

Exploring the pre-hospital setting for the emergency care and transfer of neonates: the role of UK ambulance and neonatal transport services
Babies born before arrival (BBA) of a healthcare professional in the pre-hospital setting have a higher risk of morbidity and mortality than those born in the presence of professionals, both in low- and high-income countries.1,2 Furthermore, an increasing body of evidence shows that babies that are born extremely premature or with congenital abnormalities are more likely to survive if born in a hospital with access to tertiary neonatal intensive care services.3,4 Whether BBA or born outside of a tertiary unit, these babies will be attended to by the UK ambulance service or a commissioned neonatal transport service. As we look forward to the future of neonatal care, this special report aims to discuss the role the ambulance service plays in enhancing neonatal care provision. We highlight considerations for acute care providers, integrated care boards and neonatal networks in working cross sector to optimise care to this cohort of patients.
Stephanie Heys
Consultant Midwife, The Northwest Ambulance Service, Senior Research Leader, NIHR, stephanie.heys@nwas.nhs.uk
James Yates
Specialist Paramedic (Critical Care), Great Western Air Ambulance Charity
Camella Main
Lead Midwife, London Ambulance Service
Patrick Turton
Lead Nurse, Southwest Neonatal Advice and Retrieval (SoNAR)
Dawn Kerslake
Consultant Midwife, The South East Coast Ambulance Service
Background
In recent years the scale and development of neonatal operational delivery networks (NODNs) has strengthened joint working and collaborative system approaches to implement and evaluate the impact of national priorities for neonatal care.5 NODNs are focused on coordinating patient pathways between providers over a wide area to enable access to specialist resources and expertise, ensuring neonatal care provision and services are available. The networks allow clinicians across a range of specialties to share knowledge and skills to accelerate learning and support quality improvement across systems in this specialist branch of health care.
Neonatal networks also commission neonatal transport services, to ensure transfers of sick babies are led by specialist clinicians with appropriate equipment. However, a recent study highlighted the need to focus efforts on the burden of morbidity and mortality associated with preterm birth and ensuring babies are born in the right place at the right time.6
More recently, the pre-hospital setting has been a focus for local maternity and neonatal systems acknowledging the importance of providing optimum care for babies BBA. Despite an increase in awareness, there is a lack of recognition of the ambulance service as a key care provider of maternity and neonatal care in national reports, including the NHS three-year delivery plan.7 A truly collaborative approach to optimising care for families and service delivery of the immediate and essential actions detailed within the recent Ockenden Report, requires inclusion of ambulance trusts that also provide maternity and neonatal care.8
The role of UK ambulance services
Ambulance Service NHS Trusts are a provider of urgent and emergency health care across the UK. There are 13 ambulance trusts in the UK – 10 in England and one in each of Wales, Scotland and Northern Ireland. A unique branch of healthcare provision, ambulance services operate outside the boundaries of traditionalist health and care provider organisations, have a peripatetic identity and therefore operate in place – on-site, in primary, acute and community settings, across rural and urban areas and most importantly, in people’s homes. The ambulance service may be required to provide care at any point of the childbearing continuum to a woman or baby in any one of these locations.
