

Is cuffed endotracheal intubation in neonates a safe practice?
Endotracheal intubation and ventilation for respiratory insufficiency is a common procedure in preterm and sick infants. Traditionally, uncuffed endotracheal tubes (ETTs) are used in neonatal units, however the use of cuffed ETTs is on the increase, despite the limited evidence. This literature study reviews the evidence available on the safety of cuffed versus uncuffed ETTs for respiratory support in neonates by examining the risk of post-extubation stridor and the need for re-intubation.
Femi Adeniyi
Neonatal Consultant
Neonatal Intensive Care Unit, East Lancashire Hospitals NHS Trust
femi.adeniyi@nhs.net
Kunle Oyedokun
Paediatric Consultant
Ormskirk Neonatal Unit, Mersey and West Lancashire Teaching Hospitals NHS Trust
Adeniyi F., Oyedokun K. Is cuffed endotracheal intubation in neonates a safe practice? Infant 2023; 19(4): 145-48.
Background
Traditionally, uncuffed endotracheal tubes (ETTs) are used for endotracheal intubation and ventilation for respiratory insufficiency in neonates and young infants on neonatal units, however, the use of cuffed ETTs is increasingly seen, despite limited evidence for or against their use. The cuff is an inflatable balloon at the distal end of the ETT that can be inflated after insertion of the ETT in the airway. The cuff seals against the tracheal wall to reduce gas leaks and prevent aspiration of gastric contents and accidental extubation.
Over recent years there has been a move towards the use of cuffed ETTs in infants and children in operating theatres and paediatric intensive care units (PICUs).1 However, a short survey (unpublished) conducted by the authors in the Northwest region of England revealed that no neonatal units keep a stock of neonatal cuffed ETTs or use cuffed ETTs. This differs from the PICU in the same region, which reported that cuffed endotracheal intubation remains the standard practice for neonates requiring intubation in paediatric intensive care. In our region, the neonatal unit collaborates with the Northwest UK tertiary surgical neonatal centre for those neonates requiring further care at a neonatal surgical centre. Post-operatively most surgical neonates are admitted to the PICU from theatre with a cuffed ETT and continue with it. In the event of transfer to a neonatal unit post-operatively, most neonatal units either deflate the balloon or change the ETT because of confidence in their usual practice, given that staff have had no previous training on the safety and usefulness of cuffed ETTs in neonates.
The deflation of the balloon when transferred to the neonatal unit can cause leakage around the ETT, leading to inadequate ventilation and sometimes a further procedure to upsize the ETT using sedation and muscle relaxant.2
This variation in practice between neonatologists, PICU staff and anaesthetists raises the need to provide consensus on the safety and usefulness of cuffed ETTs in the neonatal population.
Cuffed vs uncuffed ETTs
Historically, uncuffed ETTs were used in infants and toddlers because of differences in anatomy between adults and small children. There is general belief that uncuffed ETTs should provide a sufficient seal at a peak inspiratory pressure (PIP) of 20-25cmH2O, making a cuffed ETT unnecessary.3,4 The rationale for the use of a cuffed ETT is to provide an effective airway seal while minimising pressure around the cricoid. However, in children the entire cuff should be located distal to the cricoid ring following intubation to avoid injury to the subglottic structures.1
Improved understanding of the anatomy of the neonatal airway has played a role in the increased use of cuffed ETTs in the neonatal population. Research into paediatric and neonatal airways using imaging and direct bronchoscopy suggests that the airway is elliptical, rather than round.5 This might present a higher chance of uncuffed ETT leakage in the ventilated patient, despite using one with an appropriate diameter for age.5,6
There are several advantages of cuffed over uncuffed ETTs. Cuffed ETTs have enhanced efficacy in sealing the airway and permit improved control of ventilation/ oxygenation and higher ventilation pressures in patients. Cuffed ETTs better protect against aspiration and they are more flexible in terms of sizing – changing an ETT can be avoided when too small a tube is initially inserted by subtle adjustments in the inflation of the balloon. However, cuffed ETTs have disadvantages too. Use of a cuff may risk tracheal mucosal injury due to pressure from the cuff itself (especially with the longer elliptical cuffed tubes due to risk of herniation through the epiglottis).7 The price of the cuffed ETT can be twice as high as the uncuffed ETT.8 When in use, the cuff pressure should be monitored frequently to avoid aspiration and tracheal injury. Furthermore, the higher pressure and extended length of the cuffed part may cause pressure necrosis. To avoid this complication, micro-cuffed low-pressure high-volume ETTs have been developed.9 Yet, despite this improved knowledge and technical progress, there is no consensus on the superiority of cuffed over uncuffed ETTs in neonates.10
The literature search
This literature study reviews the evidence available between May 2012 and May 2022 on the safety of cuffed versus uncuffed ETTs for respiratory support in neonates. The review aims to examine the risk of post-extubation stridor and the need for re-intubation in neonates intubated with cuffed versus uncuffed ETT.
