, maximum monthly) so that any unintended consequences and/or barriers can be identified.
- Celebrate achievements and disseminate widely.
Or read this article in our
Tablet/iPad edition