While most planned births in the pre-hospital setting are uneventful,9 those that require the ambulance service are associated with adverse outcomes for women and babies.10-12 In addition, not all maternity calls to the ambulance service relate to birth; some of the most complex cases attended to in the pre-hospital setting relate to emergencies throughout the childbearing continuum and following birth.13 In addition, babies born across a range of gestations in the pre-hospital setting are at an increased risk of mortality and morbidity.5,14 Alongside the risks associated with unplanned birth and maternity emergencies in the pre-hospital setting, research has identified a lack of confidence and skills among pre-hospital clinicians in dealing with low and high acuity maternal and neonatal presentations.15,16 While there is limited research on outcomes for women who contact the ambulance service during the perinatal period, a recent report focused on maternity and perinatal outcomes highlights comorbidities and poor outcomes associated with not receiving care in the right place at the right time.17 Although only 1% of calls to the ambulance service relate to maternity and neonatal care, the calls are often high acuity with high stakes and have a big impact on patients and staff. In a recent data analysis for the Welsh Ambulance Service by the Maternal and Neonatal Safety Improvement Programme (MatNeoSIP), it was found that 10% of pregnant women in Wales access urgent or emergency care at some point during pregnancy.18
Pressures within and across health care are also resulting in a shift in how patients access and engage with health care. A recent report highlighted the increased demand placed on urgent and emergency care providers in the wake of the pandemic19 and the impact upon health disparities. Despite a focus on enhancing safety in maternity service provision, the notion of ‘displaced risk’, when women access urgent and emergency care outside of maternity pathways, contextualises presentations that are often attended to by the ambulance service.20 While a focus on enhancing maternity and neonatal care provision within acute settings is needed, system approaches that recognise the need for high quality care at every point of contact, and equitability in access to such care, is the focus of this special report.
Health inequalities and disparities in access to maternity and neonatal care
While pregnancy is considered a relatively low risk event for women in the UK, inequalities within maternal healthcare provision and care delivery remain an increased risk factor for maternity and neonatal morbidity and mortality.17 Over the last decade independent reports have highlighted numerous examples of persisting disparities that impact upon outcomes for the countries’ most vulnerable families.8,21 While some improvement in the delivery of neonatal specialist care was identified after reorganisation and implementation of NODNs,22,23 a persistent increase in complex pregnancies, inequalities in outcomes for black, Asian and minority ethnic women and those living in higher areas of deprivation24 has highlighted a need to focus on intersectional risk factors among perinatal populations. In a direct challenge to address health disparities, the NHS Core20PLUS5 report25 encouraged systems to adopt a public health approach to reducing inequalities in outcomes for women and babies.
As part of a national driver to improve health care for all, the ambulance service is focused on harnessing public health approaches to deliver prevention of ill health alongside its core business to deliver urgent, emergency and elective care.26 Public Health England in collaboration with The Association of Ambulance Chief Executives (AACE) released a discussion paper in 2021 focused on embedding a social value and social justice approach to care delivery, recognising the ambulance service as positively contributing to reducing health inequalities.27 An active system partner in addressing poorer health outcomes faced by black and ethnic minority communities, population and citizens across the multitude of health and care touchpoints, the ambulance service plays a vital role in driving forward national and regional agendas.
In the context of perinatal populations, calling emergency services during and following pregnancy is a gateway to seeking help and accessing maternity care, serving as a critically important indicator of risk. Calls to the ambulance service likely represent the fact that some women don’t know what else to do, or how to access care, particularly those from ethnic minority or migrant backgrounds.28 Understanding disparities in patient journey and accessing services with particular attention to additional vulnerabilities, such as being from ethnic minority, migrant or deprived backgrounds, is imperative to provide culturally safe and competent care to all.
Points raised warrant further exploration of what complications, concerns and needs women have when calling for an ambulance, and outcomes once they arrive at the obstetric or neonatal unit. A step in addressing such points is the appointment of midwives working within the ambulance service, serving as the dedicated link between providers and systems to tackle complex challenges relating to care provision and pathways into care.
Role of midwives in the ambulance service
Nursing and midwifery registrants are an asset to ambulance trusts, bringing diversity of knowledge and specialist expertise focused on a wide range of patient groups. As the ambulance service looks forward to the future of urgent and emergency care, the potential to develop further specialist roles within ambulance services to enhance care for different groups of patients is timely. In 2008, the London Ambulance Service was the first ambulance trust to employ a consultant midwife. This appointment highlighted the volume and acuity of maternity and neonatal incidents in the pre-hospital setting. The role has evolved to support training and development for staff alongside improvement of clinical governance in pre-hospital maternity care. Establishing the role has led to several quality improvement projects relating to policies, guidelines, service delivery and pathways. One example of this is the newborn assessment tool developed in the London Ambulance Service to standardise and support the pre-hospital assessment of newborn babies at birth (FIGURE 1).
