

A novel technique for umbilical artery catheter insertion in neonates
Ahmed Yousef
Locum Neonatal Consultant, City Hospital Birmingham, Sandwell and West Birmingham NHS Trust (orcid.org/0000-0001-5009-1631)
ahmed.yousef3@nhs.net
Yousef A. A novel technique for umbilical artery catheter insertion in neonates. Infant 2023; 19(2): 71.
Umbilical arterial catheters (UAC) are frequently placed in neonates who need invasive haemodynamic monitoring or frequent blood sampling/blood gas analysis; however, insertion can be a challenging procedure. The umbilical artery has a tiny diameter and contracts quickly after transection, which makes catheterisation difficult and often unsuccessful.
This new method for UAC insertion is quick and simple. It takes advantage of the observation that the umbilical artery is surrounded by Wharton’s jelly, a gelatinous material that will immobilise the umbilical artery when some pressure is applied.
The technique
The umbilical cord should be cut in a straight and even manner. Quickly hold the cord distally with a piece of gauze surrounding the cord to prevent it from slipping. Identify and locate one of the umbilical arteries and make gentle and firm bilateral compressions on the cord with one hand to immobilise the artery. The artery will be supported by the surrounding Wharton’s jelly. With the other hand, hold the catheter at about 0.5-1cm from the tip, and then perpendicularly insert the tip into the lumen of the artery using gentle pressure initially to open up the arterial lumen until the tip passes through for about 1-2cm. Following this, slowly advance the catheter to the pre-determined length (FIGURES 1-3). Secure and verify the position using traditional procedures.
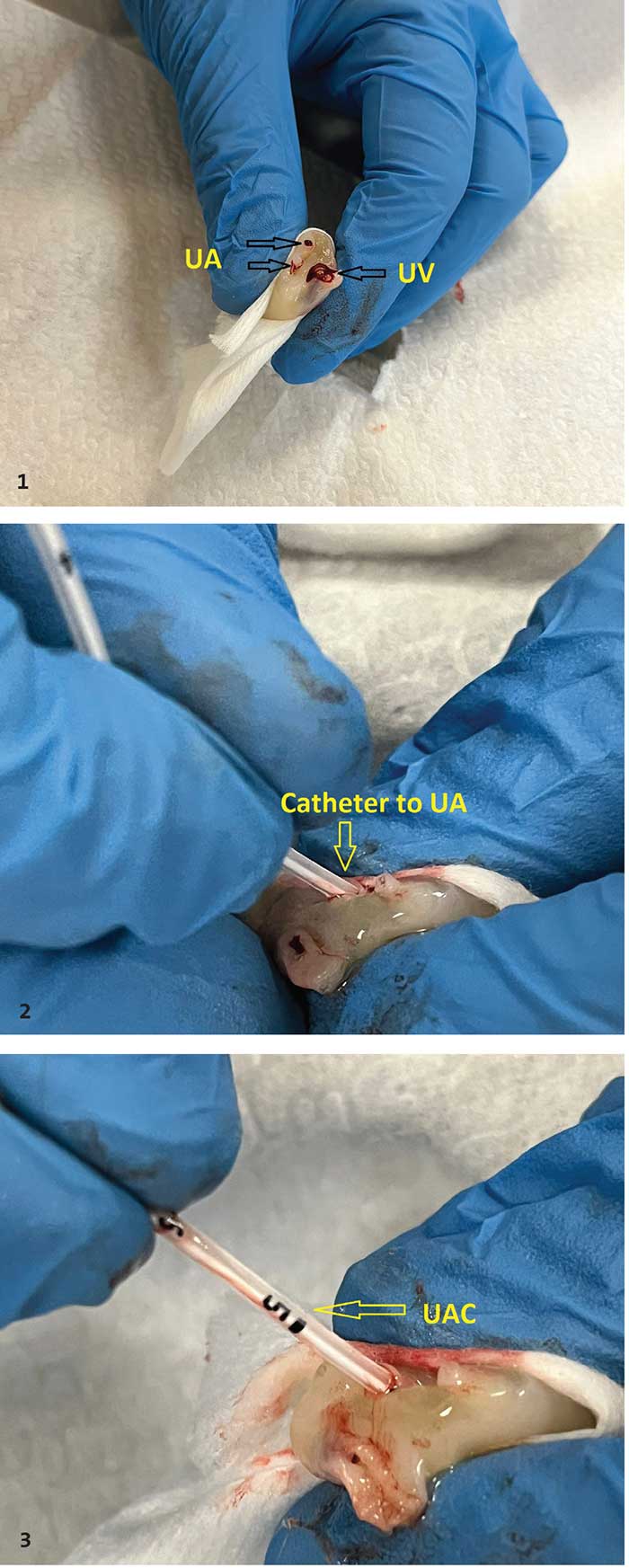
FIGURES 1-3 The stages of UAC insertion. (1) Holding the cord distally with a piece of gauze, make compressions to immobilise the artery. (2) Holding the catheter at about 0.5-1cm from the tip, insert the tip perpendicularly into the artery using gentle pressure until it passes through the lumen for about 1-2cm. (3) Slowly advance the catheter to the pre-determined length. Key: UA=umbilical arteries; UV=umbilical vein; UAC= umbilical arterial catheter.
I have used this technique overseas (Saudi Arabia, level 3 neonatal unit) and in the UK (level 2 and 3 neonatal units), on preterm and term infants ranging from 22-40+ weeks’ gestation (approximately 35 cases). In my experience, this method is quicker and more successful than conventional techniques. Furthermore, it does not require the assistance of a second practitioner and avoids the use of mosquito forceps and dilators. Dilators can cause false passage in the umbilical artery, which can result in a failed catheter insertion. There is currently a national shortage of UAC dilators and use of this technique should reduce demand and be more cost effective.
Staff training for the new technique will be implemented at City Hospital Birmingham along with a trial and audit to evaluate feasibility of this new technique.
Acknowledgement
Fresh umbilical cord has been used for the demonstration with verbal consent from the parents. Special thanks to Nancy Sakaya (Paediatric Trainee ST1) for help getting the umbilical cord and the photography.
Or read this article in our
Tablet/iPad edition