The key search terms used to search the PubMed, Embase and Cochrane databases were: neonates OR preterm babies OR premature babies OR term babies AND endotracheal airway OR endotracheal intubation OR cuffed endotracheal airway.
A preliminary search showed that the use of cuffed endotracheal intubation in the neonatal population is a recent practice and that the decade, May 2012 to May 2022, would capture the extension of the practice into neonatal medicine. Research prior to this date range was excluded.
Peer-reviewed journals were the primary source of research, with consideration given to the more academic rather than descriptive ones. Neonates and infants with weights of up to 5kg were included, with the aim of capturing newborns that may be large for gestational age at birth.
The most recent Cochrane review in 202211 examines the benefits and harms of cuffed ETT for respiratory support in neonates. The limitation of the review is that it only identified one eligible randomised controlled trial (RCT) for inclusion that compared the use of cuffed versus uncuffed ETT.12 This RCT had a small sample size and reflects the lack of study in this area of neonatal medicine.
Our critical review will include other articles published before and after the 2022 Cochrane review.
The articles selected for critical appraisal
Four quantitative research studies were selected to answer the research questions (Table 1). Three of these are retrospective cohort studies.13-15 The fourth is an RCT.12
A quality assessment was performed using the Critical Appraisal Skills Program (CASP) tool for cohort studies and an RCT checklist was applied.16 The CASP tool is commonly used in health care critical appraisal with the endorsement of the Cochrane Qualitative and Implementation Methods Group.17
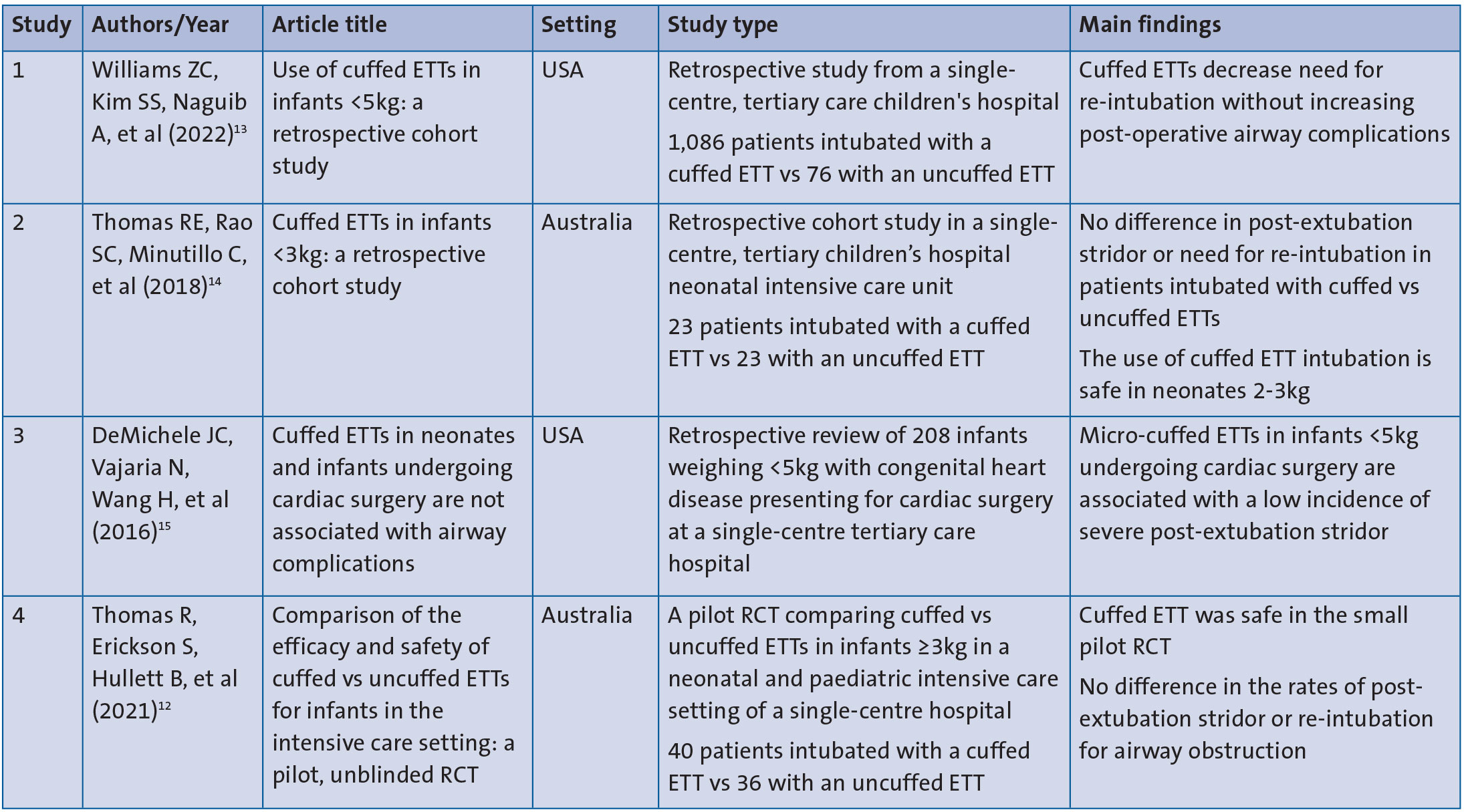
TABLE 1 The four quantitative research studies selected for critical appraisal.