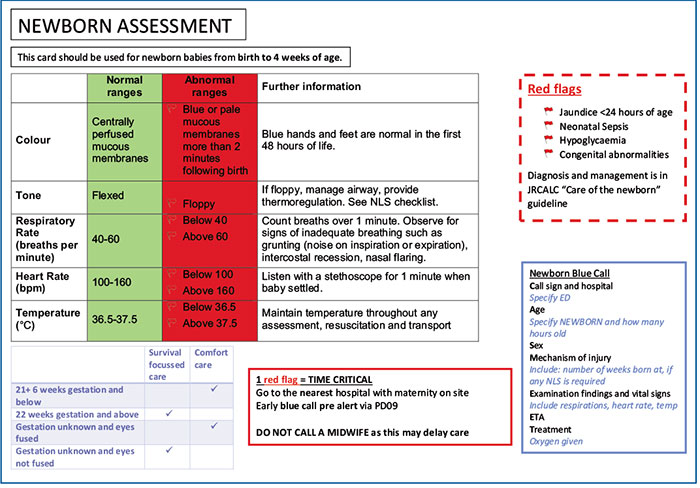
FIGURE 1 The newborn assessment tool developed in the London Ambulance Service to standardise and support the pre-hospital assessment of newborn babies at birth.
Despite proven benefits of the role, the appointment is relatively new with just four substantive consultant midwives currently appointed in ambulance trusts nationally. While many services do have a dedicated maternity lead, posts are often part-time and not consultant level. The consultant midwives in post act as a crucial conduit between urgent and emergency care provision and maternity and neonatal care providers. The role also allows the ambulance trust to contribute to the wider goals of local maternity and neonatal systems in improving accessibility, quality and safety of women and babies throughout the childbearing continuum.25
Considering the employment of a consultant midwife in an ambulance trust is crucial to oversee the provision of this specialist care by generalists (ambulance clinicians) and ensure that the ambulance service and maternity services collaborate to reduce risk and improve outcomes for mothers and neonates who require emergency care.29
Training and education
One aspect of collaboration that consultant midwives within ambulance trusts can be instrumental in delivering is multidisciplinary training. The message is clear, those who work, train and learn together undoubtedly support safer outcomes for patients.25 A focus on multidisciplinary team training is a key recommendation to enhance safe, effective care delivery.5,8 As part of the development of integrated care systems, a focus is placed on developing provider collaborations at scale.30 Despite such ambitious outputs, the ambulance service is rarely included in training and skills drills led by acute providers nor any standardisation within ambulance trusts of the level and frequency of training to deal with obstetric and neonatal emergencies.
Simulation-based training has been shown to improve staff experience of undertaking training and improving competence when dealing with actual clinical emergencies.31 Midwives in the London Ambulance Service and The North West Ambulance Service have initiated a training programme that involves bringing together ambulance clinicians and community midwifery teams to participate in simulation-based scenarios of emergency births and obstetric emergencies (FIGURE 2). The ambulance clinicians learn technical skills and an understanding of midwifery practice; it is also an opportunity to give hands-on maternity care in a safe environment. The community midwives benefit from training with the ambulance clinicians as it helps them to understand their scope of practice and it raises their awareness of the specific considerations required when delivering care outside of a hospital. A number of ambulance services across the UK have recently purchased the pre-hospital PROMPT (practical obstetric multi-professional training) package (www.promptmaternity.org), which focuses on up-skilling pre-hospital clinicians in the management of emergencies, in the absence of a midwife. A recent evaluation of pre-hospital PROMPT undertaken within the Northwest Ambulance Service highlights an increase in confidence and competence of clinicians who attend but acknowledges the limitation of exposure for staff to retain knowledge and skills taught on the day.

FIGURE 2 Simulation-based scenarios of emergency births and obstetric emergencies.
Sharing excellence: the development of the out-of-hospital newborn life support course
The Newborn Life Support (NLS) course was introduced in 1999, standardising the approach to management of a newborn baby. As a physiological-based, quality assured course, it is delivered and utilised internationally. However, despite assertions that NLS is for any healthcare professional involved in care of the newborn, it fails to address the issues and challenges that arise in out-of-hospital clinical practice. In the absence of a standardised approach, several groups have issued guidance suggesting best practice in this unique setting, but despite an increasing degree of collaboration, there have been no clear attempts to standardise training between organisations or healthcare professions. This has led to varying degrees of competence and comfort in out-of-hospital newborn care, particularly within the ambulance service.15 As such, a bespoke programme, targeted to the needs of the clinician working in the community, midwifery-led units or emergency services, was needed.
The challenges facing out-of-hospital clinicians are multifactorial and diverse. Staffing and resources are stretched, with assistance taking time to arrive and remote advice often being unavailable. A unique mix of healthcare professionals are brought together in the care of these babies, and the equipment available is variable, but consistent in its deviation from hospital standards. This influences the interventions that can be delivered or the way in which they are provided. Support to transition, which is the focus of NLS, is only the first aspect of out-of-hospital newborn care with the majority of infants subsequently requiring transport to hospital and ongoing care or observation during this period.
The out-of-hospital newborn life support course (OHNLS) was developed, in association with the Resuscitation Council UK (RCUK), by a multidisciplinary group consisting of paramedics, midwives and doctors. It was constructed around the core NLS principles acknowledging that the physiology of the newborn requires standardised management. However, the course material was carefully designed to ensure that differences in equipment, resources, staffing and the environment were addressed. OHNLS teaches optimal care of the newborn through developing expertise and nuance with the equipment available to the out-of-hospital practitioner. A new lecture is delivered on non-technical skills and team performance to improve the formulation and function ofad hoc teams between midwives, paramedics and other out-of-hospital clinicians. New scenarios were carefully written to reflect real life situations and allow paramedics and midwives to work collaboratively, with debriefs focusing on both the clinical care and team working. A new post-transition workshop was developed teaching assessment of the newborn, management of key adverse events, such as hypoxia and hypoglycemia, alongside discussing options for safe transport. Neonatal hypothermia is commonly described in this group of newborns32 and so thermal care is heavily emphasised throughout the course material. Guidance and best practice advice from individual organisations were integrated into the materials where appropriate. The final assessment mirrors NLS, with the same airway test followed by an adapted theoretical exam, reflecting core NLS material and additional teaching held within OHNLS.
The proof-of-concept courses for OHNLS ran in November 2022 and after adapting the material based on feedback from faculty and candidates, the pilot courses were delivered in September 2023. The course will now be rolled out across the country, with a focus on developing faculty and course centres as well as training OHNLS providers. Currently, candidates are provided with OHNLS supplementary material alongside the NLS manual, but with the guideline 2025 changes, it is anticipated that the ‘Birth outside the labour ward’ chapter of the NLS textbook will be updated with this supplementary material. A key aspect of improving the scalability of this course will also be the development of a new generic instructor course stream, which will allow a more sustainable growth of OHNLS.
While initiatives such as the OHNLS course can bring standardisation to the clinical care of newborns in the out-of-hospital setting, ambulance staff remain hampered in their efforts to deliver expert care to these infants due to variability in the equipment provided. As an example, a recent study from an ambulance trust in England found that the temperature of babies born out-of-hospital was recorded by paramedics in only 2.7% of cases.16 However, paramedics reported that appropriate thermometers were either unavailable or unsuitable alternatives were provided. Access to equipment for premature infants is particularly variable. Equipment variability is not limited to pre-hospital teams with community midwives also facing the same challenge.
The development of the OHNLS course will go some way towards addressing the variability in training and standards surrounding newborn care in this challenging setting. However, the course can only reach a small percentage of clinicians working in this environment, so more needs to be done to improve the education and continuing development of our out-of-hospital colleagues. The RCUK has recently updated its ‘Equipment used in homebirth’ list33 to reflect the practices advocated in the OHNLS course, and NHS England has also adapted its recommended load lists for ambulance trusts. These recom-mendations will hopefully influence the activity of services and procurement teams to ensure that clinical staff are appropriately equipped to manage a newborn of any gestation in the out-of-hospital setting. A vital area for further work is around the transport of newborns from the community, as the current lack of equipment and guidance may result in unsafe practices being displayed.