The appraisal
The following sections concern the appraisal of the four research studies identified in the literature search.
Study design
Study 4 was the only RCT, the remaining three studies being retrospective cohort studies. An RCT represents a level 1 hierarchy of evidence, compared to a cohort study, which is at a level 3 hierarchy of evidence.18 The RCT utilises a blinded randomisation tool to allocate patients into cuffed and uncuffed ETT groups, which reduces the bias that was likely in the other three cohort retrospective studies.19 However, the limitation of study 4 was that it involved only a small sample size of 76 neonates, which is consistent with an ongoing lack of adequate recruiting into neonatal research in high income countries.20 Comparatively, studies 1 and 3 have the advantages of a larger sample size and the non-requirement of consent because of their retrospective cohort nature.
Population
The four studies were from developed countries (Australia and the USA), where the standard of care for neonates is similar to a UK setting. However, the review provided the outcomes from the study from both the anaesthesiology and neonatal intensive care point of view. For instance, studies 1, 2 and 3 showed peri-operative intubation practice outcomes of the anaesthesiology team, as opposed to study 4, which reviewed the practice in the neonatal intensive care population. This created variation in the patient and expert populations represented and a need for caution in interpreting the results. Also, studies 1, 2 and 3 represent groups ventilated by anaesthetists and paediatric intensivists with a shorter ventilation period compared to the neonatal population in study 4, where the patients were in neonatal units and more likely to require a prolonged ventilation period.19
It is imperative to emphasise that the subset requiring cardiopulmonary bypass (CPB) for high-risk surgery has a higher risk of stridor that is independent of either intubation with cuffed or uncuffed ETT. Hence, a meaningful comparison between neonates intubated with cuffed and uncuffed ETTs is impossible when evaluating the subset of patients presenting for high-risk surgeries, including cardiac surgery, as seen in studies 1 and 3.13,15 Furthermore, the need for racemic epinephrine in the subset of patients who had cardiac surgery and CPB compared to the non-cardiac surgery group, agrees with previous reports of a similar incidence of post-extubation airway concerns in patients who had surgery for congenital heart disease (CHD) rather than patients who underwent non-cardiac surgical procedures.
Methodology
A critical review of methodology is paramount as methodology forms the basis of a good study.21 A previous study emphasised the marked variations in different manufacturers’ neonatal cuffed ETTs and some poorly designed neonatal cuffed ETTs.22 Hence, the introduction of high-volume, low-pressure micro-cuffed ETTs with better sealing and a cuff-free subglottic zone is an improvement in cuffed ETTs.23 Therefore, it is essential to state that there were differences in the manufacturers of the cuffed ETTs used in the studies, with risk of bias. The cuffed ETTs used in the four studies were the Halyard Microcuff (Avanos Medical, Alpharetta, Georgia, USA) and Kimberly-Clark Microcuff ETT (Kimberly-Clark, Roswell, Georgia, USA), which are both high-volume low-pressure cuffed ETTs. No data are available to discuss the relationship of the cuff to the subglottic zone.