Neonatal transport services
Since 2004, neonatal services in the UK have been configured into Managed Clinical Networks.34 A key aspect of this was the centralisation of specialist neonatal intensive care to fewer centres and, alongside this, the designation of neonatal units into three core levels: special care units, local neonatal units and neonatal intensive care units.35 Centralisation for other specialisms such as endocrinology, surgery, cardiology, extracorporeal membranous oxygenation and hepatology are also seen on a regional and supra-regional level.
To support the effective functioning of these networks, dedicated neonatal transport services were commissioned in line with the NHS Neonatal Transport Service Specification.36 There are currently 14 transport services in the UK, which undertake approximately 15,000 transfers annually, uplifting neonates when a higher level of care is required and repatriating them after recovery.37 The majority of these are road transfers, with a small but increasing number being undertaken using rotary or fixed wing air ambulances. These transport teams are staffed by specialist nursing, medical and allied health professionals with 24/7 consultant availability for advice or clinical support on transfers. The equipment carried by the teams allows the initiation or continuation of intensive care, including targeted thermal control, invasive and non-invasive ventilation and infusions.
The funding and commissioning of neonatal transport teams is currently limited to the transfer of neonates into or out of a neonatal unit. There is no capacity or provision to respond to neonates born in the community setting, or for the support of the transfer of pregnant women between hospital facilities. The responsibility for the transport of these cases lies with the ambulance service and while it is unrealistic to expect the training of staff and the equipment available to equal that of transport teams, there are areas for improvement.
Exposure to pre-hospital birth is low for individual clinicians, resulting in a reduced level of confidence.15 This can be partially overcome through rapidly accessible and clear guidance alongside the availability of remote clinical support, neither of which is consistently available in the UK. A common area of uncertainty is the most appropriate destination, particularly when the newborn is undergoing life support or ongoing support to transition. The UK Ambulance Service Guidelines38 state that local protocols should be followed, reflecting the variability between systems. This introduces uncertainty and confusion in an already demanding situation, potentially resulting in newborns arriving at the wrong department and subsequently having a delay in receiving definitive care. A dedicated neonatal advice line could assist here, but none are currently available to UK ambulance staff.
The equipment available to transport infants is also variable and clear guidance around the safe transport of the newborn is lacking. Two commercial devices are used in the UK ambulance services, the NeoMate (Ferno) and the Ambulance Child Restraint (Paraid). Both offer a good solution to transporting well newborns from approximately 2kg, but the use of vital thermal control measures within the restraint system, such as a thermal mattress is not supported by the manufacturers. This is due to the crash-testing having only been completed with babies that are dressed and not wrapped for good thermal control. The lower limit of 2kg also precludes their use with smaller preterms. The KangooFix (Ferno), allows for transport of well newborns from 1kg while facilitating close contact with a parent for thermal care. This has been used safely and effectively in neonatal transport teams, but no ambulance trust in the UK has invested in this product.39 In the absence of appropriate equipment, particularly for unwell or preterm newborns, ambulance staff will continue to be faced with improvisation and pragmatic decision-making balancing risk and benefit when considering how best to safely transport a newborn from the out of hospital environment (FIGURE 3).

FIGURE 3 Premature baby (manikin) in the NeoMate harness.
Current pathway developments and opportunities
Several recent developments across systems in the UK have evidenced the impact of cross collaborative working on the standardisation of pathways in support of babies born in the right place. The suspected preterm labour pathway developed by SECAmb (South East Coast Ambulance Service) was designed to deliver babies to expert care taking into consideration the complexities of this decision making outside of hospital by ambulance clinicians (FIGURE 4). The early expertise of intensive care units is demonstrated to improve outcomes for this patient group. Additionally, babies born outside these specialist centres, will need to undergo an ex-utero transfer, which has been associated with adverse outcomes, as well as increased demand and 1:1 care by specialist teams. This pathway supports clinicians, reduces the need for ex-utero transfers and has been successfully implemented in the SECAmb area. However, careful clinical decision-making needs to be undertaken, acknowledging the risk versus benefit of prolonged travel times to intensive care units, particularly in more rural areas. This highlights the complex nature of pathway development and the clinical decision making required by paramedics to recognise a risky preterm labour presentation.
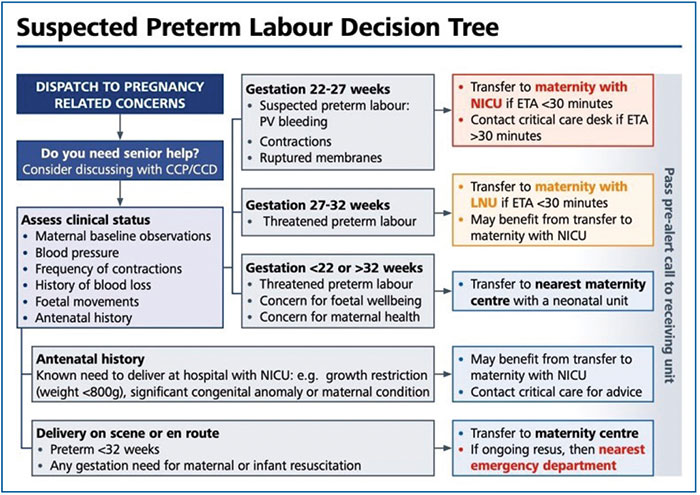
FIGURE 4 The SECAmb suspected preterm labour decision tree.
Final thoughts
The ambulance service and specialist neonatal transport services play a vital role in the emergency and urgent management and care of neonates, caring for some of the most vulnerable babies born at a range of gestations. NODNs and neonatal units who work collaboratively with their regional ambulance service have evidenced effective system approaches to ensuring appropriate pathways and commissioned services to ensure care delivery is prioritised. A national approach to considering the pre-hospital setting as a critical environment in which care is delivered, will support an expansion of service provisions and a true multidisciplinary approach (TABLE 1). The context of environment, the equipment available, the complexity of decision making and the psychological impact on ambulance clinicians has been highlighted. Care provided to neonates in the pre-hospital setting requires additional thought within and across healthcare systems to ensure the timely implementation of the neonatal critical care transformation review and the three-year plan for maternity and neonatal care.
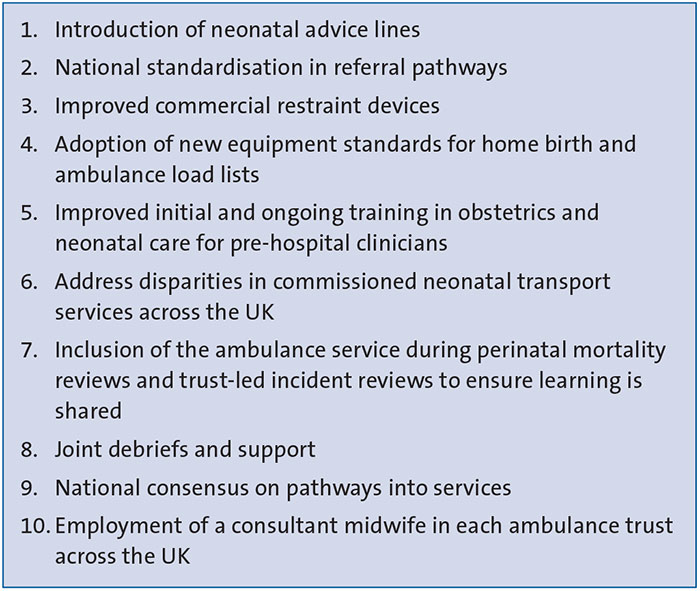
TABLE 1 System considerations to enhance care for neonates in the pre-hospital setting.
Or read this article in our
Tablet/iPad edition