The four studies involved in the review neither stated the guidance used in monitoring pressure of the cuffed ETT nor provided information regarding the level of training provided to the multi-disciplinary teams looking after the patients. Moreover, post-ETT extubation stridor as a complication following intubation can be subjective. This may explain why the data on stridor varied in all four studies, including documentation of stridor and need for dexamethasone or adrenaline treatment. However, the retrospective cohort studies enable achievement of a large sample size but with the risk of recall bias, which was not fully addressed in the published articles.24
Results
Study 1 is one of the three cohort studies and has the largest number of recruits over a three-year period; 1,086 patients received cuffed ETTs (compared to 76 with an uncuffed ETT) suggesting that this might be standard practice in the study centre.13
Study 2 reported no significant differences between uncuffed and cuffed ETT in neonates up to 34 weeks’ gestation and weight as low as 2.62kg, with regards to changing the ETT to find the correct size.14 In addition, the study 4 pilot RCT agreed that using cuffed ETT in neonates from 35 weeks’ gestation reduced the need for upsizing the ETT. However, study 4 reported that the cohort with uncuffed ETT was significantly more likely to require re-intubation to find the correctly-sized ETT or re-intubation at any time during the ventilation period.12
Study 4 showed no significant differences in the rates of post-extubation stridor, post-extubation dexamethasone, post-extubation nebulised adrenaline, nor re-intubation for airway obstruction. However, the cohort in the cuffed ETT had a shorter duration of time on the ventilator compared to the uncuffed cohort and a reduction in atelectasis. Furthermore, in study 2, two of the 23 cuffed cohort of patients received pre-extubation steroids as prophylaxis after they had cuffed ETT for eight and 17 days, respectively.
There was an increased incidence of stridor in post-operative cardiac surgery patients without bypass that were intubated with cuffed ETT in study 1.13 The cause of the stridor was attributed to cardiac or respiratory insufficiency. Similarly, study 3 reported increased incidence of post-extubation stridor in post-cardiac surgery patients with cuffed ETT; the group emphasised that co-morbidity was significantly associated with stridor.15
Discussion
The main findings were that cuffed ETT could be helpful in the target neonatal population from 35 weeks’ gestation and birth weight of 2kg. However, there is limited or no information on the use of cuffed ETTs in neonates of <35 weeks’ gestation and <2kg. The micro-cuffed ETT commonly used throughout this review is size 3.0 (the smallest size available); two neonates had a larger size 3.5 cuffed ETT across the four studies.
The retrospective cohort studies demonstrate no significant difference in post-extubation stridor or need for re-intubation between the uncuffed and cuffed ETT intubated neonates. This was similar to findings in the RCT, which showed no difference in the risk of post-extubation stridor between patients with cuffed or uncuffed ETT. However, the RCT emphasised that neonates intubated with uncuffed ETTs risk needing re-intubation, usually to ascertain the correct ETT size for adequate ventilation.
It is essential to emphasise that this review noted the high risk of post-extubation stridor in neonates that under-went cardiac surgery. The incidence of stridor was similar in both cuffed and uncuffed ETT intubated neonates post-cardiac surgery and this was attributed to the possibility of traction during surgery and respiratory or cardiac insufficiency, as opposed to endotracheal intubation.
The previous disadvantages of a cuffed ETT, such as the safety around monitoring of the cuff pressure and the high risk of tracheal mucosa injury, were not identified in this review.7
Limitations
The limitations of retrospective studies, such as lack of training and inadequate definition of recorded outcomes, reduce the validity of the outcomes recorded. Nevertheless, a prospective study will objectively determine post-extubation airway complications and their association with patient variables and, possibly, compare the complication rates between cuffed and uncuffed ETTs in this high-risk population. It will be beneficial to have a multidisciplinary involvement in a future RCT multi-centre study design.
Conclusion
This literature review provides information about the safe use of cuffed ETTs in neonates >35 weeks’ gestation weighing >2kg. The studies demonstrate no difference in the risk of post-extubation stridor or re-intubation using cuffed versus uncuffed ETTs. However, data are limited and there is need for a well-designed multi-centre RCT to establish any other benefits/harms of cuffed versus uncuffed ETTs.
Acknowledgement
The authors are grateful to the following colleagues for help with reviewing the content of the article:
Christopher Ugwu, Paediatric Registrar, Wirral University Teaching Hospital NHS Foundation Trust.
Sanjeev Rath, Neonatal Consultant, Wirral University Teaching Hospital NHS Foundation Trust.
Ambrose Onibere, Neonatal Consultant, Glan Clywd Hospital.
Shri Babarao, Neonatal Consultant, Liverpool Women’s NHS Foundation Trust.
Or read this article in our
Tablet/iPad edition
- Unlike paediatric care, neonatal units commonly use traditional uncuffed ETTs rather than cuffed ETTs.
- Cuffed ETTs may offer some benefits over uncuffed ETTs but are they safe for use in neonates?
- This literature review provides information about the safe use of cuffed ETTs in neonates.
- The available studies are limited but the critical appraisal demonstrates no difference in the risk of post-extubation stridor or re-intubation using cuffed versus uncuffed ETTs.
Also published in Infant:
